You might also like
- Awareness of Effects of Sleep Deprivation Among College StudentsDocument4 pagesAwareness of Effects of Sleep Deprivation Among College StudentsSEAN KENZO SULITNo ratings yet
- Shovels and Shields: A Knight Class Guide On The Spade Wielding Hero in Blue and CompanyDocument19 pagesShovels and Shields: A Knight Class Guide On The Spade Wielding Hero in Blue and Companyjeff fejjNo ratings yet
- Sleep and Electronic DevicesDocument7 pagesSleep and Electronic DevicesCarlos Olivera LópezNo ratings yet
- Jurnal 5Document28 pagesJurnal 5dwi putri ratehNo ratings yet
- BRUNBORG Et Al-2011-Journal of Sleep ResearchDocument7 pagesBRUNBORG Et Al-2011-Journal of Sleep ResearchAndhika CahyaNo ratings yet
- Media Use and Sleep in Teenagers What Do We KnowDocument7 pagesMedia Use and Sleep in Teenagers What Do We KnowMichelle OnozaNo ratings yet
- Adolescents' Electronic Media Use at Night, Sleep Disturbance, and Depressive Symptoms in The Smartphone AgeDocument14 pagesAdolescents' Electronic Media Use at Night, Sleep Disturbance, and Depressive Symptoms in The Smartphone AgemariskaNo ratings yet
- The Use of Technology at Night Impact On Sleep and HealthDocument2 pagesThe Use of Technology at Night Impact On Sleep and HealthSan RNo ratings yet
- The Association Between Use of Mobile Phones After Lights Out and Sleep Disturbances Among Japanese Adolescents: A Nationwide Cross-Sectional SurveyDocument12 pagesThe Association Between Use of Mobile Phones After Lights Out and Sleep Disturbances Among Japanese Adolescents: A Nationwide Cross-Sectional SurveyMutiara Pertiwi Part IINo ratings yet
- Efek HP Terhadap Kualitas TidurDocument9 pagesEfek HP Terhadap Kualitas TidurKaroniNo ratings yet
- Accepted Manuscript: Sleep MedicineDocument29 pagesAccepted Manuscript: Sleep Medicinedwi putri ratehNo ratings yet
- Pone 0276226Document14 pagesPone 0276226Yussika FernandaNo ratings yet
- Ana 4. Adolescent SleepDocument7 pagesAna 4. Adolescent SleepAlfredo CastilloNo ratings yet
- The Impact of Cyberspace Usage Affecting Sleep DeprivationDocument8 pagesThe Impact of Cyberspace Usage Affecting Sleep DeprivationYeh HeetNo ratings yet
- Journal of Sleep Research - 2023 - Dibben - Adolescents Interactive Electronic Device Use Sleep and Mental Health ADocument18 pagesJournal of Sleep Research - 2023 - Dibben - Adolescents Interactive Electronic Device Use Sleep and Mental Health AneiralejandroblpNo ratings yet
- 1 s2.0 S1087079214000811 MainDocument9 pages1 s2.0 S1087079214000811 Mainm67arthaNo ratings yet
- Investigating The Effects of Electronic Devices On Sleeping HabitsDocument4 pagesInvestigating The Effects of Electronic Devices On Sleeping HabitsJayReneNo ratings yet
- Effect of Electronics To SleepDocument10 pagesEffect of Electronics To SleephonorableekouoNo ratings yet
- 48 Aktsa Original 12 3Document10 pages48 Aktsa Original 12 3alifia shafa s psiNo ratings yet
- Compiledannotations 2Document8 pagesCompiledannotations 2api-320970548No ratings yet
- Oamjms 9b 297Document4 pagesOamjms 9b 297Matt FlorendoNo ratings yet
- The Role of Environmental Factors On Sleep Patterns and School Performance in AdolescentsDocument9 pagesThe Role of Environmental Factors On Sleep Patterns and School Performance in AdolescentsJim HawkinsNo ratings yet
- Evening Use of Light-Emitting Ereaders Negatively Affects Sleep, Circadian Timing, and Next-Morning AlertnessDocument6 pagesEvening Use of Light-Emitting Ereaders Negatively Affects Sleep, Circadian Timing, and Next-Morning AlertnessPawan KumarNo ratings yet
- STEM12B - GROUP5 - TopicManuscript 2 1 1 1 1Document5 pagesSTEM12B - GROUP5 - TopicManuscript 2 1 1 1 1Allysa Nicole GuerreroNo ratings yet
- Pediatrics TvysueñoDocument7 pagesPediatrics TvysueñoFrancia Elena Rocha VasquezNo ratings yet
- Uso Noturno Do CelularDocument8 pagesUso Noturno Do CelularLídia SouzaNo ratings yet
- Adolescents With A Smartphone Sleep Less Than Their PeersDocument7 pagesAdolescents With A Smartphone Sleep Less Than Their PeersS PronNo ratings yet
