You might also like
- Post-Operative Care, DSTC Online, Jun.2021Document38 pagesPost-Operative Care, DSTC Online, Jun.2021tepat rshsNo ratings yet
- 2.6.B Yohana USG Guided Core BiopsyDocument42 pages2.6.B Yohana USG Guided Core Biopsytepat rshsNo ratings yet
- Falsafah Penanggulangan Trauma 2012Document22 pagesFalsafah Penanggulangan Trauma 2012ryanNo ratings yet
- Skoring Dalam Trauma: Suryadi SoedarmoDocument23 pagesSkoring Dalam Trauma: Suryadi Soedarmotepat rshsNo ratings yet
- Kibi - DSTC - How To Keep The PT Alive I Juni 21Document32 pagesKibi - DSTC - How To Keep The PT Alive I Juni 21tepat rshsNo ratings yet
- 2.4.B DR Denni Clinical Evidence of Ribociclib Into Clinical PracticeDocument40 pages2.4.B DR Denni Clinical Evidence of Ribociclib Into Clinical Practicetepat rshsNo ratings yet
- 2.5 Dr. I Gede CRP DR BSTDocument42 pages2.5 Dr. I Gede CRP DR BSTtepat rshsNo ratings yet
- 2.2.a Dr. Dimyati Innovative Approach in Differentiated Thyroid Cancer ManagementDocument36 pages2.2.a Dr. Dimyati Innovative Approach in Differentiated Thyroid Cancer Managementtepat rshsNo ratings yet
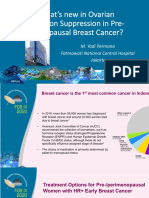
- 2.3.a DR Yadi Permana Whats New in Ovarian Function Suppression in Pre-MenopausalDocument36 pages2.3.a DR Yadi Permana Whats New in Ovarian Function Suppression in Pre-Menopausaltepat rshsNo ratings yet
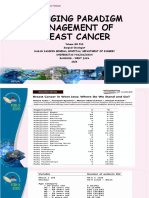
- 2.6.a Dr. Yohana Changing Paradigm Management of Breast CancerDocument11 pages2.6.a Dr. Yohana Changing Paradigm Management of Breast Cancertepat rshsNo ratings yet
- 2.7.a DR - Hasrayati FOB IX - FNAB ThyroidDocument35 pages2.7.a DR - Hasrayati FOB IX - FNAB Thyroidtepat rshsNo ratings yet
- 2.2.B Dr. Erwin Best Practice Sharing For Radio Iodine RefracterDocument76 pages2.2.B Dr. Erwin Best Practice Sharing For Radio Iodine Refractertepat rshsNo ratings yet
- 2.4.a Dr. Samuel J Haryono Rationale of Using CDK 4:6 Inhibitors in HR Positive ABCDocument24 pages2.4.a Dr. Samuel J Haryono Rationale of Using CDK 4:6 Inhibitors in HR Positive ABCtepat rshsNo ratings yet
- 2.1.B Dr. Riadhi Practical Issue in The FieldDocument16 pages2.1.B Dr. Riadhi Practical Issue in The Fieldtepat rshsNo ratings yet
- 2.1.B Dr. Riadhi Practical Issue in The FieldDocument16 pages2.1.B Dr. Riadhi Practical Issue in The Fieldtepat rshsNo ratings yet
- Advance Cardiac Life SupportDocument18 pagesAdvance Cardiac Life Supporttepat rshsNo ratings yet
- 1.2.a Dr. Sonar Bendamustine and LymphomaDocument45 pages1.2.a Dr. Sonar Bendamustine and Lymphomatepat rshsNo ratings yet
- 5.2 Thoracotomy EmergencyDocument28 pages5.2 Thoracotomy Emergencytepat rshsNo ratings yet
- 1.2.b. Dr. Dwi Hari Susilo - Management of Advanced Head & Neck CancerDocument32 pages1.2.b. Dr. Dwi Hari Susilo - Management of Advanced Head & Neck Cancertepat rshsNo ratings yet
- 1.4.a Prof Ramdan FOB IX - Genetics Counseling-Where Are WeDocument26 pages1.4.a Prof Ramdan FOB IX - Genetics Counseling-Where Are Wetepat rshsNo ratings yet
- 1.4.B DR Monty Genomic Profiling To Guide Treatment Decision in Early Stage Breast CancerDocument43 pages1.4.B DR Monty Genomic Profiling To Guide Treatment Decision in Early Stage Breast Cancertepat rshsNo ratings yet
- 5.3 Subcutaneous EmphysemaDocument15 pages5.3 Subcutaneous Emphysematepat rshsNo ratings yet
- 2.3 Coronary Artery Bypass GraftingDocument30 pages2.3 Coronary Artery Bypass Graftingtepat rshsNo ratings yet
- 4.1 TO TorakotomiDocument29 pages4.1 TO Torakotomitepat rshsNo ratings yet
- 2.1 Luka Tusuk Dan Tembak Pada ThoraxDocument17 pages2.1 Luka Tusuk Dan Tembak Pada Thoraxtepat rshsNo ratings yet
- 2.8 Chest PhysiotherapyDocument17 pages2.8 Chest Physiotherapytepat rshsNo ratings yet
