You might also like
- Medical Terminology in A FLASH!Document66 pagesMedical Terminology in A FLASH!Martha Herr88% (16)
- EKG | ECG Interpretation. Everything You Need to Know about 12-Lead ECG/EKG InterpretationFrom EverandEKG | ECG Interpretation. Everything You Need to Know about 12-Lead ECG/EKG InterpretationRating: 3 out of 5 stars3/5 (1)
- Pro-Form 940s - Owner's ManualDocument16 pagesPro-Form 940s - Owner's ManualTaury83% (6)
- Cardiologia - EletrocardiografiaDocument40 pagesCardiologia - EletrocardiografiaDANIEL ALEJANDRONo ratings yet
- EcgDocument57 pagesEcgenii_ta100% (9)
- ECG InterpretationDocument1 pageECG InterpretationCecil-An DalanonNo ratings yet
- The 12-Lead Electrocardiogram for Nurses and Allied ProfessionalsFrom EverandThe 12-Lead Electrocardiogram for Nurses and Allied ProfessionalsNo ratings yet
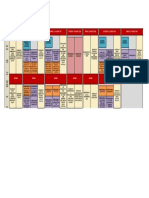
- Program at Glance WECOC 2021-Updated Juli 2021Document1 pageProgram at Glance WECOC 2021-Updated Juli 2021Bambang SupriadiNo ratings yet
- ECG MorphologyDocument36 pagesECG MorphologyMr Joko100% (2)
- Chapter 03Document13 pagesChapter 03matsliuNo ratings yet
- ECG Lesson 1Document5 pagesECG Lesson 1Marwan M.No ratings yet
- Ventricular Conduction Disturbances: Bundle Branch Blocks and Related AbnormalitiesDocument12 pagesVentricular Conduction Disturbances: Bundle Branch Blocks and Related AbnormalitiesFelipe GallardoNo ratings yet
- Electrical Axis and Axis Deviation: Fig. 6.1CDocument9 pagesElectrical Axis and Axis Deviation: Fig. 6.1CFelipe GallardoNo ratings yet
- ECG EKG InterpretationDocument11 pagesECG EKG InterpretationGunma AkagiNo ratings yet
- A Seminar On ECGDocument16 pagesA Seminar On ECGVibha C PrabhuNo ratings yet
- Electrical Conduction Pathway: Course Lesson Student Email Atika - Salsabila91@ui - Ac.idDocument12 pagesElectrical Conduction Pathway: Course Lesson Student Email Atika - Salsabila91@ui - Ac.idlemon kyuteaNo ratings yet
- Ecg (Ekg) : Dr. Jamal Dabbas Interventional Cardiologist & InternistDocument87 pagesEcg (Ekg) : Dr. Jamal Dabbas Interventional Cardiologist & Internistsara rababahNo ratings yet
- EKGDocument31 pagesEKGJay JiangNo ratings yet
- Ecg Reading Made EasyDocument59 pagesEcg Reading Made EasyAngealyn GaviolaNo ratings yet
- Electrocardiography: An Introduction To The ECGDocument76 pagesElectrocardiography: An Introduction To The ECGInnocent Clifford MaranduNo ratings yet
- Lecture 3c Interpretation of ECG - The Heart Model EM Theory & Applications II Spring Semester 2006Document27 pagesLecture 3c Interpretation of ECG - The Heart Model EM Theory & Applications II Spring Semester 2006hebaNo ratings yet
- Elektrokardiogramm) Is A Graphic Produced by An ElectrocardiographDocument5 pagesElektrokardiogramm) Is A Graphic Produced by An ElectrocardiographReverie ManalaysayNo ratings yet
- I. The Standard 12 Lead ECGDocument2 pagesI. The Standard 12 Lead ECGapi-376925250% (2)
- Conquering The ECGDocument25 pagesConquering The ECGPankaj PatilNo ratings yet
- Electrical Axis and Axis Deviation: Mean Qrs Axis: DefinitionDocument9 pagesElectrical Axis and Axis Deviation: Mean Qrs Axis: Definitionrocker_jadulNo ratings yet
- ECG Made Easy by Mallareddy SripujaDocument46 pagesECG Made Easy by Mallareddy Sripujagrreddy836100% (3)
- Strong's EKG Chamber Enlargement - DraftDocument12 pagesStrong's EKG Chamber Enlargement - DraftMonica GonzalezNo ratings yet
- Hypertrophy and Enlargement of The HeartDocument23 pagesHypertrophy and Enlargement of The HeartZion_MilgemNo ratings yet
- ECG 1 and 2 2012Document56 pagesECG 1 and 2 2012thomasNo ratings yet
- Qrs & Voltage: Dr. David D. Ariwibowo SPJP, FihaDocument14 pagesQrs & Voltage: Dr. David D. Ariwibowo SPJP, FihaJevisco LauNo ratings yet