- Correction EFFECT OF ELECTRONICS TO SLEEPDocument10 pagesCorrection EFFECT OF ELECTRONICS TO SLEEPhonorableekouoNo ratings yet
- Significance of The StudyDocument6 pagesSignificance of The StudyLauren FeiNo ratings yet
- Protective and Risk Factors For Adolescent Sleep - A Meta-Analytic ReviewDocument14 pagesProtective and Risk Factors For Adolescent Sleep - A Meta-Analytic ReviewJust a GirlNo ratings yet
- PR 1Document17 pagesPR 1ajgars175No ratings yet
- Fpsyt 12 629407Document10 pagesFpsyt 12 629407Syed SalmanNo ratings yet
- Electronic Media Use and Sleep in School Aged Children and AdolescentsDocument8 pagesElectronic Media Use and Sleep in School Aged Children and AdolescentspattyeateatNo ratings yet
- HBM 39 4471Document9 pagesHBM 39 4471Pedro Henrique Ramos De SouzaNo ratings yet
- Internet Addiction and Sleep Disturbance20151208 27534 Susfx4 With Cover PageDocument5 pagesInternet Addiction and Sleep Disturbance20151208 27534 Susfx4 With Cover PageFirdani MutiaraNo ratings yet
- Sleep Deprivation - Its Effect To YNHS Tech-Voc StudentsDocument62 pagesSleep Deprivation - Its Effect To YNHS Tech-Voc StudentsBonggot LadyAntonietteNo ratings yet
- Changes of Evening Exposure To Electronic Devices During The COVID-19 Lockdown Affect The Time Course of Sleep DisturbancesDocument9 pagesChanges of Evening Exposure To Electronic Devices During The COVID-19 Lockdown Affect The Time Course of Sleep Disturbancesfita9candraNo ratings yet
- 207 Research Proposal 1Document10 pages207 Research Proposal 1Jana WeshahiNo ratings yet
- Evening Use of Light-Emitting Ereaders Negatively Affects Sleep, Circadian Timing, and Next-Morning AlertnessDocument6 pagesEvening Use of Light-Emitting Ereaders Negatively Affects Sleep, Circadian Timing, and Next-Morning AlertnessccrrzzNo ratings yet
- CHAPTER-1-5-PR2-G12Document43 pagesCHAPTER-1-5-PR2-G12docosinvonNo ratings yet
- ADHD and Screen Time Case StudyDocument9 pagesADHD and Screen Time Case StudyMerwinNo ratings yet
- Impact of Different Pre-Sleep Phone Use Patterns On Sleep QualityDocument4 pagesImpact of Different Pre-Sleep Phone Use Patterns On Sleep QualityFizza ChNo ratings yet
- Ewc 661 ProposalDocument9 pagesEwc 661 ProposalLuqman AriefNo ratings yet
- Television Viewing, Computer Game Playing, and Internet Use and Self-Reported Time To Bed and Time Out of Bed in Secondary-School ChildrenDocument4 pagesTelevision Viewing, Computer Game Playing, and Internet Use and Self-Reported Time To Bed and Time Out of Bed in Secondary-School ChildrenSyahrul AminNo ratings yet
- Community Medicine Research 2.5.23..2Document11 pagesCommunity Medicine Research 2.5.23..2YadhuNo ratings yet
- StatsDocument10 pagesStatsAKSHITA BHARDWAJ 2239409No ratings yet
- Sleep Problems and Internet Addiction Among Children and Adolescents: A Longitudinal StudyDocument8 pagesSleep Problems and Internet Addiction Among Children and Adolescents: A Longitudinal StudySakshi SharmaNo ratings yet
- (2019) Adolescent Perceptions of Sleep and Influences On Sleep BehaviourDocument8 pages(2019) Adolescent Perceptions of Sleep and Influences On Sleep BehaviourFabian Opazo DelgadoNo ratings yet
- The ThesisDocument8 pagesThe ThesisTerraMonsta BlogspotNo ratings yet
- Impact of Digital Media On Sleep Pattern Disturbance in Medical and Nursing StudentsDocument7 pagesImpact of Digital Media On Sleep Pattern Disturbance in Medical and Nursing StudentsValarmathiNo ratings yet
- The Relationship Between A Night Usage of Mobile Phone and Sleep Habit and The Circadian Typology of Japanese Students Aged 18-30 Years PDFDocument12 pagesThe Relationship Between A Night Usage of Mobile Phone and Sleep Habit and The Circadian Typology of Japanese Students Aged 18-30 Years PDFAmalia Nur WahyuNo ratings yet
- Ijerph 17 07131Document11 pagesIjerph 17 07131Kusum DahalNo ratings yet
- Mobile App Development and Usability Research To Help Dementia and Alzheimer PatientsDocument7 pagesMobile App Development and Usability Research To Help Dementia and Alzheimer PatientsTakwa ZgayaNo ratings yet