- Pelvic FracturesDocument37 pagesPelvic Fracturestepat rshsNo ratings yet
- 1.3 Options For Thoracic Surgical ApproachesDocument13 pages1.3 Options For Thoracic Surgical Approachestepat rshsNo ratings yet
- Prehospital Management of BurnsDocument21 pagesPrehospital Management of Burnstepat rshsNo ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (120)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Basic Life SupportDocument28 pagesBasic Life SupportMaesaNo ratings yet
- Macromolecule LabDocument7 pagesMacromolecule Labapi-318665838No ratings yet
- Jurnal DentistDocument8 pagesJurnal DentistAnugrah AztriNo ratings yet
- Journal 032019 PDFDocument64 pagesJournal 032019 PDFestefyNo ratings yet
- Health Examination ReportDocument6 pagesHealth Examination ReportVince LimNo ratings yet
- 2018 Book IntracerebralHemorrhageTherape PDFDocument210 pages2018 Book IntracerebralHemorrhageTherape PDFLinaSuarezNo ratings yet
- Acceptance and Commitment Therapy For Chronic PainDocument190 pagesAcceptance and Commitment Therapy For Chronic PainKenji Yonezawa100% (6)
- 2017 MP Starter Plan 5 To 9 Proposal - Complete RidersDocument17 pages2017 MP Starter Plan 5 To 9 Proposal - Complete RidersJoselle M. GaddiNo ratings yet
- Ingredients:: The Lemonade Diet (Adapted From)Document2 pagesIngredients:: The Lemonade Diet (Adapted From)test100% (2)
- Wisdom TeethDocument2 pagesWisdom TeethMr bondNo ratings yet
- STAGES of AnesthesiaDocument4 pagesSTAGES of AnesthesiaMabz Posadas BisnarNo ratings yet
- Genital Dermatology Atlas: Second EditionDocument343 pagesGenital Dermatology Atlas: Second EditionAnonymous MPGsKXw7No ratings yet
- Michelle Robinson ResumeDocument4 pagesMichelle Robinson Resumeapi-329474244No ratings yet
- CC1 Lab. Notes (Carbo)Document5 pagesCC1 Lab. Notes (Carbo)Kimberly Joy GregorioNo ratings yet
- Final BBCR PrefaceDocument8 pagesFinal BBCR PrefaceSushma NaigotriyaNo ratings yet
- Neuromuscular Disorders: Peripheral Nervous System/ Myelopathy Case SessionDocument3 pagesNeuromuscular Disorders: Peripheral Nervous System/ Myelopathy Case Sessionamitm2012No ratings yet
- NCLEX PracticeDocument18 pagesNCLEX Practiceandrew504777No ratings yet
- SPINE Course Materials Spine Pathway PDFDocument82 pagesSPINE Course Materials Spine Pathway PDFYoka Mahendra PranaNo ratings yet
- Engagement in Child and Adolescent Treatment - The Role of Parental Cognitions and AttributionsDocument16 pagesEngagement in Child and Adolescent Treatment - The Role of Parental Cognitions and Attributionssolutions4familyNo ratings yet
- Case PresentationDocument7 pagesCase PresentationGrace SamNo ratings yet
- Jurnal Effect of CBT InterventionDocument18 pagesJurnal Effect of CBT InterventionMUHAMMAD FAIZ BIN ABD RAHMANNo ratings yet
- Dry Needling Versus Acupuncture: The Ongoing Debate: Acupuncture in Medicine November 2015Document8 pagesDry Needling Versus Acupuncture: The Ongoing Debate: Acupuncture in Medicine November 2015ريما ميماNo ratings yet
- AutPlay PowerpointDocument48 pagesAutPlay PowerpointSarah CummingsNo ratings yet
- Pharmacy Informatics NotesDocument3 pagesPharmacy Informatics NotesSmoi Liver100% (2)
- Reverse AbdominoplastyDocument3 pagesReverse AbdominoplastyongchenguanNo ratings yet
- TracheomalaciaDocument11 pagesTracheomalaciaAgung BhaktiyarNo ratings yet
- Haute Couture HolidaysDocument452 pagesHaute Couture HolidaysJethro Gabriel TrinidadNo ratings yet
- Sankhya SampraptiDocument20 pagesSankhya Sampraptidr-sachNo ratings yet
- Legal Med. Report-QueenDocument61 pagesLegal Med. Report-QueenQuinnee VallejosNo ratings yet
- Pallavaram CETPDocument14 pagesPallavaram CETPsnahushNo ratings yet