You might also like
- The Ultrasound PractitionerDocument32 pagesThe Ultrasound PractitionerWebster The-TechGuy Lungu100% (1)
- Medical DirectiveDocument3 pagesMedical DirectiveShiv Raj MathurNo ratings yet
- Ravi Kannaiyan: QC Inspection EngineerDocument5 pagesRavi Kannaiyan: QC Inspection EngineerVinoth BalaNo ratings yet
- Cleaningvssanitizingservsafe1583366413072 PDFDocument2 pagesCleaningvssanitizingservsafe1583366413072 PDFHenry SNo ratings yet
- Kennedy-Model of Exemplary Midwifery PracticeDocument16 pagesKennedy-Model of Exemplary Midwifery PracticeAnonymous bq4KY0mcWGNo ratings yet
- Work Environment SOP Free TemplateDocument2 pagesWork Environment SOP Free TemplateIftikhar KhanNo ratings yet
- Robert W. Schrier - Atlas of Diseases of The Kidney Volume 01 PDFDocument316 pagesRobert W. Schrier - Atlas of Diseases of The Kidney Volume 01 PDFAtu Oana100% (3)
- The Role of The Enrolled Nursing Auxiliary in A Selected Health Care AdministrationDocument5 pagesThe Role of The Enrolled Nursing Auxiliary in A Selected Health Care AdministrationhoifishNo ratings yet
- Barriers To Effective PARU Handover: ACORN December 2010Document6 pagesBarriers To Effective PARU Handover: ACORN December 2010Pebri IrawanNo ratings yet
- Team Triage Improves Emergency Department EfficiencyDocument3 pagesTeam Triage Improves Emergency Department EfficiencyAbdi Agus YouandiNo ratings yet
- Research: Interpreting AccountabilityDocument76 pagesResearch: Interpreting AccountabilitySubin AugustineNo ratings yet
- Allocation of Physician Time in Ambulatory Practice: A Time and Motion Study in 4 SpecialtiesDocument10 pagesAllocation of Physician Time in Ambulatory Practice: A Time and Motion Study in 4 SpecialtiesMonica CabaNo ratings yet
- Busby 1992Document9 pagesBusby 1992Anonymous 6DyD7ZDCNENo ratings yet
- Can The Nurse Do Folliculometry in Acceptable Agreement As Infertilityclinicians First Part of Ongoing Training ProgramDocument9 pagesCan The Nurse Do Folliculometry in Acceptable Agreement As Infertilityclinicians First Part of Ongoing Training Programrichardong lauNo ratings yet
- Literature Review of Studies On The Effectiveness of Nurses Ability To Order and Interpret X-RaysDocument8 pagesLiterature Review of Studies On The Effectiveness of Nurses Ability To Order and Interpret X-RaysFlorsie MirandaNo ratings yet
- Journal MedicalDocument9 pagesJournal Medicalreynosa chavezNo ratings yet
- Nurse-Led Care in Dermatology: A Review of The Literature: CorrespondenceDocument6 pagesNurse-Led Care in Dermatology: A Review of The Literature: CorrespondenceafbmgNo ratings yet
- International Emergency Nursing: SciencedirectDocument7 pagesInternational Emergency Nursing: SciencedirectWulan dariNo ratings yet
- Questionnaire Survey On Use of Placebo: PapersDocument3 pagesQuestionnaire Survey On Use of Placebo: PapersShahzadNo ratings yet
- Emerg Med J-2004-Subash-542-4 PDFDocument4 pagesEmerg Med J-2004-Subash-542-4 PDFSriatiNo ratings yet
- Review On SymstaticDocument12 pagesReview On SymstaticJeppeye Tan MasongNo ratings yet
- Acupuncturist Perceptions of Serving As A Clinical Trial PractitionerDocument7 pagesAcupuncturist Perceptions of Serving As A Clinical Trial Practitionerbinglei chenNo ratings yet
- 1472 6882 12 88Document9 pages1472 6882 12 88Doctora SantanaNo ratings yet
- Individu AzaDocument5 pagesIndividu AzaZachya IslamiaNo ratings yet
- Why Nurses Are LeavingDocument7 pagesWhy Nurses Are LeavingAroon ErmaNo ratings yet
- Registered and Enrolled Nurses' Experiences of Ethical Issues in Nursing PracticeDocument7 pagesRegistered and Enrolled Nurses' Experiences of Ethical Issues in Nursing PracticeMeyar Y. Abu AsadNo ratings yet
- Role in Complex Patient Management: Hypertension: The Nurse Practitioner'SDocument8 pagesRole in Complex Patient Management: Hypertension: The Nurse Practitioner'SIndah SundariNo ratings yet
- Impact of Supervision and Self-Assessment On Doctor-Patient Communication in Rural MexicoDocument9 pagesImpact of Supervision and Self-Assessment On Doctor-Patient Communication in Rural MexicoUtari UbNo ratings yet
