You might also like
- Parathyroid Glands: Presented By: Dr. Mohammed Alshehri Pgy2Document28 pagesParathyroid Glands: Presented By: Dr. Mohammed Alshehri Pgy2Omar Alruwaili100% (1)
- Handbook of DermatologyDocument235 pagesHandbook of DermatologyNicholas MiteiNo ratings yet
- Electrolytes TableDocument4 pagesElectrolytes TableMeg NoriegaNo ratings yet
- Grabovoi NumbersDocument25 pagesGrabovoi Numberssorin6186% (14)
- 10 Topnotch Obstetrics Gynecology SuperExam1 PDFDocument84 pages10 Topnotch Obstetrics Gynecology SuperExam1 PDFvardhan100% (3)
- Uworld NotesDocument12 pagesUworld NotesTush Rame100% (1)
- Parathyroid Disorders I. HyperparathyroidismDocument4 pagesParathyroid Disorders I. HyperparathyroidismAllene PaderangaNo ratings yet
- Epoetin AlfaDocument2 pagesEpoetin AlfaIzell Lee100% (2)
- Hyperparathyroidism and HypoparathyroidismDocument44 pagesHyperparathyroidism and Hypoparathyroidismshweta singhNo ratings yet
- D E R M: Litt'sDocument706 pagesD E R M: Litt'sshintaNo ratings yet
- Calcium Homeostasis: Endocrine Regulation of (Ca)Document4 pagesCalcium Homeostasis: Endocrine Regulation of (Ca)PRANAB KUMAR MUKHERJEENo ratings yet
- ExamDocument8 pagesExamkrull243No ratings yet
- Hyperparathyroidism Concept MapDocument2 pagesHyperparathyroidism Concept MapDeo FactuarNo ratings yet
- Dispensing, Incompatibilities, and Adverse Drug Reactions Answer Key-PINK PACOPDocument78 pagesDispensing, Incompatibilities, and Adverse Drug Reactions Answer Key-PINK PACOPBilly Vince AlquinoNo ratings yet
- Angiography (Cardiac Catherization) : Patient Teaching/preparationDocument2 pagesAngiography (Cardiac Catherization) : Patient Teaching/preparationpsyNo ratings yet
- High Risk NewbornDocument8 pagesHigh Risk NewbornKath ArabisNo ratings yet
- Disorders of Parathyroid Gland: BY: Dr. Rakesh Dr. Karthik Dr. Soumya BY: Dr. Rakesh Dr. Karthik Dr. SoumyaDocument59 pagesDisorders of Parathyroid Gland: BY: Dr. Rakesh Dr. Karthik Dr. Soumya BY: Dr. Rakesh Dr. Karthik Dr. SoumyaAirdorid LoginidNo ratings yet
- Brand Name Generic Name Indication and Contraindication Nursing Consideration Action of The Drug Dose and Administration Side EffectsDocument2 pagesBrand Name Generic Name Indication and Contraindication Nursing Consideration Action of The Drug Dose and Administration Side EffectsCarla Dana GozumNo ratings yet
- Medications and Nursing ResponsibilitiesDocument6 pagesMedications and Nursing ResponsibilitiesDarla JoyceNo ratings yet
- Pediatric Endocrinology Part 2: Pediatrics 2Document8 pagesPediatric Endocrinology Part 2: Pediatrics 2sarguss14No ratings yet
- OsteoporosisDocument2 pagesOsteoporosistjelongNo ratings yet
- Endocrine Part 2 DRAFTDocument6 pagesEndocrine Part 2 DRAFTPreeti Joan BuxaniNo ratings yet
- Hypocalcemia Metabolic Bone Disease Joint DisorderDocument11 pagesHypocalcemia Metabolic Bone Disease Joint DisorderLlewelyn AgpaoaNo ratings yet
- Milk FeverDocument78 pagesMilk FeverAsif AliNo ratings yet
- ElectrolyteDocument4 pagesElectrolyteRon Vien'sNo ratings yet
- Hyperparathyroidism 170629131536Document48 pagesHyperparathyroidism 170629131536usmanNo ratings yet
- Downer CowDocument80 pagesDowner Cowavijaymba808No ratings yet
- Opposite To K (Potassium) Seizure: Electrolytes Normal Values Function Hypo Hyper Na (Sodium) 135-145 Meq/LDocument2 pagesOpposite To K (Potassium) Seizure: Electrolytes Normal Values Function Hypo Hyper Na (Sodium) 135-145 Meq/LEben Ezar Dela CruzNo ratings yet
- LEC 3 Parathyroid Gland DisordersDocument39 pagesLEC 3 Parathyroid Gland Disordersalhusien.abd2000No ratings yet
- WEEK 9 Disorders of The Parathyroid GlandsDocument2 pagesWEEK 9 Disorders of The Parathyroid GlandsJiro MarianoNo ratings yet
