You might also like
- Head TraumaDocument92 pagesHead TraumaRezaNo ratings yet
- Vitamin E - Dr. Wilfrid E. Shute's Complete Updated Vi - Shute, Wilfrid E., 1907Document236 pagesVitamin E - Dr. Wilfrid E. Shute's Complete Updated Vi - Shute, Wilfrid E., 1907Anonymous gwFqQcnaX100% (2)
- Cardiac Surgery MCQDocument43 pagesCardiac Surgery MCQprofarmah100% (7)
- STROKE: Handbook with activities, exercises and mental challengesFrom EverandSTROKE: Handbook with activities, exercises and mental challengesNo ratings yet
- 3&4&5-Assessment of Peripheral Vascular SystemDocument43 pages3&4&5-Assessment of Peripheral Vascular SystemKhaled Mohamed AssemNo ratings yet
- Rheumatology - Dr. Allam 2021Document33 pagesRheumatology - Dr. Allam 2021mohamedeen hamzaNo ratings yet
- Goat Medicine and SurgeryDocument393 pagesGoat Medicine and Surgerydrum75% (4)
- Stupor and Coma in AdultsDocument23 pagesStupor and Coma in AdultsFdo RMNo ratings yet
- MKSAP 16 - NeurologyDocument333 pagesMKSAP 16 - NeurologyBacanator100% (4)
- Mcqs Faculty of General Medicine VI YearDocument110 pagesMcqs Faculty of General Medicine VI YearAbdimajiid100% (2)
- Diagnosing Secondary Headaches (Practical Neurology) (2020 - 05)Document5 pagesDiagnosing Secondary Headaches (Practical Neurology) (2020 - 05)Apostolos T.No ratings yet
- Collection IELTS EssaysDocument237 pagesCollection IELTS EssaysНастя Костенко100% (1)
- 5-Surgical Management of Ptosis and Brow PtosisDocument21 pages5-Surgical Management of Ptosis and Brow PtosisJovan Z. Popović100% (1)
- Diagnosis and Treatment of Traumatic Brain InjuryDocument22 pagesDiagnosis and Treatment of Traumatic Brain InjuryAmandaNo ratings yet
- Step-by-Step Guide to DVT Ultrasound Exam of Lower ExtremitiesDocument37 pagesStep-by-Step Guide to DVT Ultrasound Exam of Lower ExtremitiesEL SHITANo ratings yet
- Headache NewDocument17 pagesHeadache NewHaris PeaceNo ratings yet
- Definition, Classification, Etiology, and Pathophysiology of Shock in Adults - UpToDateDocument20 pagesDefinition, Classification, Etiology, and Pathophysiology of Shock in Adults - UpToDateblip blip blooopNo ratings yet
- Postoperative Fever - UpToDate PDFDocument25 pagesPostoperative Fever - UpToDate PDFkatsuiaNo ratings yet
- General Pathology MCQsDocument32 pagesGeneral Pathology MCQsedcrfvtgb12345684% (37)
- Approach To The Adult Patient With Syncope in The Emergency DepartmentDocument26 pagesApproach To The Adult Patient With Syncope in The Emergency DepartmentVinicius DumontNo ratings yet
- Anatomy Physiology Nervous System Brain Stroke Risk FactorsDocument4 pagesAnatomy Physiology Nervous System Brain Stroke Risk FactorsKimsha ConcepcionNo ratings yet
- Brain TumorDocument18 pagesBrain TumorSKSAIDINESH100% (1)
- Evaluation of The Adult With Nontraumatic Headache in The Emergency Department - UpToDateDocument35 pagesEvaluation of The Adult With Nontraumatic Headache in The Emergency Department - UpToDateJuanda MedinaNo ratings yet
- Evaluation of Headache in AdultsDocument21 pagesEvaluation of Headache in AdultsMaicon RamosNo ratings yet