- The Impact of Electronics On SleepDocument4 pagesThe Impact of Electronics On SleephonorableekouoNo ratings yet
- Final PR1Document11 pagesFinal PR1masillamakon3No ratings yet
- A23 1 FullDocument1 pageA23 1 FullYussika FernandaNo ratings yet
- Qualitative-Updated - Title-Approval-Form - GROUP 2Document5 pagesQualitative-Updated - Title-Approval-Form - GROUP 2kberrameNo ratings yet
- Internet Addiction and Sleep Problems A Systematic Review andDocument11 pagesInternet Addiction and Sleep Problems A Systematic Review andVanessa AldeaNo ratings yet
- BMC Public HealthDocument15 pagesBMC Public HealthLateecka R KulkarniNo ratings yet
- How Much Sleep Do We Need?Document26 pagesHow Much Sleep Do We Need?Arief UbaidillahNo ratings yet
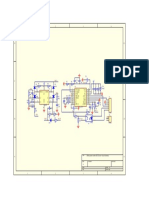
- DC DC Driver Circuit Schematic PDFDocument1 pageDC DC Driver Circuit Schematic PDFRyn YahuFNo ratings yet
- Bumuntu RulebookDocument8 pagesBumuntu RulebookJesse KahoaalohakūpaʻaNo ratings yet
- AoS SS Reference Rules 200928Document2 pagesAoS SS Reference Rules 200928GrayNo ratings yet
- You're Too Far AwayDocument1 pageYou're Too Far AwayAntonio Luiz PimentaNo ratings yet
- Miriam College Pe 104 (Volleyball) Midterm ExaminationDocument2 pagesMiriam College Pe 104 (Volleyball) Midterm ExaminationChloe UsaNo ratings yet
- Legends of Avallen - Quickstart GuideDocument43 pagesLegends of Avallen - Quickstart GuideDelares Plenny100% (1)
- Sprite Stacking ScriptDocument2 pagesSprite Stacking Scriptwilson palma samaniegoNo ratings yet
- Chess Openings PDFDocument12 pagesChess Openings PDFMurugananth ChockalingamNo ratings yet
- Upfront GamesDocument1 pageUpfront GamesZildjian TumbagaNo ratings yet
- IFRS Session 1 To 3Document40 pagesIFRS Session 1 To 3techna8No ratings yet
- 25K Dorks Good For AllDocument424 pages25K Dorks Good For AllAnibalNo ratings yet
- PobabilityDocument68 pagesPobabilityRamNagalNo ratings yet
- Fans Contributions - Alternate Maps, Variants, EtcDocument3 pagesFans Contributions - Alternate Maps, Variants, EtcRenish MehtaNo ratings yet
- Cthulhu - Death May Die - FAQ v2.0Document15 pagesCthulhu - Death May Die - FAQ v2.0Aurel BathmanNo ratings yet
- Duplicate Bridge Scoring: X X y yDocument3 pagesDuplicate Bridge Scoring: X X y ySELAMET SANTOSONo ratings yet
- Board Games As A Platform For Collaborative Learning: October 2016Document32 pagesBoard Games As A Platform For Collaborative Learning: October 2016SITI NURFARHANA HISAMUDINNo ratings yet
- Printyour: BracketsDocument1 pagePrintyour: BracketsKTLO NewsNo ratings yet
- ListndsDocument18 pagesListndsBejeweled LuigiGhostNo ratings yet
- ICE Enterprises - ICE3600 - MERP - Dunland and The Southern Misty MountainsDocument73 pagesICE Enterprises - ICE3600 - MERP - Dunland and The Southern Misty MountainsDavid Wilson100% (1)
- Egacy: George Fan's Layoff and OctogeddonDocument9 pagesEgacy: George Fan's Layoff and OctogeddonSrynnENo ratings yet
- Bill Nagler - ACAANDocument7 pagesBill Nagler - ACAANFacundoNo ratings yet
- Modular Magic ItemsDocument3 pagesModular Magic ItemsChristoffer MårtenssonNo ratings yet
- Scott Malthouse - Echoes of The LabyrinthDocument23 pagesScott Malthouse - Echoes of The Labyrinthpepe100% (1)
- School AttendanceDocument2 pagesSchool AttendanceIndra Kurniawan VanliNo ratings yet
- SC305 User and Programming ManualDocument14 pagesSC305 User and Programming Manualstefany M comun parionaNo ratings yet
- Literature Review SoccerDocument8 pagesLiterature Review Soccerafmzndvyddcoio100% (1)
- Blue Chevaliers Open 2023 Tournament PreviewDocument30 pagesBlue Chevaliers Open 2023 Tournament PreviewJayden Chua Qi Ze (Amkss)No ratings yet
- Darkest Night Tabletop Simulator RulesDocument16 pagesDarkest Night Tabletop Simulator RulespacopaquitoNo ratings yet
- 5e Cleric Domain - Moon - GM BinderDocument3 pages5e Cleric Domain - Moon - GM BinderChaeyeon KimNo ratings yet