- Medication Administration Errors: Understanding The Issues: ArticleDocument10 pagesMedication Administration Errors: Understanding The Issues: Articleahmad afridiNo ratings yet
- Pri 328Document11 pagesPri 328Daniel DeinarovičNo ratings yet
- Artikel 4 PDFDocument3 pagesArtikel 4 PDFhariet rinancyNo ratings yet
- Factors Influencing Evidence-Based Practice Among Community NursesDocument5 pagesFactors Influencing Evidence-Based Practice Among Community NursesIlvita MayasariNo ratings yet
- International Emergency Nursing: Karen Hammad, Lingli Peng, Olga Anikeeva, Paul Arbon, Huiyun Du, Yinglan LiDocument5 pagesInternational Emergency Nursing: Karen Hammad, Lingli Peng, Olga Anikeeva, Paul Arbon, Huiyun Du, Yinglan LiRuly AryaNo ratings yet
- Nursing Handoffs A Systematic Review of The.26Document11 pagesNursing Handoffs A Systematic Review of The.26Zoa Ng Wai Kwan100% (2)
- Requested FileDocument6 pagesRequested FilekitsilcNo ratings yet
- Rle Journal MackinnonDocument4 pagesRle Journal MackinnonAllyssa MackinnonNo ratings yet
- Collaboration Between Family Physicians and Nurse CliniciansDocument8 pagesCollaboration Between Family Physicians and Nurse CliniciansRafa AssidiqNo ratings yet
- Training Using Simulation in Internal Medicine Residencies: An Educational PerspectiveDocument3 pagesTraining Using Simulation in Internal Medicine Residencies: An Educational PerspectiveagaetioNo ratings yet
- Predictors of Research Utilization Among Jordanian Registered Nurses: A Descriptive Correlational StudyDocument9 pagesPredictors of Research Utilization Among Jordanian Registered Nurses: A Descriptive Correlational Studysumaia abuhatabNo ratings yet
- Nagah 4Document12 pagesNagah 4karimam rroshdNo ratings yet
- J Nursing Management - 2017 - Schenk - Time Motion Analysis of Nursing Work in ICU Telemetry and Medical Surgical UnitsDocument7 pagesJ Nursing Management - 2017 - Schenk - Time Motion Analysis of Nursing Work in ICU Telemetry and Medical Surgical UnitsKhristel ZavaletaNo ratings yet
- Comprehensive Discharge Planning-Ebp PowerpointDocument45 pagesComprehensive Discharge Planning-Ebp Powerpointapi-24187790No ratings yet
- The Causes of Prescribing Errors in English General PracticesDocument8 pagesThe Causes of Prescribing Errors in English General PracticesrosianaNo ratings yet
- Jurnal KesehatanDocument11 pagesJurnal KesehatanesidianauttariNo ratings yet
- Use of and Attitudes Toward Complementary and Alternative Medicine Among Nurse-Midwives in IsraelDocument7 pagesUse of and Attitudes Toward Complementary and Alternative Medicine Among Nurse-Midwives in IsraelEndahNo ratings yet
- Discharge Planing Critical CareDocument9 pagesDischarge Planing Critical CareBayu Akbar KhayudinNo ratings yet
- Daily: The Introduction of Evidencesbased Component PracticeDocument4 pagesDaily: The Introduction of Evidencesbased Component PracticeuncleadolphNo ratings yet
- Am J Crit Care 2006 Scott 30 7Document9 pagesAm J Crit Care 2006 Scott 30 7dasfkjkNo ratings yet
- Cost Consequences StudyDocument4 pagesCost Consequences StudySankita SandalNo ratings yet
- A Conceptual Framefwork For Home NursingDocument8 pagesA Conceptual Framefwork For Home NursingNur Inayah IsmaniarNo ratings yet
- Murphy 2008Document8 pagesMurphy 2008Ajup SafarudinNo ratings yet
- 02 Review of LiteratureDocument8 pages02 Review of LiteratureAnnapoorna SHNo ratings yet
- Nursing Attitudes and BeliefsDocument5 pagesNursing Attitudes and Beliefsyovanimanuel imanuelNo ratings yet
- Dok PerilakuDocument15 pagesDok PerilakuNURHAFNI HARAHAPNo ratings yet
- Bedside Nursing Handover A Case StudyDocument8 pagesBedside Nursing Handover A Case StudyAisha MagarangNo ratings yet
- CH 01 PDFDocument25 pagesCH 01 PDFkikiNo ratings yet
- Time Management Strategies in Nursing Practice: Susan WaterworthDocument10 pagesTime Management Strategies in Nursing Practice: Susan WaterworthClarisse AcacioNo ratings yet
- Relationship of Nurses' Assessment of Organizational Culture, Job Satisfaction, and Patient Satisfaction With Nursing CareDocument6 pagesRelationship of Nurses' Assessment of Organizational Culture, Job Satisfaction, and Patient Satisfaction With Nursing CareFalensia MARSNo ratings yet
