You might also like
- Training On Good Manufacturing PracticesDocument26 pagesTraining On Good Manufacturing PracticesxxkooonxxNo ratings yet
- Research PaperDocument14 pagesResearch PaperWatashi Wa Darl Desu100% (1)
- MateriaMedica DunhamDocument436 pagesMateriaMedica Dunhamphani_bNo ratings yet
- A Training Module For Retail SroreDocument24 pagesA Training Module For Retail SroreMudassar Nawaz90% (31)
- A Study of Knowledge, Attitude & Practice On Food Safety Among The Food Handlers in The Restaurants of Kalyani, District: NadiaDocument13 pagesA Study of Knowledge, Attitude & Practice On Food Safety Among The Food Handlers in The Restaurants of Kalyani, District: NadiaIJAR JOURNALNo ratings yet
- Grade 8 Nail Care Midterm ExamDocument2 pagesGrade 8 Nail Care Midterm ExamSir Game Credits100% (1)
- Food Sanitation Practices of Kubo Food Court EstablishmentsDocument21 pagesFood Sanitation Practices of Kubo Food Court EstablishmentsEvogen GenesisNo ratings yet
- Food Handler's Manual: InstructorFrom EverandFood Handler's Manual: InstructorRating: 5 out of 5 stars5/5 (1)
- Food Safety Knowledge and Self-Reported Practices PDFDocument29 pagesFood Safety Knowledge and Self-Reported Practices PDFAlle Eiram PadilloNo ratings yet
- NABH QuestionnaireDocument3 pagesNABH QuestionnairePoojitha KNo ratings yet
- The Problem and Its Setting Background of The StudyDocument70 pagesThe Problem and Its Setting Background of The StudyJoana Mae M. WamarNo ratings yet
- Food Safety Knowledge, Attitude and Hygiene Practices Among The Street Food Vendors in Northern Kuching City, SarawakDocument9 pagesFood Safety Knowledge, Attitude and Hygiene Practices Among The Street Food Vendors in Northern Kuching City, SarawakFidya Ardiny50% (2)
- Relationship of Knowledge and Attitude With Food Handling Practices: A Systematic ReviewDocument12 pagesRelationship of Knowledge and Attitude With Food Handling Practices: A Systematic ReviewIJPHSNo ratings yet
- Food Handling Serving and Hygiene PractiDocument7 pagesFood Handling Serving and Hygiene PractiFarha KamilatunNo ratings yet
- Go Septic TankDocument6 pagesGo Septic TankAnniesonNo ratings yet
- Food Hygiene and Safety Practices of Food EstablishmentsDocument4 pagesFood Hygiene and Safety Practices of Food EstablishmentsIJAR JOURNAL100% (1)
- The Evaluation of Food Hygiene Knowledge, Attitudes, and PracticesDocument6 pagesThe Evaluation of Food Hygiene Knowledge, Attitudes, and PracticessyooloveNo ratings yet
- Determinants of Food Safety Practices Among Food Handlers in Selected Food EstablishmentsDocument9 pagesDeterminants of Food Safety Practices Among Food Handlers in Selected Food EstablishmentsIJPHSNo ratings yet
- Ijphs Fix B.inggrisDocument14 pagesIjphs Fix B.inggrisrizkimNo ratings yet
- Research PaperDocument19 pagesResearch PaperDearlyne AlmazanNo ratings yet
- Thesis About Improper Hygiene11Document18 pagesThesis About Improper Hygiene11Angelie UmambacNo ratings yet
- Articulo - Food Safety and Education LevelDocument6 pagesArticulo - Food Safety and Education LevelNicole PerezNo ratings yet
- Evaluating Food Safety Knowledge and Practices Among Foodservice Staff in Al Madinah Hospitals, Saudi ArabiaDocument19 pagesEvaluating Food Safety Knowledge and Practices Among Foodservice Staff in Al Madinah Hospitals, Saudi ArabiaAiza ConchadaNo ratings yet