- Membaca Ekg: Dr. Aritantri Darmayani, M.SC, SPPDDocument76 pagesMembaca Ekg: Dr. Aritantri Darmayani, M.SC, SPPDDekdesNo ratings yet
- Anatomy & Physiology of The Heart: Heart Lectrure, ECE4610, Z. Moussavi, Fall 2011Document8 pagesAnatomy & Physiology of The Heart: Heart Lectrure, ECE4610, Z. Moussavi, Fall 2011Gaoudam NatarajanNo ratings yet
- ECG Waves and Intervals Spatial Orientation of The 12 Lead ECGDocument31 pagesECG Waves and Intervals Spatial Orientation of The 12 Lead ECGiah_18No ratings yet
- 118 Skills Lab-Week 2-ECG TakingDocument8 pages118 Skills Lab-Week 2-ECG TakingKeisha BartolataNo ratings yet
- ECG 11 HikDocument21 pagesECG 11 Hikmdee02031999mNo ratings yet
- LdfısjlısDocument52 pagesLdfısjlısChristine HudginsNo ratings yet
- EcgDocument11 pagesEcgRajneesh TiwariNo ratings yet
- The P-Wave, PR Interval and PR SegmentDocument1 pageThe P-Wave, PR Interval and PR SegmentllocopoloNo ratings yet
- ECG Interpretation TheoryDocument4 pagesECG Interpretation TheorySteph PiperNo ratings yet
- Auskultation. ECG - LastDocument5 pagesAuskultation. ECG - LastAndreyNo ratings yet
- ECG - Module - Printable Analysis and Interpretation of ECGDocument37 pagesECG - Module - Printable Analysis and Interpretation of ECGPankaj PatilNo ratings yet
- Left Anterior Fascicular Block Left Posterior Fascicular BlockDocument1 pageLeft Anterior Fascicular Block Left Posterior Fascicular BlockLwin Maung Maung ThikeNo ratings yet
- 12electrocardiogram Part 1Document18 pages12electrocardiogram Part 1Jaydave PatelNo ratings yet
- 4 07introtoecg PDFDocument16 pages4 07introtoecg PDFPatricia SanchezNo ratings yet
- Bimbingan Ekg r1Document76 pagesBimbingan Ekg r1lintang andilaNo ratings yet
- 5 - EcgDocument37 pages5 - EcgMonika MeriyaNo ratings yet
- Introduction To ECG Interpretation January 2023Document101 pagesIntroduction To ECG Interpretation January 2023davidjoejoekidNo ratings yet
- Deconstructing The ECG Curve - The Components of The Tracing: Key ConceptsDocument117 pagesDeconstructing The ECG Curve - The Components of The Tracing: Key ConceptsdrynwhylNo ratings yet
- ECG InerpretitionDocument12 pagesECG InerpretitionMended_Heart100% (6)
- How To Read An ECGDocument15 pagesHow To Read An ECGCFTCNo ratings yet
- Electrocardiography Basic: DR Budi EnochDocument49 pagesElectrocardiography Basic: DR Budi EnochYohanes Malindo Wiyaa DBs-uno100% (1)
- ECG PracticalDocument48 pagesECG PracticalbvkjtzrvnyNo ratings yet
- EKG Basics - LongDocument40 pagesEKG Basics - Longمحمد خالدNo ratings yet
- ECG With ImageDocument7 pagesECG With ImagemathavanNo ratings yet
- Electrocardiography: DR Budi EnochDocument115 pagesElectrocardiography: DR Budi EnochAriyanaNo ratings yet
- ECG Made EasyDocument82 pagesECG Made EasyBobby SodhiNo ratings yet
- EKG Interpretation Basics Guide: Electrocardiogram Heart Rate Determination, Arrhythmia, Cardiac Dysrhythmia, Heart Block Causes, Symptoms, Identification and Medical Treatment Nursing HandbookFrom EverandEKG Interpretation Basics Guide: Electrocardiogram Heart Rate Determination, Arrhythmia, Cardiac Dysrhythmia, Heart Block Causes, Symptoms, Identification and Medical Treatment Nursing HandbookNo ratings yet
- MI2 TP6 Artículo VFCDocument6 pagesMI2 TP6 Artículo VFCFelipe GallardoNo ratings yet
- MI2 TP6 Artículo Alerta PDFDocument8 pagesMI2 TP6 Artículo Alerta PDFFelipe GallardoNo ratings yet
- MI2 TP6 Artículo Actigrafía PDFDocument12 pagesMI2 TP6 Artículo Actigrafía PDFFelipe GallardoNo ratings yet
- MI2 TP6 Artículo Temperatura PDFDocument9 pagesMI2 TP6 Artículo Temperatura PDFFelipe GallardoNo ratings yet
- ECG Leads: Bipolar Limb Leads (I, II, and Unipolar Limb Leads (aVRDocument11 pagesECG Leads: Bipolar Limb Leads (I, II, and Unipolar Limb Leads (aVRFelipe GallardoNo ratings yet