- CEFALEA Evaluation of Headache in Adults - UpToDateDocument23 pagesCEFALEA Evaluation of Headache in Adults - UpToDateJOSE ANTONIO ALBARRAN MENDOZANo ratings yet
- Evaluation of Headache in AdultsDocument19 pagesEvaluation of Headache in AdultsBeatriz SilvaNo ratings yet
- Evaluation of Headache in Adults - UpToDateDocument18 pagesEvaluation of Headache in Adults - UpToDateSebastianNo ratings yet
- Overview of The Clinical Features and Diagnosis of Brain Tumors in AdultsDocument37 pagesOverview of The Clinical Features and Diagnosis of Brain Tumors in AdultsFSHB-A&ANo ratings yet
- Etiology and evaluation of weakness in childrenDocument20 pagesEtiology and evaluation of weakness in childrenPWaaaaNo ratings yet
- Syncope in AdultsDocument42 pagesSyncope in AdultsZabatehNo ratings yet
- Acute Viral Encephalitis in ChildrenDocument16 pagesAcute Viral Encephalitis in ChildrenCF PonceNo ratings yet
- Acute Headache - StatPearls - NCBI BookshelfDocument11 pagesAcute Headache - StatPearls - NCBI BookshelfMuhammad Shaheer SajidNo ratings yet
- Cardinal Manifestations HeadacheDocument51 pagesCardinal Manifestations HeadacheRoby KieranNo ratings yet
- HEADACHESDocument5 pagesHEADACHESDaniel PancuNo ratings yet
- Sin CopeDocument40 pagesSin Copehanna gabriela figueroa silvaNo ratings yet
- Approach To The Adult Patient With Syncope in The Emergency DepartmentDocument45 pagesApproach To The Adult Patient With Syncope in The Emergency Departmentcarolina pulidoNo ratings yet
- Headache: Paul G. Mathew, M.D., and Ivan Garza, M.DDocument13 pagesHeadache: Paul G. Mathew, M.D., and Ivan Garza, M.DElizabeth PedruezaNo ratings yet
- Syncope in Adults - Clinical Manifestations and Initial Diagnostic Evaluation - UpToDateDocument21 pagesSyncope in Adults - Clinical Manifestations and Initial Diagnostic Evaluation - UpToDateBruno FernandesNo ratings yet
- 1 Neuropsychiatry of HeadacheDocument6 pages1 Neuropsychiatry of HeadachepriyadikkalaNo ratings yet
- Approach in EmergenciesDocument41 pagesApproach in Emergenciesnotasmedicinaint2022No ratings yet
- Acute Viral Encephalitis in Children Clinical Manifestations and DiagnosisDocument41 pagesAcute Viral Encephalitis in Children Clinical Manifestations and DiagnosisCRISTOPHER CHAVAR GARCIANo ratings yet
- Stupor and Coma in AdultsDocument14 pagesStupor and Coma in AdultsElena Chitoiu100% (1)
- Convulsive Status Epilepticus in Adults - Classification, Clinical Features, and DiagnosisDocument8 pagesConvulsive Status Epilepticus in Adults - Classification, Clinical Features, and DiagnosisDaniel BallesterosNo ratings yet
- Stupor and Coma in Adults: Author: Section Editors: Deputy EditorDocument30 pagesStupor and Coma in Adults: Author: Section Editors: Deputy EditorYessenia BarrantesNo ratings yet
- Stupor and Coma in Adults - UpToDateDocument46 pagesStupor and Coma in Adults - UpToDatemgvbNo ratings yet
- Definition, Classification, Etiology, and Pathophysiology of Shock in Adults - UpToDateDocument18 pagesDefinition, Classification, Etiology, and Pathophysiology of Shock in Adults - UpToDatePaloma GBNo ratings yet
- Initial Assessment and Management of Acute StrokeDocument41 pagesInitial Assessment and Management of Acute StrokeandresNo ratings yet