- Cross Sectional Study On Safety FoodDocument6 pagesCross Sectional Study On Safety FoodSiska PratiwiNo ratings yet
- Baluka Et Al - Janaury 2015Document12 pagesBaluka Et Al - Janaury 2015Iwan Suryadi MahmudNo ratings yet
- Evaluation of Basic Knowledge On Food Safety and Food Handling Practices Amongst Migrant in MalaysiaDocument10 pagesEvaluation of Basic Knowledge On Food Safety and Food Handling Practices Amongst Migrant in MalaysiaSiska PratiwiNo ratings yet
- Food Sanitation and Hygiene Practices Among Food Handlers in Food Joints in HyderabadDocument6 pagesFood Sanitation and Hygiene Practices Among Food Handlers in Food Joints in HyderabadEditor IJTSRDNo ratings yet
- Jurnal International Gizi Institusi - Higiene Dan Sanitasi Penyelenggaraan Makanan InstitusiDocument8 pagesJurnal International Gizi Institusi - Higiene Dan Sanitasi Penyelenggaraan Makanan InstitusiAsri Dewi Putri100% (1)
- Philtech Thesis - Ara, Allyson, Vanessa, Jia, JerwinDocument12 pagesPhiltech Thesis - Ara, Allyson, Vanessa, Jia, JerwinAragrace MalejanaNo ratings yet
- Food Sanitation Practices in A Private Education InstitutionDocument33 pagesFood Sanitation Practices in A Private Education InstitutionGwen De CastroNo ratings yet
- 1 - Food Safety Assessment On Knowledge, Attitude, and Practice A Study Among Food HandlersDocument6 pages1 - Food Safety Assessment On Knowledge, Attitude, and Practice A Study Among Food Handlerslassan199358No ratings yet
- Food Hygienic Practices and Safety Measures AmongDocument7 pagesFood Hygienic Practices and Safety Measures AmongIntrovert PrinzNo ratings yet
- Adellade Luchinga ProjectDocument14 pagesAdellade Luchinga ProjectDERRICK OCHIENGNo ratings yet
- Assessment of The Food Hygiene Practices of Food Handlers in The Federal Capital Territory of NigeriaDocument6 pagesAssessment of The Food Hygiene Practices of Food Handlers in The Federal Capital Territory of Nigeriarafael514No ratings yet
- Assessment of Knowledge, Attitude and Practices Concerning Food Safety Among Restaurant Workers in Putrajaya, MalaysiaDocument10 pagesAssessment of Knowledge, Attitude and Practices Concerning Food Safety Among Restaurant Workers in Putrajaya, MalaysiaAlexander DeckerNo ratings yet
- Nutrition Vol 6 No2 P 346-353Document8 pagesNutrition Vol 6 No2 P 346-353sara6anneNo ratings yet
- Application of The WHO Keys of Safer Food To Improve Food Handling Practices of Food Vendors in A Poor Resource Community in GhanaDocument10 pagesApplication of The WHO Keys of Safer Food To Improve Food Handling Practices of Food Vendors in A Poor Resource Community in GhanaOldriana Prawiro HapsariNo ratings yet
- RESEARCH - Chapter 1Document9 pagesRESEARCH - Chapter 1Ivan PadecioNo ratings yet
- DocumentDocument11 pagesDocumentepokayeNo ratings yet
- Chapter 22Document11 pagesChapter 22MaryGraceVelascoFuentesNo ratings yet
- Siow NorraDocument9 pagesSiow NorraJan Oneille Y. VallesNo ratings yet
- Journal Homepage: - : 61 YearsDocument11 pagesJournal Homepage: - : 61 YearsIJAR JOURNALNo ratings yet
- Final Research 2Document23 pagesFinal Research 2Richael ImpasNo ratings yet
- Chapter 1Document8 pagesChapter 1Mikageシ TVNo ratings yet
- Background of The StudyDocument3 pagesBackground of The StudyKraeNo ratings yet
- JSKM2013 PerkasakafetariaDocument9 pagesJSKM2013 PerkasakafetariaMuhammad BaihaqiNo ratings yet
- RESEARCH TITLE-WPS OfficeDocument9 pagesRESEARCH TITLE-WPS OfficeDaisy Joy SalavariaNo ratings yet
