You might also like
- Aerosol Generating Medical ProceduresDocument6 pagesAerosol Generating Medical Proceduresdhira anindita100% (1)
- Medication SafetyDocument68 pagesMedication SafetyPrince Jhessie L. Abella100% (9)
- The Use of Temporary Anchorage Devices For ORTHODONTIC TREATMENT of Class III Uin A Patient With An Impacred Upper CanineDocument7 pagesThe Use of Temporary Anchorage Devices For ORTHODONTIC TREATMENT of Class III Uin A Patient With An Impacred Upper CanineMargarita Lopez MartinezNo ratings yet
- ASA Staff Safety For COVID-19: StatementDocument8 pagesASA Staff Safety For COVID-19: StatementAbidi HichemNo ratings yet
- Anesthesia Management in CovidDocument4 pagesAnesthesia Management in CovidMuhammad Farooq AfzalNo ratings yet
- Checklist For Preparing Your IR Service For COVID-19Document8 pagesChecklist For Preparing Your IR Service For COVID-19uroshkgNo ratings yet
- Covid y TraqueostomíaDocument9 pagesCovid y TraqueostomíaCatalina Muñoz VelasquezNo ratings yet
- CDC AerosolDocument5 pagesCDC Aerosolwiwik sNo ratings yet
- EPP. Am. College, Surgeons.20.Document3 pagesEPP. Am. College, Surgeons.20.Mary RodriguezNo ratings yet
- Covid-19: Negative Pressure Rooms: Anmf Evidence BriefDocument5 pagesCovid-19: Negative Pressure Rooms: Anmf Evidence BriefninesuNo ratings yet
- Oral Oncology: CORONA-steps For Tracheotomy in COVID-19 Patients: A Staff-Safe Method For Airway ManagementDocument3 pagesOral Oncology: CORONA-steps For Tracheotomy in COVID-19 Patients: A Staff-Safe Method For Airway ManagementCorin Boice TelloNo ratings yet
- AO CMF COVID-19 Task Force Guidelines v1-6 PDFDocument8 pagesAO CMF COVID-19 Task Force Guidelines v1-6 PDFadhityaNo ratings yet
- Ti2020 Article WhatWeDoWhenACOVID-19PatientNe PDFDocument3 pagesTi2020 Article WhatWeDoWhenACOVID-19PatientNe PDFsiscaNo ratings yet
- Guideline For Conservation of Respiratory Protection ResourcesDocument14 pagesGuideline For Conservation of Respiratory Protection ResourcesAMEU URGENCIASNo ratings yet
- 2020 Article 1361-2Document3 pages2020 Article 1361-2Maria Alejandra AconchaNo ratings yet
- Jurnal Deskriptif IngDocument6 pagesJurnal Deskriptif IngAulin putri damayantiNo ratings yet
- It Wasn't Raining When Noah Built The ArkDocument4 pagesIt Wasn't Raining When Noah Built The ArkocramusNo ratings yet
- Perioperative Considerstions in Urgent Surgical Care of Suspected and Confirmed COVID-19 Orthopaedic PatientsDocument23 pagesPerioperative Considerstions in Urgent Surgical Care of Suspected and Confirmed COVID-19 Orthopaedic PatientsDoctor's BettaNo ratings yet
- Managing Theatre ProcessesDocument6 pagesManaging Theatre ProcessesjinoNo ratings yet
- Precautions For Operating Room Team Members During The COVID-19 PandemicDocument4 pagesPrecautions For Operating Room Team Members During The COVID-19 Pandemicjhon neiffer alberto mosquera zeaNo ratings yet
- Guidance On The Use of Personal Protective Equipment Ppe in Hospitals During The Covid 19 OutbreakDocument9 pagesGuidance On The Use of Personal Protective Equipment Ppe in Hospitals During The Covid 19 OutbreakGerlan Madrid MingoNo ratings yet