- Disorders of Parathyroid Gland: by DR Irum Siddiquie PGR PediatricsDocument54 pagesDisorders of Parathyroid Gland: by DR Irum Siddiquie PGR PediatricsJamesNo ratings yet
- II. Electrolyte Imbalance: By: Yves Mariel A. Rimando, RN, MN, CNNDocument66 pagesII. Electrolyte Imbalance: By: Yves Mariel A. Rimando, RN, MN, CNNczeremar chanNo ratings yet
- Fe 3Document43 pagesFe 3api-3697326No ratings yet
- Benjamin Button - 56Document97 pagesBenjamin Button - 56Aubrey Unique EvangelistaNo ratings yet
- HPT DDX (Sarah)Document3 pagesHPT DDX (Sarah)Maisarah RepinNo ratings yet
- Hypercalcemia (F&e)Document3 pagesHypercalcemia (F&e)Sarah Grace CajucomNo ratings yet
- Calcium: HypercalcemiaDocument7 pagesCalcium: HypercalcemiaGregNo ratings yet
- Hyper para Thyroid Is MDocument3 pagesHyper para Thyroid Is MAriefNo ratings yet
- Men1, Gi Endo Cam304 2019 J.burgessDocument27 pagesMen1, Gi Endo Cam304 2019 J.burgessJeffrey XieNo ratings yet
- Hyper Parathyroid IsmDocument20 pagesHyper Parathyroid IsmPartha SarathyNo ratings yet
- Potassium Supplements ParenteralDocument3 pagesPotassium Supplements Parenteralcarl meiNo ratings yet
- Wk8 - Electrolyte Imbalances & Acid-Base ImbalancesDocument65 pagesWk8 - Electrolyte Imbalances & Acid-Base ImbalancesPotato PceeNo ratings yet
- Case PresentationDocument20 pagesCase PresentationkaleeswariNo ratings yet
- Top 5 Causes of Passive Cervical FlexionDocument7 pagesTop 5 Causes of Passive Cervical FlexionCabinet VeterinarNo ratings yet
- Hypocalcemia: Julie Allen, BVMS, MS, MRCVS, Dacvim (Saim), DacvpDocument1 pageHypocalcemia: Julie Allen, BVMS, MS, MRCVS, Dacvim (Saim), DacvpElenaNo ratings yet
- Chapter54 Management of Patients With Kidney DisordersDocument40 pagesChapter54 Management of Patients With Kidney Disordersjericho dinglasanNo ratings yet
- Fluids and ElectrolyteDocument16 pagesFluids and ElectrolytechijklNo ratings yet
- Calcium Gluconate: (Kal-See-Um Gloo-Koh-Nate)Document3 pagesCalcium Gluconate: (Kal-See-Um Gloo-Koh-Nate)govind_soni_15No ratings yet
- HypercalcaemiaDocument10 pagesHypercalcaemiaKav RajapNo ratings yet
- ThyroidDocument6 pagesThyroidvmvlivNo ratings yet
- CT 7Document6 pagesCT 7Shaine TeodoroNo ratings yet
- HYPERCALCAEMIADocument4 pagesHYPERCALCAEMIAaizatamlikhaNo ratings yet
- HYPERPARATHYROIDISMDocument1 pageHYPERPARATHYROIDISMPhilip Gene II MalacasNo ratings yet
- Parathyroid GlandDocument18 pagesParathyroid Glandasish kpNo ratings yet
- Hypoparathyroidism: DR Ranganath N Professor Department of OrthopaedicsDocument33 pagesHypoparathyroidism: DR Ranganath N Professor Department of Orthopaedicsnandhana s nairNo ratings yet
- ElectrolytesDocument5 pagesElectrolytesChariza Trompeta100% (1)
- Fluid and Electrolytes: Dr. Nupur SarkarDocument24 pagesFluid and Electrolytes: Dr. Nupur SarkarNupurshinjiniNo ratings yet
- Calcium Gluconate Drug StudyDocument4 pagesCalcium Gluconate Drug StudyAngelou Joefred CongresoNo ratings yet
- Extranotes MedsurgDocument2 pagesExtranotes MedsurgIRA MONIQUE CABADENNo ratings yet
- Potassium ChlorideDocument2 pagesPotassium ChlorideAinaB ManaloNo ratings yet
- Rickets Metabolic Bone DiseasesDocument61 pagesRickets Metabolic Bone DiseasesKrameshNo ratings yet
- Preeclampsia EclampsiaDocument10 pagesPreeclampsia EclampsiajasphergliponeoNo ratings yet
- Fe 2Document26 pagesFe 2api-3697326No ratings yet
- Rickets & Osteomalacia: Suresh DhakarDocument51 pagesRickets & Osteomalacia: Suresh DhakarsandipkumarrayNo ratings yet
- Metabolic Bone Disease PDFDocument50 pagesMetabolic Bone Disease PDFAdNo ratings yet
- KaliumDocument2 pagesKaliumJustine Kaye Iballa HarligaNo ratings yet