- Beyond HandwashingDocument8 pagesBeyond HandwashingvgmejiaNo ratings yet
- Food Safety Practices Among Vendors in Capaoay San Jacinto PangasinanDocument4 pagesFood Safety Practices Among Vendors in Capaoay San Jacinto PangasinanPatricia Mae SabadoNo ratings yet
- 8-Article Text-13-1-10-20200803Document10 pages8-Article Text-13-1-10-20200803Adonis BesaNo ratings yet
- Main Main - Final - Result - Project - 2Document65 pagesMain Main - Final - Result - Project - 2Ebuka AniNo ratings yet
- Research ArticleDocument10 pagesResearch ArticlealpahchichupsNo ratings yet
- The Effect of Food Safety Education On Handwashing Practices in School Canteens' Food HandlersDocument10 pagesThe Effect of Food Safety Education On Handwashing Practices in School Canteens' Food HandlersJhervhee A. ArapanNo ratings yet
- 1739 6742 1 PBDocument10 pages1739 6742 1 PBrsud.latemmamalaspgNo ratings yet
- Effect of Hygiene Guidelines On Knowledge, Attitudes, and Practices of Food Handlers at University CafeteriasDocument12 pagesEffect of Hygiene Guidelines On Knowledge, Attitudes, and Practices of Food Handlers at University CafeteriasOSCAR DE JESUS FLORESNo ratings yet
- Research Paper (Judy Garcia & Ybeth Duerme)Document8 pagesResearch Paper (Judy Garcia & Ybeth Duerme)Judy GarciaNo ratings yet
- JEHAST Kesehatan LingkunganDocument4 pagesJEHAST Kesehatan LingkunganDela ElisaNo ratings yet
- Studi Tentang Pengetahuan, Perilaku Dan Kebersihan Penjamah Makanan Di Instalasi Gizi Blu Rsup Prof. Dr. R.D Kandou ManadoDocument8 pagesStudi Tentang Pengetahuan, Perilaku Dan Kebersihan Penjamah Makanan Di Instalasi Gizi Blu Rsup Prof. Dr. R.D Kandou Manadorani afridaNo ratings yet
- Literature Review On Food Safety KnowledgeDocument5 pagesLiterature Review On Food Safety Knowledgeafmzwrhwrwohfn100% (1)
- Food Control: Norrakiah Abdullah Sani, Oi Nee SiowDocument8 pagesFood Control: Norrakiah Abdullah Sani, Oi Nee SiowJerod KingNo ratings yet
- HACCP Rumah SakitDocument7 pagesHACCP Rumah SakitnanaazzahraNo ratings yet
- Essay Article On Consumer Awareness Towards Food SafetyDocument4 pagesEssay Article On Consumer Awareness Towards Food SafetyMohd Faizal Bin AyobNo ratings yet
- The Final Result Project 2Document32 pagesThe Final Result Project 2Ebuka AniNo ratings yet
- Factors Influence Awareness Canteen Student MalaysiaDocument4 pagesFactors Influence Awareness Canteen Student MalaysiaPawitra RamuNo ratings yet
- Grp5 RRLSDocument5 pagesGrp5 RRLSria.redddNo ratings yet
- Research StudyDocument2 pagesResearch StudyHadaza LanaNo ratings yet
- We Go Through Hardship in Order For Us To Become Stronger Believers and You Will Not Have Any Type of Growth OR Progresio N, If You Don'T Go Through Any Type of PainDocument1 pageWe Go Through Hardship in Order For Us To Become Stronger Believers and You Will Not Have Any Type of Growth OR Progresio N, If You Don'T Go Through Any Type of PainNadanNadhifahNo ratings yet
- Raihan BHS InggrisDocument13 pagesRaihan BHS InggrisNadanNadhifahNo ratings yet
- Emergency Basic PrincipalDocument75 pagesEmergency Basic PrincipalNarti RajakNo ratings yet
- Neuromuscular Transmission in Migraine A Single-Fiber EMG Study in Clinical SubgroupsDocument8 pagesNeuromuscular Transmission in Migraine A Single-Fiber EMG Study in Clinical SubgroupsNadanNadhifahNo ratings yet
- Iud (Intra Uterine Device)Document10 pagesIud (Intra Uterine Device)NadanNadhifahNo ratings yet