- Recognition of Clinical Deterioration, A Clinical Leadership Opportunity For Nurse ExecutiveDocument6 pagesRecognition of Clinical Deterioration, A Clinical Leadership Opportunity For Nurse ExecutivePAULA SORAIA CHENNo ratings yet
- Ma. Bernardita v. VillaruelDocument184 pagesMa. Bernardita v. VillaruelJeffreydanceljr100% (3)
- Chapter 5Document42 pagesChapter 5Yuuki Chitose (tai-kun)No ratings yet
- Patient Perceptions of Emergency Department Fast Track: A Prospective Pilot Study Comparing Two Models of CareDocument3 pagesPatient Perceptions of Emergency Department Fast Track: A Prospective Pilot Study Comparing Two Models of CareErvin WidhiantyasNo ratings yet
- 414 IJAR 2663 Nursing Process With Cover Page v2Document17 pages414 IJAR 2663 Nursing Process With Cover Page v2Dinda Dwi PermataNo ratings yet
- Advanced Practice and Leadership in Radiology NursingFrom EverandAdvanced Practice and Leadership in Radiology NursingKathleen A. GrossNo ratings yet
- Eustachian TubeDocument6 pagesEustachian TubeNaruto_Uchiha777No ratings yet
- School of Medical Sciences Kathmandu UniversityDocument6 pagesSchool of Medical Sciences Kathmandu Universitysuyog raj gautamNo ratings yet
- Mental Wellness PSA 3Document15 pagesMental Wellness PSA 3Romarate, FranzineNo ratings yet
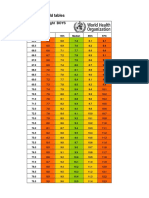
- Boys Simplified Field Tables Weight For Length 2 To 5 Years (Percentiles)Document4 pagesBoys Simplified Field Tables Weight For Length 2 To 5 Years (Percentiles)Gabrielly LopesNo ratings yet
- SJODR 48 555 556 CDocument2 pagesSJODR 48 555 556 Cyasser bedirNo ratings yet
- Republic of The Philippines Central Mindanao University College of NURSING University Town, Musuan, Maramag, BukidnonDocument2 pagesRepublic of The Philippines Central Mindanao University College of NURSING University Town, Musuan, Maramag, BukidnonJastine SabornidoNo ratings yet
- IGDDocument210 pagesIGDUlfa KurniasihNo ratings yet
- Pengaruh Senam Rematik Terhadap Skala Nyeri: Rheumatoid Arthritis Pada LansiaDocument7 pagesPengaruh Senam Rematik Terhadap Skala Nyeri: Rheumatoid Arthritis Pada LansiaDinaliza UtamiNo ratings yet
- T27208AQCDocument1 pageT27208AQCpiagiopersempreNo ratings yet
- Podcast Call SheetDocument2 pagesPodcast Call Sheetapi-632200301No ratings yet
- Communication Breakdown at City HospitalDocument3 pagesCommunication Breakdown at City HospitalSiddhartha AhluwaliaNo ratings yet
- Lesson Plan A2 Edexcel 2018 - 2019 - FinalDocument4 pagesLesson Plan A2 Edexcel 2018 - 2019 - FinalMilka RahmanNo ratings yet
- 12 Lead Ecg Application FormDocument2 pages12 Lead Ecg Application Formmuzammil1No ratings yet
- Module B - Lesson 3Document14 pagesModule B - Lesson 3Melanie CortezNo ratings yet
- Administering Intradermal InjectionDocument17 pagesAdministering Intradermal InjectionPattNo ratings yet
- St. Croix County Jail Bookings For Sept. 9Document3 pagesSt. Croix County Jail Bookings For Sept. 9EastMetroPatchNo ratings yet
- EDUC-5420 - Week 1# Written AssignmentDocument7 pagesEDUC-5420 - Week 1# Written AssignmentShivaniNo ratings yet
- Summer and Winter VacationsDocument5 pagesSummer and Winter VacationsYahia IdressNo ratings yet
- Operating RoomDocument13 pagesOperating RoomrichardNo ratings yet
- Alumunium Chlorohydrate: Material Safety Data SheetDocument4 pagesAlumunium Chlorohydrate: Material Safety Data Sheethinur awaNo ratings yet
- Dry Lab Exercise 4 EndocrineDocument4 pagesDry Lab Exercise 4 Endocrine06Fajrian RidhatunnisaNo ratings yet
- Cumulative Adversity As A Correlate of Posttraumatic GrowthDocument20 pagesCumulative Adversity As A Correlate of Posttraumatic GrowthLorena RodríguezNo ratings yet
- Text of The Timothy J. Barber ActDocument2 pagesText of The Timothy J. Barber ActThe Livingston County NewsNo ratings yet
- Meniere DiseaseDocument6 pagesMeniere Diseasefirza yoga baskoroNo ratings yet
- Clinical Image - Max 1st MolarDocument2 pagesClinical Image - Max 1st MolarShriya SingiNo ratings yet