You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Surgery 3 White Part 1Document87 pagesSurgery 3 White Part 1Håíthãm KhãtïßNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- YY תרגול כיתתי- גדילה, תזונה ומטבוליזם PDFDocument125 pagesYY תרגול כיתתי- גדילה, תזונה ומטבוליזם PDFHåíthãm KhãtïßNo ratings yet
- Ministry of Health Price List For Ambulatory and Hospitalization ServicesDocument40 pagesMinistry of Health Price List For Ambulatory and Hospitalization ServicesHåíthãm KhãtïßNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Zarif Qaraqra English Section, Seria A, 6 Group 1, 2020 - 2021Document3 pagesZarif Qaraqra English Section, Seria A, 6 Group 1, 2020 - 2021Håíthãm KhãtïßNo ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Surgery 2 PDFDocument176 pagesSurgery 2 PDFHåíthãm KhãtïßNo ratings yet
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Ministry of Health Price List For Ambulatory and Hospitalization ServicesDocument49 pagesMinistry of Health Price List For Ambulatory and Hospitalization ServicesHåíthãm KhãtïßNo ratings yet
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Goal:: Practical Activity in Clinic (Oncalls)Document60 pagesGoal:: Practical Activity in Clinic (Oncalls)Håíthãm KhãtïßNo ratings yet
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Hepatitis B Vaccine: Dosage Forms & StrengthsDocument3 pagesHepatitis B Vaccine: Dosage Forms & StrengthsHåíthãm KhãtïßNo ratings yet
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- 3 Tier Drug List: CaliforniaDocument154 pages3 Tier Drug List: CaliforniaHåíthãm KhãtïßNo ratings yet
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Abc of Drug 1Document130 pagesAbc of Drug 1Håíthãm KhãtïßNo ratings yet
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hepatitis A VaccineDocument5 pagesHepatitis A VaccineHåíthãm KhãtïßNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Breast CancerDocument53 pagesBreast Cancersmbala100% (1)
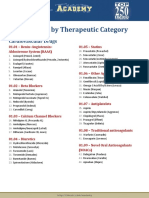
- Drug List by Therapeutic Category: Cardiovascular DrugsDocument7 pagesDrug List by Therapeutic Category: Cardiovascular DrugsAloah122346No ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Neisseria Genus EnglDocument127 pagesNeisseria Genus EnglHåíthãm KhãtïßNo ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- 5 DR Farhat MoazamDocument9 pages5 DR Farhat MoazamHåíthãm KhãtïßNo ratings yet
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Curs Epitelii EnglezaDocument50 pagesCurs Epitelii EnglezaHåíthãm KhãtïßNo ratings yet
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Genetic DiseasesDocument43 pagesGenetic DiseasesAisha BirdNo ratings yet
- Immune System Has Two Lines of Defense:: A. Innate (Non Specific) ImmunityDocument105 pagesImmune System Has Two Lines of Defense:: A. Innate (Non Specific) ImmunityHåíthãm KhãtïßNo ratings yet
- Connective Tissue HistologyDocument12 pagesConnective Tissue HistologyHåíthãm KhãtïßNo ratings yet
- Curs 3 Lecture Nutrition and Bacteria CultivationDocument74 pagesCurs 3 Lecture Nutrition and Bacteria CultivationHåíthãm KhãtïßNo ratings yet
- Genetic DiseasesDocument43 pagesGenetic DiseasesAisha BirdNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Goal:: Practical Activity in Clinic (Oncalls)Document60 pagesGoal:: Practical Activity in Clinic (Oncalls)Håíthãm KhãtïßNo ratings yet
- Breast Slide DeckDocument34 pagesBreast Slide DeckJane ViNo ratings yet
- Corynebacterium Listeria EnlgDocument97 pagesCorynebacterium Listeria EnlgHåíthãm KhãtïßNo ratings yet
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Abiliti 2Document68 pagesAbiliti 2Håíthãm KhãtïßNo ratings yet
- VaksinasiDocument54 pagesVaksinasinikeNo ratings yet