- Narrative Text:: Fairy TalesDocument15 pagesNarrative Text:: Fairy TalesNadanNadhifahNo ratings yet
- Hortatory Eksposition:: Indonesian People Should Value All The Different Culture To Promote Unity of The NationDocument5 pagesHortatory Eksposition:: Indonesian People Should Value All The Different Culture To Promote Unity of The NationNadanNadhifahNo ratings yet
- Analytical EkspositionDocument6 pagesAnalytical EkspositionNadanNadhifahNo ratings yet
- Ecology of Microorganism 1Document16 pagesEcology of Microorganism 1NadanNadhifahNo ratings yet
- Knowledge, Attitude, and Practice Among Foodworkers in Restaurants of Shahrekord, IranDocument6 pagesKnowledge, Attitude, and Practice Among Foodworkers in Restaurants of Shahrekord, IranNadanNadhifahNo ratings yet
- Jamaotolaryngology Lee 2019 Oi 190047Document7 pagesJamaotolaryngology Lee 2019 Oi 190047NadanNadhifahNo ratings yet
- CT Angiography For Acute Gastrointestinal Bleeding: What The Radiologist Needs To KnowDocument9 pagesCT Angiography For Acute Gastrointestinal Bleeding: What The Radiologist Needs To Knowintan cNo ratings yet
- Pendahuluan HelmintologiDocument38 pagesPendahuluan Helmintologiamirah sinumNo ratings yet
- DefDocument8 pagesDefNadanNadhifahNo ratings yet
- ETHIOPIADocument13 pagesETHIOPIANadanNadhifahNo ratings yet
- Jurnal 6Document7 pagesJurnal 6NadanNadhifahNo ratings yet
- Imaging and Clinical Features of Patients With 2019 Novel Coronavirus Sars-Cov-2Document6 pagesImaging and Clinical Features of Patients With 2019 Novel Coronavirus Sars-Cov-2NadanNadhifahNo ratings yet
- Transanal Endoscopic Treatmen VocalDocument6 pagesTransanal Endoscopic Treatmen VocalNadanNadhifahNo ratings yet
- A2 (Jurnal BPH)Document5 pagesA2 (Jurnal BPH)NadanNadhifahNo ratings yet
- The Clinical and Chest CT Features Associated With Severe and Critical COVID-19 PneumoniaDocument5 pagesThe Clinical and Chest CT Features Associated With Severe and Critical COVID-19 PneumoniaNadanNadhifahNo ratings yet
- Jurnal 5 PDFDocument9 pagesJurnal 5 PDFNadanNadhifahNo ratings yet
- Paed COVID 19 Case P PUL 2020Document6 pagesPaed COVID 19 Case P PUL 2020Minaz PatelNo ratings yet
- The Efficifacy Voice Theraphy in Vocal Nodul PDFDocument6 pagesThe Efficifacy Voice Theraphy in Vocal Nodul PDFNadanNadhifahNo ratings yet
- A1 (Long-Term Outcome After Thrombolysis For Acute Lower Limb Ischaemia) PDFDocument9 pagesA1 (Long-Term Outcome After Thrombolysis For Acute Lower Limb Ischaemia) PDFNadanNadhifahNo ratings yet
- Ultrasound in Evaluation Pleural Efussion PDFDocument15 pagesUltrasound in Evaluation Pleural Efussion PDFNadanNadhifahNo ratings yet
- A2 (Comparison of Prostatic Artery Embolisation (PAE) Versus Transurethral Resection of The Prostate (TURP) For Benign Prostatic Hyperplasia Randomised, Open Label, Non-Inferiority Trial)Document10 pagesA2 (Comparison of Prostatic Artery Embolisation (PAE) Versus Transurethral Resection of The Prostate (TURP) For Benign Prostatic Hyperplasia Randomised, Open Label, Non-Inferiority Trial)NadanNadhifahNo ratings yet
- Open Surgical or Endovascular Revascularization For Acute Limb IschemiaDocument9 pagesOpen Surgical or Endovascular Revascularization For Acute Limb IschemiamarisahanaNo ratings yet
- A4 (Functional Outcome Hirschprung Disease After Soave and Duhamel)Document6 pagesA4 (Functional Outcome Hirschprung Disease After Soave and Duhamel)NadanNadhifahNo ratings yet