- 02a - PPE - Summary and Rationale For RecommendationsDocument2 pages02a - PPE - Summary and Rationale For RecommendationsMohammedNo ratings yet
- Tay 2020Document2 pagesTay 2020Corin Boice TelloNo ratings yet
- Tls Ep Covid 19 Ppe or Faq April27Document10 pagesTls Ep Covid 19 Ppe or Faq April27Vengky UtamiNo ratings yet
- COVID 19 Outpatient DialysisDocument5 pagesCOVID 19 Outpatient DialysisTheala RadistaNo ratings yet
- Covid 19 Airway ManagementDocument6 pagesCovid 19 Airway ManagementPablo RamirezNo ratings yet
- Guidance For Return To Practice For Otolaryngology-Head and Neck SurgeryDocument9 pagesGuidance For Return To Practice For Otolaryngology-Head and Neck SurgeryLeslie Lindsay AlvarezNo ratings yet
- Aha RCP CovidDocument3 pagesAha RCP Covidalex zuluagaNo ratings yet
- Interim Guidance For Healthcare Providers During COVID-19 OutbreakDocument3 pagesInterim Guidance For Healthcare Providers During COVID-19 OutbreakDita Ambarsari SyafruddinNo ratings yet
- Standard Operating ProcedureDocument15 pagesStandard Operating ProcedureAyman AliNo ratings yet
- Respiratory Physiotherapy Guidelines For Managing Patients With Covid or of Unknown Covid Status 15nov21 - 0Document4 pagesRespiratory Physiotherapy Guidelines For Managing Patients With Covid or of Unknown Covid Status 15nov21 - 0Gl VgNo ratings yet
- Guidelines For The Management of Tracheal Intubation in Critically Ill AdultsDocument26 pagesGuidelines For The Management of Tracheal Intubation in Critically Ill AdultsFemiko Panji AprilioNo ratings yet
- Annex 40 INTERIM GUIDELINES ON RESUSCITATION DURING COVID19 PANDEMICDocument15 pagesAnnex 40 INTERIM GUIDELINES ON RESUSCITATION DURING COVID19 PANDEMICAzran Shariman HasshimNo ratings yet
- 10 1111@anae 15054 PDFDocument33 pages10 1111@anae 15054 PDFJuliana Rodriguez MariñoNo ratings yet
- COVID Tracheostomy Guidance - CompressedDocument6 pagesCOVID Tracheostomy Guidance - CompressedMary GalvezNo ratings yet
- Covid19 Infection Prevention and ControlDocument70 pagesCovid19 Infection Prevention and ControlAdeuga ADEKUOYENo ratings yet
- A Protocol of Infection Control For Mechanical Thrombectomy in Possible COVID-19 Patients: Tokai University COVID-19 ManualDocument5 pagesA Protocol of Infection Control For Mechanical Thrombectomy in Possible COVID-19 Patients: Tokai University COVID-19 ManualMartha OktaviaNo ratings yet
- UHMS Guidelines - COVID-19 V4Document3 pagesUHMS Guidelines - COVID-19 V4Juan CruzNo ratings yet
- Insertion Mangement Peripheral IVCannulaDocument20 pagesInsertion Mangement Peripheral IVCannulaAadil AadilNo ratings yet
- Airway Mangement of Covid19Document31 pagesAirway Mangement of Covid19Shehan WijayasiriwardanaNo ratings yet
- Tracheostomy in The COVID 19 PandemicDocument3 pagesTracheostomy in The COVID 19 PandemicKenjiNo ratings yet
- Interim Guidance Pediatric Patients March 27 2020Document4 pagesInterim Guidance Pediatric Patients March 27 2020Luis Alberto Anco CórdovaNo ratings yet
- Jurnal 1Document5 pagesJurnal 1RianNo ratings yet
- Via Aerea COVID 19Document3 pagesVia Aerea COVID 19zunarodriguezleoNo ratings yet
- Approaches To The Management of Patients in Oral and Maxillofacial Surgery During COVID-19 PandemicDocument21 pagesApproaches To The Management of Patients in Oral and Maxillofacial Surgery During COVID-19 PandemicYahul MazfarNo ratings yet