- Definition, Classification, Etiology, and Pathophysiology of Shock in Adults - UpToDateDocument16 pagesDefinition, Classification, Etiology, and Pathophysiology of Shock in Adults - UpToDatevara prasadNo ratings yet
- Compromiso de Conciencia UptodateDocument32 pagesCompromiso de Conciencia UptodatelbobadillabNo ratings yet
- Acute Headache Management in Emergency Department 2019Document9 pagesAcute Headache Management in Emergency Department 2019SamuelsonNo ratings yet
- Headaches - Ira RahmawatiDocument20 pagesHeadaches - Ira RahmawatiPutri NaylaaNo ratings yet
- Clinical Manifestations and Diagnosis of Central Nervous System Tumors in ChildrenDocument27 pagesClinical Manifestations and Diagnosis of Central Nervous System Tumors in ChildrenFSHB-A&ANo ratings yet
- Ischemic StrokeDocument13 pagesIschemic StrokearthurbaidoodouglasNo ratings yet
- Syncope in Adults - Clinical Manifestations and Initial Diagnostic EvaluationDocument26 pagesSyncope in Adults - Clinical Manifestations and Initial Diagnostic EvaluationRaúl MartínezNo ratings yet
- Headache in ChildrenDocument30 pagesHeadache in ChildrenDeiby TorricoNo ratings yet
- Headaches Attributed To Ischemic Stroke and Transient Ischemic AttackDocument8 pagesHeadaches Attributed To Ischemic Stroke and Transient Ischemic Attackchartreuse avonleaNo ratings yet
- Approach To HeadacheDocument61 pagesApproach To Headachesabahat.husainNo ratings yet
- Pearls: Headache: David W. Dodick, M.DDocument8 pagesPearls: Headache: David W. Dodick, M.DLightNo ratings yet
- Pitfallsinthe Managementof Headacheinthe Emergency DepartmentDocument21 pagesPitfallsinthe Managementof Headacheinthe Emergency DepartmentOscar Gregorio Coronado MacdanielNo ratings yet
- Kopel, Et Al. (2021)Document18 pagesKopel, Et Al. (2021)CARLOS SANTIAGO PEREZ RODRIGUEZNo ratings yet
- Acute Headache Guide for Emergency PhysiciansDocument6 pagesAcute Headache Guide for Emergency PhysiciansRoselyn DawongNo ratings yet
- Perinatal Brain Damage Causes and TreatmentDocument5 pagesPerinatal Brain Damage Causes and TreatmentIsak ShatikaNo ratings yet
- Headache and Facial Pain: Key PointsDocument5 pagesHeadache and Facial Pain: Key PointsCaesar Muhammad WijayaNo ratings yet
- Initial Assessment and Management of Acute Stroke - UpToDateDocument27 pagesInitial Assessment and Management of Acute Stroke - UpToDateDiego VillacisNo ratings yet
- Definition, Classification, Etiology, and Pathophysiology of Shock in AdultsDocument26 pagesDefinition, Classification, Etiology, and Pathophysiology of Shock in AdultsValerie ZimmermannNo ratings yet
- 1 s2.0 S0736467917311897 MainDocument11 pages1 s2.0 S0736467917311897 MainA2150A N Fikri AbrorNo ratings yet
- Initial Assessment and Management of Acute StrokeDocument49 pagesInitial Assessment and Management of Acute StrokeIrina DuceacNo ratings yet
- General physical exam of neuro systemDocument112 pagesGeneral physical exam of neuro systemSuganya BalachandranNo ratings yet
- Shock UptodateDocument47 pagesShock UptodateMartín A. GaticaNo ratings yet
- Initial Evaluation of VertigoDocument11 pagesInitial Evaluation of VertigoIraNo ratings yet