- Myocardial Ischemia and Infarction, Part I: ST Segment Elevation and Q Wave SyndromesDocument19 pagesMyocardial Ischemia and Infarction, Part I: ST Segment Elevation and Q Wave SyndromesFelipe GallardoNo ratings yet
- Electrical Axis and Axis Deviation: Fig. 6.1CDocument9 pagesElectrical Axis and Axis Deviation: Fig. 6.1CFelipe GallardoNo ratings yet
- Sepsis 2018Document9 pagesSepsis 2018Gianfranco Tovar Calderón100% (1)
- Perdarahan PeripartumDocument8 pagesPerdarahan PeripartumSuhatman AhNo ratings yet
- NCP Activity Intolerance (HTN Crisis)Document3 pagesNCP Activity Intolerance (HTN Crisis)Jenny AjocNo ratings yet
- MOR-FREE 569 + Coreactant C-99 ENDocument4 pagesMOR-FREE 569 + Coreactant C-99 ENMohit100% (1)
- CV By, Yvette02Document4 pagesCV By, Yvette02Yvette PamatmatNo ratings yet
- Buku AJar Infeksi Dan Pediatrik Tropis IDAIDocument31 pagesBuku AJar Infeksi Dan Pediatrik Tropis IDAIAndika SiswantaNo ratings yet
- 2023.jama - ICardíaca Con FEVI Preservada PDFDocument12 pages2023.jama - ICardíaca Con FEVI Preservada PDFEmanuelNo ratings yet
- AF Catheter AblationDocument37 pagesAF Catheter AblationSnehal JayaramNo ratings yet
- SincopaDocument73 pagesSincopacheptenev_959813483No ratings yet
- SEMINARDocument31 pagesSEMINARDeveshNo ratings yet
- A Study To Assess The Knowledge Regarding Lifestyle Modifications Among The Cardiac Patients in NMCH, Jamuhar, Sasaram, Rohtas (Bihar)Document7 pagesA Study To Assess The Knowledge Regarding Lifestyle Modifications Among The Cardiac Patients in NMCH, Jamuhar, Sasaram, Rohtas (Bihar)IJARSCT JournalNo ratings yet
- Your Circulatory System Consists of The HeartDocument4 pagesYour Circulatory System Consists of The HeartMichelle Anne OlivarNo ratings yet
- How The Human Heart Works PDFDocument2 pagesHow The Human Heart Works PDFGerard AyalaNo ratings yet
- The Prominent Dr. RombachDocument4 pagesThe Prominent Dr. Rombachtt324No ratings yet
- Winchester Cibotti Sun 2023 2023 Chronic Coronary Disease Guideline at A GlanceDocument5 pagesWinchester Cibotti Sun 2023 2023 Chronic Coronary Disease Guideline at A GlancealexafarrenNo ratings yet
- Medmastery Cardiac CT Essentials HandbookDocument61 pagesMedmastery Cardiac CT Essentials HandbookVladlena CaraimanNo ratings yet
- Cpet by Karlman Wasserman 2019Document76 pagesCpet by Karlman Wasserman 2019Wafa Naseem SheikhNo ratings yet
- Drugs Used in CPR - Lesson PlanDocument12 pagesDrugs Used in CPR - Lesson Planmonika makwana100% (2)
- TH TH: Minutes of 5 Meeting of MDB Page 1 of 14Document14 pagesTH TH: Minutes of 5 Meeting of MDB Page 1 of 14Khalid SaminaNo ratings yet
- Bab268 XLS EngDocument707 pagesBab268 XLS EngJithinmathai jacobNo ratings yet
- ACLS HandoutsDocument4 pagesACLS HandoutshasanNo ratings yet
- Perioperative Management of Patients Receiving Anticoagulants - UpToDate PDFDocument52 pagesPerioperative Management of Patients Receiving Anticoagulants - UpToDate PDFGustavo MartinezNo ratings yet
- Treatment Strategies of Acute Myocardial Infarction Updates OnDocument11 pagesTreatment Strategies of Acute Myocardial Infarction Updates OnLilasNo ratings yet
- Defibrelator ch1Document31 pagesDefibrelator ch1د.محمد عبد المنعم الشحاتNo ratings yet
- 79-Article Text-247-1-10-20220604Document10 pages79-Article Text-247-1-10-20220604Andarias MangeraNo ratings yet
- Case Study: Millie LarsenDocument11 pagesCase Study: Millie LarsenAkriti DangolNo ratings yet
- Mediclear: Site Office - 90, Vasant Complex, Mayur Vihar, DelhiDocument3 pagesMediclear: Site Office - 90, Vasant Complex, Mayur Vihar, DelhirajendradattaNo ratings yet
- Approach To Ventricular ArrhythmiasDocument18 pagesApproach To Ventricular ArrhythmiasDavid CruzNo ratings yet