- Adapting Urology Residency Training PIIS0090429520304520Document5 pagesAdapting Urology Residency Training PIIS0090429520304520Nidhin MathewNo ratings yet
- Picc Infection PDFDocument16 pagesPicc Infection PDFMahesh ChandraNo ratings yet
- Coronavirus Covid 19 Guidance On Use of Personal Protective Equipment Ppe in Non Inpatient Health Care Settings During The Covid 19 OutbreakDocument6 pagesCoronavirus Covid 19 Guidance On Use of Personal Protective Equipment Ppe in Non Inpatient Health Care Settings During The Covid 19 OutbreakGerlan Madrid MingoNo ratings yet
- COVID 19. 4 - 13 KashmerDocument42 pagesCOVID 19. 4 - 13 KashmerIshfaq GanaiNo ratings yet
- 1 s2.0 S1479666X20301888 MainDocument5 pages1 s2.0 S1479666X20301888 MainTécnicos CredineNo ratings yet
- COVID-19: A Quick Look at Aspects of Critical CareDocument5 pagesCOVID-19: A Quick Look at Aspects of Critical CareJbarrianNo ratings yet
- Recommendations For Prehospital Airway Management in Patients With Suspected COVID-19 InfectionDocument5 pagesRecommendations For Prehospital Airway Management in Patients With Suspected COVID-19 InfectionConnor StephensonNo ratings yet
- BulletinDocument16 pagesBulletindean qpNo ratings yet
- Coronavirus Disease 2019 (COVID-19) - Anesthetic Concerns, Including Airway Management and Infection ControlDocument32 pagesCoronavirus Disease 2019 (COVID-19) - Anesthetic Concerns, Including Airway Management and Infection ControlT GalenNo ratings yet
- Apexa NO 8Document5 pagesApexa NO 8Apexa YadavNo ratings yet
- Issues Related To Kidney Disease and HypertensionDocument12 pagesIssues Related To Kidney Disease and HypertensionCarlos Huaman ZevallosNo ratings yet
- Sars P&P GuidelineDocument21 pagesSars P&P Guidelineyos_peace86No ratings yet
- 2 Epitaxis Covid19Document3 pages2 Epitaxis Covid19andinNo ratings yet
- Current Problems in Diagnostic Radiology 50 (2021) 284 287Document4 pagesCurrent Problems in Diagnostic Radiology 50 (2021) 284 287Leonard AcsinteNo ratings yet
- Coronavirus RCOphth Update March 18th 1Document8 pagesCoronavirus RCOphth Update March 18th 1charoiteNo ratings yet
- Considerations For Conducting Spirometry During and After COVID19 07062020Document2 pagesConsiderations For Conducting Spirometry During and After COVID19 07062020mahdi snellNo ratings yet
- JObstetAnaesthCritCare10269-2682971 072709 PDFDocument6 pagesJObstetAnaesthCritCare10269-2682971 072709 PDFMuhammad RenaldiNo ratings yet
- Covid-19: Anaesthesia Procedures May Generate Fewer Aerosols Than Presumed, Study SuggestsDocument2 pagesCovid-19: Anaesthesia Procedures May Generate Fewer Aerosols Than Presumed, Study SuggestsMuhammad RenaldiNo ratings yet
- Extubation of Patients With COVID-19: ReferenceDocument4 pagesExtubation of Patients With COVID-19: ReferenceMuhammad RenaldiNo ratings yet
- References: Safety Considerations For Neuraxial Anaesthesia in Parturients With COVID-19Document2 pagesReferences: Safety Considerations For Neuraxial Anaesthesia in Parturients With COVID-19Muhammad RenaldiNo ratings yet