- ABC Emergency Differential DiagnosisewwwwweDocument3 pagesABC Emergency Differential Diagnosisewwwwwesharu4291No ratings yet
- Cerebral Herniation Syndromes and Intracranial HypertensionFrom EverandCerebral Herniation Syndromes and Intracranial HypertensionMatthew KoenigNo ratings yet
- ANATOMY OF THE EYE Mindmap - Dr. PraneshDocument1 pageANATOMY OF THE EYE Mindmap - Dr. PraneshDr Pranesh BalasubramaniamNo ratings yet
- 225 DIV1 5503623 Personal+SpecificationDocument28 pages225 DIV1 5503623 Personal+SpecificationDr Pranesh BalasubramaniamNo ratings yet
- 21 - Episcleritis & Scleritis PDFDocument11 pages21 - Episcleritis & Scleritis PDFHasan AnsariNo ratings yet
- 225 DIV1 5503623 Personal+SpecificationDocument28 pages225 DIV1 5503623 Personal+SpecificationDr Pranesh BalasubramaniamNo ratings yet
- Recent Advances in Retinoblastoma Management and GeneticsDocument12 pagesRecent Advances in Retinoblastoma Management and GeneticsDr Pranesh BalasubramaniamNo ratings yet
- Recent Advances in Retinoblastoma Management and GeneticsDocument12 pagesRecent Advances in Retinoblastoma Management and GeneticsDr Pranesh BalasubramaniamNo ratings yet
- Recent Advances in Retinoblastoma Management and GeneticsDocument12 pagesRecent Advances in Retinoblastoma Management and GeneticsDr Pranesh BalasubramaniamNo ratings yet
- 01.blindness and Vision Impairment in A RuralDocument8 pages01.blindness and Vision Impairment in A RuralDr Pranesh BalasubramaniamNo ratings yet
- Cat Grading ReviewDocument6 pagesCat Grading ReviewDr Pranesh BalasubramaniamNo ratings yet
- Optic Disc: Normal Color, Pseudo Atrophy, Types of Optic AtrophyDocument35 pagesOptic Disc: Normal Color, Pseudo Atrophy, Types of Optic AtrophyDr Pranesh BalasubramaniamNo ratings yet
- Demystifying Viral Anterior Uveitis: A Review: Nicole Shu-Wen Chan Mbbs - Soon-Phaik Chee Frcophth Mmed (S'Pore)Document14 pagesDemystifying Viral Anterior Uveitis: A Review: Nicole Shu-Wen Chan Mbbs - Soon-Phaik Chee Frcophth Mmed (S'Pore)Dr Pranesh BalasubramaniamNo ratings yet
- CARE Checklist English 2013 PDFDocument1 pageCARE Checklist English 2013 PDFNithin NairNo ratings yet
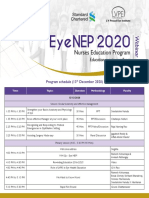
- Eyenep Program SheduledDocument1 pageEyenep Program SheduledDr Pranesh BalasubramaniamNo ratings yet
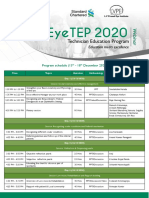
- Eyeoep Program SheduledDocument1 pageEyeoep Program SheduledDr Pranesh BalasubramaniamNo ratings yet
- 2005 Clinical Importance of LOCS III in Phacoemulsification - Bencic PDFDocument4 pages2005 Clinical Importance of LOCS III in Phacoemulsification - Bencic PDFMauVeeNo ratings yet
- LV Prasad Eye Institute EyeTEP 2020 WebinarDocument1 pageLV Prasad Eye Institute EyeTEP 2020 WebinarDr Pranesh BalasubramaniamNo ratings yet
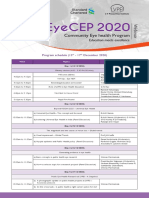
- Eyecep Program SheduledDocument1 pageEyecep Program SheduledDr Pranesh BalasubramaniamNo ratings yet
- White Dot Synd Biswas PDFDocument57 pagesWhite Dot Synd Biswas PDFDr Pranesh BalasubramaniamNo ratings yet
- Cerebral Infarction Pattern in Tuberculous Meningitis: MethodologyDocument10 pagesCerebral Infarction Pattern in Tuberculous Meningitis: MethodologyJanice MuliadiNo ratings yet
