You might also like
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Alipo-On - Tay Sachs DiseaseDocument3 pagesAlipo-On - Tay Sachs DiseaseJacqueline Rose Alipo-onNo ratings yet
- Hepa BDocument19 pagesHepa BJacqueline Rose Alipo-onNo ratings yet
- Isolation of Enteric BacteriaDocument4 pagesIsolation of Enteric BacteriaJacqueline Rose Alipo-onNo ratings yet
- Graduation Meeting 051922Document2 pagesGraduation Meeting 051922Jacqueline Rose Alipo-onNo ratings yet
- 64-Article Text-723-1-10-20220518Document23 pages64-Article Text-723-1-10-20220518Jacqueline Rose Alipo-onNo ratings yet
- Rizal EssayDocument1 pageRizal EssayJacqueline Rose Alipo-onNo ratings yet
- First Voyage Around The WorldDocument39 pagesFirst Voyage Around The WorldRay Patriarca65% (65)
- Viruses: Repurposing Therapeutics For Potential Treatment of Sars-Cov-2: A ReviewDocument19 pagesViruses: Repurposing Therapeutics For Potential Treatment of Sars-Cov-2: A ReviewJacqueline Rose Alipo-onNo ratings yet
- Cell Wall Synthesis InhibitorsDocument4 pagesCell Wall Synthesis InhibitorsJacqueline Rose Alipo-onNo ratings yet
- Medusa MonologueDocument1 pageMedusa MonologueJacqueline Rose Alipo-on100% (1)
- Economic Growth and the Rise of Filipino Nationalism in the 19th CenturyDocument10 pagesEconomic Growth and the Rise of Filipino Nationalism in the 19th Centurygborrinaga80% (69)
- Rizal Group ReportingDocument20 pagesRizal Group ReportingJacqueline Rose Alipo-onNo ratings yet
- Kartilya NG Katipunan Content and Contextual AnalysisDocument16 pagesKartilya NG Katipunan Content and Contextual Analysismichelle6ompad6grego69% (83)
- Literary PeriodsDocument6 pagesLiterary PeriodsHaleema Khalid100% (1)
- Seroepidemiological Investigation of Non-Health Care Worker Contacts of Middle East Respiratory Syndrome Coronavirus (Mers-Cov) Infected PatientsDocument32 pagesSeroepidemiological Investigation of Non-Health Care Worker Contacts of Middle East Respiratory Syndrome Coronavirus (Mers-Cov) Infected PatientsJacqueline Rose Alipo-onNo ratings yet
- Kartilya NG Katipunan Content and Contextual AnalysisDocument16 pagesKartilya NG Katipunan Content and Contextual Analysismichelle6ompad6grego69% (83)
- M Sars-C V-2: Olecular Docking Studies of Aromatherapy Oils Against ODocument25 pagesM Sars-C V-2: Olecular Docking Studies of Aromatherapy Oils Against OJacqueline Rose Alipo-onNo ratings yet
- "Melancholy - Art Block" PDFDocument1 page"Melancholy - Art Block" PDFJacqueline Rose Alipo-onNo ratings yet
- Philippine Declaration of Independence 1898Document3 pagesPhilippine Declaration of Independence 1898MjNo ratings yet
- Act of DeclarationDocument21 pagesAct of DeclarationRona Escaro100% (3)
- Philippine Declaration of Independence 1898Document3 pagesPhilippine Declaration of Independence 1898MjNo ratings yet
- Chinese MestizosDocument23 pagesChinese MestizosSharon Servidad-MonsaleNo ratings yet
- RA 1425 mandates study of Rizal's life and worksDocument4 pagesRA 1425 mandates study of Rizal's life and worksAlbert BertilloNo ratings yet
- Nitazoxanide/Camostat Combination For COVID19: An Unexplored Potential TherapyDocument6 pagesNitazoxanide/Camostat Combination For COVID19: An Unexplored Potential TherapyJacqueline Rose Alipo-onNo ratings yet
- Model Organisms: Jennifer Slade B.SC (Hon), M.SC CandidateDocument37 pagesModel Organisms: Jennifer Slade B.SC (Hon), M.SC CandidateJacqueline Rose Alipo-onNo ratings yet
- Cell Biology: An Introduction: Grading SystemDocument8 pagesCell Biology: An Introduction: Grading SystemJacqueline Rose Alipo-onNo ratings yet
- Module 0 RHistDocument4 pagesModule 0 RHistJacqueline Rose Alipo-onNo ratings yet
- Investigating CellsDocument11 pagesInvestigating CellsJacqueline Rose Alipo-onNo ratings yet
- Model Organisms: Jennifer Slade B.SC (Hon), M.SC CandidateDocument37 pagesModel Organisms: Jennifer Slade B.SC (Hon), M.SC CandidateJacqueline Rose Alipo-onNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Information MSQ KROK 2 Medicine 2007 2021 OTOPHYNOPHARYNGOLOGYDocument6 pagesInformation MSQ KROK 2 Medicine 2007 2021 OTOPHYNOPHARYNGOLOGYReshma Shaji PnsNo ratings yet