- Funding: Tracheal Intubation in COVID-19 Patients: Update On Recommendations. Response To BR J Anaesth 2020 125: E28e37Document3 pagesFunding: Tracheal Intubation in COVID-19 Patients: Update On Recommendations. Response To BR J Anaesth 2020 125: E28e37Muhammad RenaldiNo ratings yet
- MCN ReviewerDocument5 pagesMCN ReviewerShar EnriquezNo ratings yet
- BJOMSDocument2 pagesBJOMSMohammed SharifNo ratings yet
- Psychopathology Unit - 1: Abnormality and NormalityDocument37 pagesPsychopathology Unit - 1: Abnormality and NormalityNehaNo ratings yet
- Group Health & Life Insurance: Guide & ProceduresDocument27 pagesGroup Health & Life Insurance: Guide & Proceduresأحمد نوفلNo ratings yet
- MeningococcemiaDocument14 pagesMeningococcemiaMonica Marie MoralesNo ratings yet
- Awareness During AnesthesiaDocument40 pagesAwareness During Anesthesiadr_nkhan3415No ratings yet
- Data Interpretation PDF Set 9Document59 pagesData Interpretation PDF Set 9GAURAV BURMANNo ratings yet
- Employees State Insurance Act-A Hand Book of ESIC HospitalsDocument38 pagesEmployees State Insurance Act-A Hand Book of ESIC HospitalsSoundar RajNo ratings yet
- Checklist For Monitoring CHC/FRU: EmailDocument12 pagesChecklist For Monitoring CHC/FRU: EmailNational Child Health Resource Centre (NCHRC)No ratings yet
- Infant and Young Child Feeding: Key FactsDocument5 pagesInfant and Young Child Feeding: Key FactsmalentotNo ratings yet
- Resume of Neil J. GajjarDocument6 pagesResume of Neil J. GajjarNeil J. GajjarNo ratings yet
- Shigella Dysentriae: Nama Mahasiswa: Risa Shaumi Nama Skuadron: BacteriologyDocument2 pagesShigella Dysentriae: Nama Mahasiswa: Risa Shaumi Nama Skuadron: Bacteriologyreyhan fatihNo ratings yet
- Cadi PDFDocument66 pagesCadi PDFpradeepsj ReddyNo ratings yet
- Abdelkhalekabdelrazek 2021Document8 pagesAbdelkhalekabdelrazek 2021Apotik ApotekNo ratings yet
- WHO Health Workers ClassificationDocument14 pagesWHO Health Workers Classificationkotrae100% (1)
- Administering InjectionsDocument7 pagesAdministering InjectionsCyrille Aira AndresaNo ratings yet
- Importance of Pharmacists in Indian Healthcare Delivery SystemDocument5 pagesImportance of Pharmacists in Indian Healthcare Delivery SystemDebasish BhattacharjeeNo ratings yet
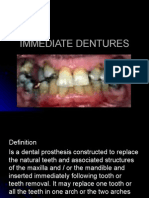
- Immediate DenturesDocument23 pagesImmediate DenturesWael FahadNo ratings yet
- Strokes, Caused by Blood ClotsDocument4 pagesStrokes, Caused by Blood Clotskata toth100% (1)
- Attitude, KnowledgeDocument7 pagesAttitude, KnowledgenabilahbilqisNo ratings yet
- Resume - Bahram MinaDocument2 pagesResume - Bahram Minamohammadrezahajian12191No ratings yet
- Case-Control Study DesignDocument60 pagesCase-Control Study DesignErmiasNo ratings yet
- Prot 001Document19 pagesProt 001patrickNo ratings yet
- Foster2018Document14 pagesFoster2018febrinaNo ratings yet
- Health Teaching PlanDocument1 pageHealth Teaching PlanRheeanne AmilasanNo ratings yet
- Newborn AssessmentDocument4 pagesNewborn AssessmentCezanne Danabelle HutallaNo ratings yet
- Autismand PDDDocument229 pagesAutismand PDDIan BrownNo ratings yet
- NKTI - NKTI Life Stories and TestimonialsDocument8 pagesNKTI - NKTI Life Stories and TestimonialsAnonymous 01pQbZUMMNo ratings yet