- Curs 1 - 2 EnglDocument213 pagesCurs 1 - 2 EnglHåíthãm KhãtïßNo ratings yet
- Breast CancerDocument52 pagesBreast CancerazharyekaputraNo ratings yet
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (120)
- Automated External Defibrillation - A0Document1 pageAutomated External Defibrillation - A0Håíthãm KhãtïßNo ratings yet
- Job Hazard AnalysisDocument35 pagesJob Hazard AnalysisMichael NullasNo ratings yet
- Apley & Solomon's Fraktur ClaviculaDocument3 pagesApley & Solomon's Fraktur ClaviculaChiki CacaNo ratings yet
- Chapter 5 Physical InjuryDocument12 pagesChapter 5 Physical InjuryJm LanabanNo ratings yet
- V63N1A08Document7 pagesV63N1A08Carolina JozamiNo ratings yet
- Daftar Kode Diagnosis Dan TindakanDocument2 pagesDaftar Kode Diagnosis Dan TindakanDita RatnasariNo ratings yet
- Update On Treatment - TFCC Tears: Dr. Jai SungaranDocument8 pagesUpdate On Treatment - TFCC Tears: Dr. Jai SungaranLaineyNo ratings yet
- Adult Questions FinalDocument7 pagesAdult Questions FinalHasan A AsFourNo ratings yet
- ALWEE ALYWIN AZLIM v. MUHAMMAD SHAHID MOHD. TOHADocument23 pagesALWEE ALYWIN AZLIM v. MUHAMMAD SHAHID MOHD. TOHAmerNo ratings yet
- 023 HSE-WP-2023-023-YAK (PIPING INSTALLATION) - Approved N SignedDocument30 pages023 HSE-WP-2023-023-YAK (PIPING INSTALLATION) - Approved N SignedsyamilNo ratings yet
- X PROCEDURAL SKILLS AND OTHERSDocument9 pagesX PROCEDURAL SKILLS AND OTHERSWilson Ong Ying FaNo ratings yet
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Skeletal SystemDocument24 pagesThe Skeletal SystemAlexa100% (1)
- Vocab 2 BodypartsDocument2 pagesVocab 2 BodypartsDieu Linh100% (1)
- Syndesmosis GoodDocument35 pagesSyndesmosis GoodRoger WatersNo ratings yet
- 2002 YLR 2117 - GHULAM QADIR Versus THE STATE - LAHORE HIGH COURT LAHOREDocument11 pages2002 YLR 2117 - GHULAM QADIR Versus THE STATE - LAHORE HIGH COURT LAHOREFarwan AkhtarNo ratings yet
- Risk Assessment For Electrical Equipment InstalationDocument15 pagesRisk Assessment For Electrical Equipment Instalationmanikandan100% (2)
- MOS - Fire FightingDocument23 pagesMOS - Fire FightingMohammad Hadoumi SaldanNo ratings yet
- Craniofacial PainDocument12 pagesCraniofacial PainJyothsna YelpulaNo ratings yet
- Studyprotocol Open AccessDocument14 pagesStudyprotocol Open AccessMahmoud El MohamdyNo ratings yet
- First Aid QuizDocument10 pagesFirst Aid QuizLavern CharleryNo ratings yet
- CV DR Dehnadi 14 Nov 22Document5 pagesCV DR Dehnadi 14 Nov 22mohammadrezahajian12191No ratings yet
- Craniotomy: Craniectomy / CranioplastyDocument30 pagesCraniotomy: Craniectomy / CranioplastyYuji TanakaNo ratings yet
- May 2016 Exam ReportDocument16 pagesMay 2016 Exam ReportJane KoNo ratings yet
- AN Outline To Bones and Tissue Injuries Management - 4 PDFDocument70 pagesAN Outline To Bones and Tissue Injuries Management - 4 PDFAlphamaleagainNo ratings yet
- 140b-56109667-Standing Supported Left Glute Push Clinical ReasoningDocument2 pages140b-56109667-Standing Supported Left Glute Push Clinical ReasoningAbhishek VermaNo ratings yet
- Nursing Care Plan PainDocument2 pagesNursing Care Plan Painjanmarc goreroNo ratings yet
- ADSMC Services (ADSafety) SO2 - BOSH ModuleDocument180 pagesADSMC Services (ADSafety) SO2 - BOSH Modulebeng acostaNo ratings yet
- Muscles of The Dog 2: 2012 Martin Cake, Murdoch UniversityDocument11 pagesMuscles of The Dog 2: 2012 Martin Cake, Murdoch UniversityPiereNo ratings yet
- Medical Guidelines of Sick Leaves DurationDocument19 pagesMedical Guidelines of Sick Leaves Durationousama aklanNo ratings yet
- 7 Patellar Tracking Exercises For Subluxation & DislocationDocument9 pages7 Patellar Tracking Exercises For Subluxation & DislocationAnh Đức NguyễnNo ratings yet
- Sanjana S. Zad, Pragati PatilDocument15 pagesSanjana S. Zad, Pragati PatilAquaNo ratings yet