- Dengue Optic NeuropathyDocument1 pageDengue Optic NeuropathyDr Pranesh BalasubramaniamNo ratings yet
- Special Names in SurgeryDocument20 pagesSpecial Names in SurgeryDr Pranesh Balasubramaniam100% (1)
- Presentation Tips by Presentation ZenDocument6 pagesPresentation Tips by Presentation ZenmuhjaerNo ratings yet
- Nutritional Deficiency Anemias: by Satish SDocument26 pagesNutritional Deficiency Anemias: by Satish SDr Pranesh BalasubramaniamNo ratings yet
- B Lood: Bleeding and Thrombosis in The Myeloproliferative DisordersDocument13 pagesB Lood: Bleeding and Thrombosis in The Myeloproliferative DisordersJicko Street HooligansNo ratings yet
- Hemo Dynamic Disorders Thrombo Embolism and ShockDocument29 pagesHemo Dynamic Disorders Thrombo Embolism and ShockMai ÜüNo ratings yet
- Autopsy in The Event of Maternal Death - A UK Perspective: ReviewDocument8 pagesAutopsy in The Event of Maternal Death - A UK Perspective: ReviewMayada OsmanNo ratings yet
- Hyaluronic Acid Embolism Treated With Subcutaneous High and Low Hyaluronidase Doses: Efficacy and Surrounding Tissue EffectDocument8 pagesHyaluronic Acid Embolism Treated With Subcutaneous High and Low Hyaluronidase Doses: Efficacy and Surrounding Tissue Effectkalinca marizyNo ratings yet
- Nursing - January 2024Document68 pagesNursing - January 2024kenangrok2009No ratings yet
- Elevated Risk of Blood Clots in Women Taking Birth Control Containing Drospirenone, Study ShowsDocument3 pagesElevated Risk of Blood Clots in Women Taking Birth Control Containing Drospirenone, Study ShowsJomerlyn AbaricoNo ratings yet
- Hugo Dato Discharge Summary (Informe de Alta Hugo Dato)Document14 pagesHugo Dato Discharge Summary (Informe de Alta Hugo Dato)Mouline TarikNo ratings yet
- Teaching Slide Recognising ThrombophlebitisDocument27 pagesTeaching Slide Recognising Thrombophlebitisramuoodoo83% (6)
- Andexxa Formulary KitDocument32 pagesAndexxa Formulary KitAlbert ChangNo ratings yet
- LIVER TRANSIENT HEPATIC ATTENUATION DEFECT ExplainedDocument6 pagesLIVER TRANSIENT HEPATIC ATTENUATION DEFECT Explainedcalustre2016No ratings yet
- 5W FeverDocument14 pages5W FeverYork GarcíaNo ratings yet
- PBL 2 - StrokeDocument14 pagesPBL 2 - StrokeKong Pei IngNo ratings yet
- ACEP - October 2023 1Document24 pagesACEP - October 2023 1s2qtxnxwk7No ratings yet
- 111 - Contact PrecautionsDocument115 pages111 - Contact PrecautionsOlgaKNo ratings yet
- 2137 FullDocument7 pages2137 FullCourtneykdNo ratings yet
- Hemostasis in FESSDocument22 pagesHemostasis in FESSJAGANNo ratings yet
- Acute Limb Ischemia: Clinical PracticeDocument9 pagesAcute Limb Ischemia: Clinical PracticeIndah MaulidawatiNo ratings yet
- Antithrombotic Therapy For VTE DiseaseDocument169 pagesAntithrombotic Therapy For VTE DiseaseMauricio Pedraza CiroNo ratings yet
- Advice and Exercises After A Total Hip Replacement THR - Jun21Document15 pagesAdvice and Exercises After A Total Hip Replacement THR - Jun21Julenda CintarinovaNo ratings yet
- Drugs That Affect The Hematological SystemDocument4 pagesDrugs That Affect The Hematological Systemoxidalaj100% (2)