- A3 (Lower Gastrointestinal Bleeding)Document5 pagesA3 (Lower Gastrointestinal Bleeding)NadanNadhifahNo ratings yet
- Med-Surg Skills Checklist: Loma Linda University School of NursingDocument9 pagesMed-Surg Skills Checklist: Loma Linda University School of NursingSereen KhattabNo ratings yet
- Colgate-Palmolive CompanyDocument7 pagesColgate-Palmolive CompanyDanielle Clarice ReyesNo ratings yet
- Sound Treatement Case Study - Operating TheatreDocument1 pageSound Treatement Case Study - Operating TheatreSaint-Gobain Ecophon (UK)No ratings yet
- LAS Cookery 10week 7 8Document14 pagesLAS Cookery 10week 7 8jon pantzNo ratings yet
- TR - Motorcycle Small Engine Servicing NC IIDocument162 pagesTR - Motorcycle Small Engine Servicing NC IIClint50% (2)
- Sphere Standards: Water Supply, Sanitation and Hygiene Promotion (WASH)Document29 pagesSphere Standards: Water Supply, Sanitation and Hygiene Promotion (WASH)Sote BrilloNo ratings yet
- Cholera Outbreak Guidelines: Preparedness, Prevention and ControlDocument105 pagesCholera Outbreak Guidelines: Preparedness, Prevention and ControlOxfam100% (1)
- Sluice RoomsDocument8 pagesSluice RoomsMichael Joseph Wdowiak BeijerNo ratings yet
- References Design 201304Document9 pagesReferences Design 201304BagasAdhiwangsaNo ratings yet
- Skincare With Bodycare and HaircareDocument16 pagesSkincare With Bodycare and HaircareMelvin SaweduNo ratings yet
- How To Maintain Home HygieneDocument17 pagesHow To Maintain Home HygieneShaista AkbarNo ratings yet
- PRETESTDocument2 pagesPRETESTDan Ver GawaranNo ratings yet
- Septic Tank MaintDocument1 pageSeptic Tank MaintFitri ArdhianNo ratings yet
- Proper Etiquette in A Fitness FacilityDocument3 pagesProper Etiquette in A Fitness FacilityMartin RodriguezNo ratings yet
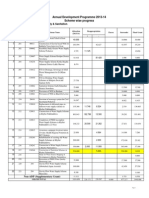
- Sector: Drinking Water Supply & Sanitation: Annual Development Programme 2013-14 Scheme Wise ProgressDocument1 pageSector: Drinking Water Supply & Sanitation: Annual Development Programme 2013-14 Scheme Wise ProgressFazal Ahmad MarwatNo ratings yet
- 21-Risk Factors Facilitating Transmission of Infectious AgentsDocument15 pages21-Risk Factors Facilitating Transmission of Infectious AgentsAnonymous 1i9aZ4V4No ratings yet
- Staal Centrum Guideline Nr03 Conveyors Focus On Hygiene 00151Document60 pagesStaal Centrum Guideline Nr03 Conveyors Focus On Hygiene 00151XavierNo ratings yet
- Sulabh International Social Service OrganisationDocument17 pagesSulabh International Social Service OrganisationNitesh KotianNo ratings yet
- WinS Monitoring System - Palapas NHS v2017-06-04Document15 pagesWinS Monitoring System - Palapas NHS v2017-06-04Josam Montero FordNo ratings yet
- AVA Food Factory Grading SystemDocument10 pagesAVA Food Factory Grading Systemstewart_hockNo ratings yet
- Course Title Front Office Service Nominal Duration of The Program Qualification LevelDocument29 pagesCourse Title Front Office Service Nominal Duration of The Program Qualification LevelAmy Amper Pelenio-LofrancoNo ratings yet
- Reviewer in Kitchen Essential and Basic Food PreparationDocument12 pagesReviewer in Kitchen Essential and Basic Food Preparationshakira avendanNo ratings yet
- Tt04-Sanitation - TIbarDocument22 pagesTt04-Sanitation - TIbarEmilia BeloNo ratings yet
- MSDS Acc1Document10 pagesMSDS Acc1Cesar Augusto Leonardo VargasNo ratings yet