- Surgical Diseases of The Parathyroid GlandsDocument34 pagesSurgical Diseases of The Parathyroid Glandsanand787No ratings yet
- ParkinsonsDocument2 pagesParkinsonspsyNo ratings yet
- Anaphylactic Shock Due To Contrast Dye Allergy HF Due To Left Ventricle Damage and MIDocument3 pagesAnaphylactic Shock Due To Contrast Dye Allergy HF Due To Left Ventricle Damage and MIpsyNo ratings yet
- ParkinsonsDocument2 pagesParkinsonspsyNo ratings yet
- ECG Description:: Ventricular FibrillationDocument2 pagesECG Description:: Ventricular FibrillationpsyNo ratings yet
- Physiological Integrity: Draw A Quick Concept Map Comparing Right Vs Left Heart FailureDocument1 pagePhysiological Integrity: Draw A Quick Concept Map Comparing Right Vs Left Heart FailurepsyNo ratings yet
- Myasthenia GravisDocument2 pagesMyasthenia GravispsyNo ratings yet
- List, Prioritize, Discuss Care For Patients Suffering An Acute Critical Neuro Emergency. Pick A Condition From This Chapter. and Create A Quick Concept MapDocument2 pagesList, Prioritize, Discuss Care For Patients Suffering An Acute Critical Neuro Emergency. Pick A Condition From This Chapter. and Create A Quick Concept MappsyNo ratings yet
- Neuro AgingDocument1 pageNeuro AgingpsyNo ratings yet
- Gather Patient HistoryDocument1 pageGather Patient HistorypsyNo ratings yet
- Nutrition Self-Monitored Blood GlucoseDocument3 pagesNutrition Self-Monitored Blood GlucosepsyNo ratings yet
- ATI Flash Cards 10, Medications Affecting Digestion and NutritionDocument22 pagesATI Flash Cards 10, Medications Affecting Digestion and NutritionSue PadgettNo ratings yet
- Radiology Presentation FinalDocument45 pagesRadiology Presentation FinalKhupe KafundaNo ratings yet
- Non-Communicable Disease Prevention and Control: Jennifer S. Cruel, RN, MNDocument65 pagesNon-Communicable Disease Prevention and Control: Jennifer S. Cruel, RN, MNChoi D. CruelNo ratings yet
- DIabetic REtinopathyDocument34 pagesDIabetic REtinopathyLuqman Khan YousafXaiNo ratings yet
- Chemical Coordination and IntegrationDocument12 pagesChemical Coordination and Integrationdlotlikar767No ratings yet
- RiumDocument3 pagesRiumDastinAndreNo ratings yet
- Narrative Pathophysiology of Varicose VeinsDocument2 pagesNarrative Pathophysiology of Varicose VeinsKim SunooNo ratings yet
- HyperlipidemiaDocument33 pagesHyperlipidemiaHimaNo ratings yet
- 09-28-15 CAH Grand RoundsDocument55 pages09-28-15 CAH Grand Roundsnila sari batubaraNo ratings yet
- MetabolismDocument16 pagesMetabolismAdiShineNo ratings yet
- T UptakeDocument3 pagesT UptakeModestus100% (1)
- 3 - SDocument45 pages3 - SFarnoush ShahriariNo ratings yet
- Adverse Effects and Safety of SGLT-2 Inhibitors: Diabetes & Metabolism December 2014Document8 pagesAdverse Effects and Safety of SGLT-2 Inhibitors: Diabetes & Metabolism December 2014Sahrul RiadiNo ratings yet
- Barbiturate PoisoningDocument3 pagesBarbiturate PoisoningDrDeepak Pawar100% (1)
- PulseDocument43 pagesPulseAngelo LacisteNo ratings yet
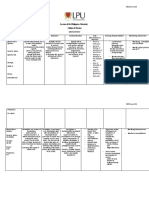
- Lyceum of The Philippines University College of Nursing: MCN Form 014Document3 pagesLyceum of The Philippines University College of Nursing: MCN Form 014twinkleNo ratings yet
- Case ReportDocument78 pagesCase ReportYuniarso Adi NugrohoNo ratings yet
- Zincum ValerianicumDocument3 pagesZincum ValerianicumKamalNo ratings yet
- Oral Pathology Hereditary Conditions: Group IDocument74 pagesOral Pathology Hereditary Conditions: Group IFatima CarlosNo ratings yet
- Laporan Kimia Farma Maros 2 MeiDocument14 pagesLaporan Kimia Farma Maros 2 MeiSitti AsiaNo ratings yet
- Te Trap LegiaDocument8 pagesTe Trap LegiasakuraleeshaoranNo ratings yet
- MUHS OBG SylabusDocument10 pagesMUHS OBG SylabusnavneetmagonNo ratings yet