- Congenital and Perinatal Infections: Throwing New Light With An Old TORCHDocument27 pagesCongenital and Perinatal Infections: Throwing New Light With An Old TORCHdr_ashutosh756078No ratings yet
- What Causes Glomerular DiseaseDocument5 pagesWhat Causes Glomerular DiseaseAswin AgusNo ratings yet
- Students ProfileDocument1 pageStudents ProfileHuegene Andreu GabiNo ratings yet
- DNA Flow Technology - 2016Document2 pagesDNA Flow Technology - 2016Uswatun hasanah harifuddinNo ratings yet
- DENGUE in Tamil LanguageDocument2 pagesDENGUE in Tamil LanguageMuhammed Hunais100% (9)
- Ghannoum, Mahmoud A. - Perfect, John R - Antifungal therapy-CRC Press (2019)Document537 pagesGhannoum, Mahmoud A. - Perfect, John R - Antifungal therapy-CRC Press (2019)Defne Güller100% (1)
- Oral Tolerance:: The Response of The Intestinal Mucosa To Dietary AntigensDocument218 pagesOral Tolerance:: The Response of The Intestinal Mucosa To Dietary AntigensammarkochiNo ratings yet
- 00 Immunology and Immunochemistry Course OutlineDocument8 pages00 Immunology and Immunochemistry Course OutlineAkinbami OlorunnifemiNo ratings yet
- Reviewer - Immunoserology - Part 1Document12 pagesReviewer - Immunoserology - Part 1Joshua Trinidad0% (1)
- New COVID-19 entry protocols for FilipinosDocument5 pagesNew COVID-19 entry protocols for FilipinosmonchanNo ratings yet
- ParasitologyDocument16 pagesParasitologyRutchelNo ratings yet
- SEROLOGY 100-POINT EXAM REVIEWDocument5 pagesSEROLOGY 100-POINT EXAM REVIEWKate Camat Faminialagao100% (1)
- Epidemiology TriangleDocument1 pageEpidemiology TriangleMelDred Cajes BolandoNo ratings yet
- A Gut Feeling For Immune Dysregulation & Neuroinflammation in Autism by Aristo Vojdani, PHD, MSC, MT and Jama LambertDocument9 pagesA Gut Feeling For Immune Dysregulation & Neuroinflammation in Autism by Aristo Vojdani, PHD, MSC, MT and Jama LambertautismoneNo ratings yet
- APhA Immunization Module 3Document49 pagesAPhA Immunization Module 3Gerald GamboaNo ratings yet
- Peculiarities of Meningitis in ChildrenDocument6 pagesPeculiarities of Meningitis in ChildrenAmalia GeorgiouNo ratings yet
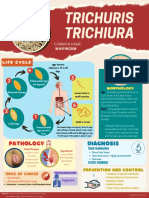
- Trichuris whipworm life cycle and pathologyDocument1 pageTrichuris whipworm life cycle and pathologyAnya IgnacioNo ratings yet
- Eur J Immunol - 2020 - Hanitsch - Treatment and Management of Primary Antibody Deficiency German InterdisciplinaryDocument15 pagesEur J Immunol - 2020 - Hanitsch - Treatment and Management of Primary Antibody Deficiency German InterdisciplinaryRSU Trijaya medical centerNo ratings yet
- Immunology and SerologyDocument66 pagesImmunology and SerologyDenver CarbonNo ratings yet
- Weight and HeiaghtDocument1 pageWeight and HeiaghtNikki LauretaNo ratings yet
- Ocular Manifestations of Connective Tissue Disorders: A Descriptive Cross Sectional StudyDocument4 pagesOcular Manifestations of Connective Tissue Disorders: A Descriptive Cross Sectional StudyIJAR JOURNALNo ratings yet
- National Immunization Schedule (NIS) : For Infants, Children and Pregnant WomenDocument13 pagesNational Immunization Schedule (NIS) : For Infants, Children and Pregnant WomenPrabir Kumar Chatterjee100% (1)
- 2010 - 3 Idsp Detail Information BKDocument73 pages2010 - 3 Idsp Detail Information BKPankaj ModhNo ratings yet
- Non Follicular PyodermaDocument1 pageNon Follicular PyodermaMagNo ratings yet
- Novartis Annual Report 2014 Pipeline InnovationDocument3 pagesNovartis Annual Report 2014 Pipeline InnovationFauzan FikriNo ratings yet
- Epi PowerpointDocument29 pagesEpi PowerpointFelisa Lacsamana Gregorio100% (3)
- MeaslesDocument32 pagesMeaslesYum C100% (2)
- 8th April 2012 IssueDocument4 pages8th April 2012 IssuebcmbtNo ratings yet
- Test Bank For Nursing For Wellness in Older Adults 8th Edition Carol A MillerDocument24 pagesTest Bank For Nursing For Wellness in Older Adults 8th Edition Carol A Millerjosehouseifgjseprtn100% (40)