You might also like
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Ocular Therapeutics GuideDocument1 pageOcular Therapeutics GuideNikka ReyesNo ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- 3.02 Introduction To Medical Anthropology!: History and Perspective in MedicineDocument4 pages3.02 Introduction To Medical Anthropology!: History and Perspective in MedicineNikka ReyesNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Physician in The Pharmaceutical IndustryDocument6 pagesPhysician in The Pharmaceutical IndustryNikka ReyesNo ratings yet
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Letters To Brgy Captains SampleDocument1 pageLetters To Brgy Captains SampleNikka ReyesNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Physician As Rural PractitionerDocument3 pagesPhysician As Rural PractitionerNikka ReyesNo ratings yet
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- 2.04b Medicine in The Philippines!Document6 pages2.04b Medicine in The Philippines!Nikka ReyesNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Characterization of Oxygen CompoundsDocument4 pagesCharacterization of Oxygen CompoundsNikka ReyesNo ratings yet
- Middle Ages Architecture Highlights Early Medieval and Gothic StylesDocument28 pagesMiddle Ages Architecture Highlights Early Medieval and Gothic StylesNikka Reyes100% (1)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Physicians As Leaders and ManagersDocument3 pagesPhysicians As Leaders and ManagersNikka ReyesNo ratings yet
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Experiment 2: Vector Addition by Component, Polygon and Parallelogram MethodsDocument20 pagesExperiment 2: Vector Addition by Component, Polygon and Parallelogram MethodsNikka ReyesNo ratings yet
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Distillation of Alcoholic BeveragesDocument5 pagesDistillation of Alcoholic BeveragesNikka ReyesNo ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Hout - Energizing Strategies and ImageryDocument2 pagesHout - Energizing Strategies and ImageryNikka ReyesNo ratings yet
- Thin Layer Chromatographic Analysis of Analgesic Tablet - Group 9Document5 pagesThin Layer Chromatographic Analysis of Analgesic Tablet - Group 9Nikka Reyes100% (2)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Rizal PlayDocument1 pageRizal PlayNikka ReyesNo ratings yet
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- DB11 - Muscles of RespirationDocument3 pagesDB11 - Muscles of RespirationNikka ReyesNo ratings yet
- Extraction of Caffeine From Tea Leaves - Group 9Document5 pagesExtraction of Caffeine From Tea Leaves - Group 9Nikka ReyesNo ratings yet
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- PHYSICS - Experiment 4Document8 pagesPHYSICS - Experiment 4Nikka ReyesNo ratings yet
- PHYSICS - Experiment 1Document6 pagesPHYSICS - Experiment 1Nikka Reyes100% (1)
- PHYSICS - Experiment 2Document6 pagesPHYSICS - Experiment 2Nikka ReyesNo ratings yet
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
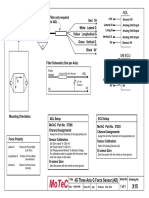
- Filter and wiring schematic for 3-axis ADL G-force sensorDocument1 pageFilter and wiring schematic for 3-axis ADL G-force sensorJuan Ramón Pérez LorenzoNo ratings yet
- Discover the training secrets of legendary bodybuildersDocument129 pagesDiscover the training secrets of legendary bodybuildersfatmir100% (7)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- TS68Document52 pagesTS68finandariefNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- DBXLH 8585B VTMDocument4 pagesDBXLH 8585B VTMmau_mmx5738No ratings yet
- Name: Sport: Movement PrepDocument24 pagesName: Sport: Movement PrepS HNo ratings yet
- Nitrogen BlanketingDocument21 pagesNitrogen Blanketingrvkumar61No ratings yet
- Ben'S Muffler RepairDocument9 pagesBen'S Muffler RepairDana LantoNo ratings yet
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Dyna Lift Flyer 500 FL 000010 enDocument20 pagesDyna Lift Flyer 500 FL 000010 enErdinc SenmanNo ratings yet
- Animal Names in English and Telugu - 20170912 - 182216545Document17 pagesAnimal Names in English and Telugu - 20170912 - 182216545karimulla goraNo ratings yet
- Planet X Restaurant Menu v2Document5 pagesPlanet X Restaurant Menu v2Chinthaka WilliamsNo ratings yet
- Jsa-0002 - CCTV Pipe Inspection RapidDocument8 pagesJsa-0002 - CCTV Pipe Inspection RapidMohamad AfifNo ratings yet
- Finasteride 5mg PDFDocument18 pagesFinasteride 5mg PDFddandan_2No ratings yet
- Subway 2009Document12 pagesSubway 2009sparklers_mNo ratings yet
- Conplast SP430Document2 pagesConplast SP430Tori Small100% (1)
- Exxonmobil High Density Polyethylene Product Guide: Extrusion MoldingDocument6 pagesExxonmobil High Density Polyethylene Product Guide: Extrusion MoldingDaikinllcNo ratings yet
- HW5e Beg CEFR Placement Test ADocument8 pagesHW5e Beg CEFR Placement Test AGabriel LemesNo ratings yet
- The Federal Environmental Protection Authority: May 2004 Addis Ababa EthiopiaDocument44 pagesThe Federal Environmental Protection Authority: May 2004 Addis Ababa Ethiopiayared0% (1)
- Barbecue Sauce HomadeDocument22 pagesBarbecue Sauce HomadeLiza NasrNo ratings yet
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Basic Science JSS 1 2NDDocument29 pagesBasic Science JSS 1 2NDAdeoye Olufunke100% (2)
- Dissertation - December 2022Document71 pagesDissertation - December 2022Musasa TinasheNo ratings yet
- Form Ibpr Haul Road PDFDocument2 pagesForm Ibpr Haul Road PDFelvandi100% (1)
- Facilitating Civic Engagement Through Consultation: Learning From Local Communities Through The NHI-Accountability Project in South AfricaDocument64 pagesFacilitating Civic Engagement Through Consultation: Learning From Local Communities Through The NHI-Accountability Project in South AfricaOxfamNo ratings yet
- Work Immersion PortfolioDocument15 pagesWork Immersion PortfolioKaye Irish RosauroNo ratings yet
- 4-Ingredient Vegan Easy Brownies - Minimalist Baker RecipesDocument2 pages4-Ingredient Vegan Easy Brownies - Minimalist Baker RecipespeteNo ratings yet
- Designing Resistance Training Programmes To Enhance Muscular Fitness A Review of The Acute Programme VariablesDocument12 pagesDesigning Resistance Training Programmes To Enhance Muscular Fitness A Review of The Acute Programme VariablesSheilani MartinsNo ratings yet
- Home ScienceDocument29 pagesHome ScienceAhmad Muneer ChadkutNo ratings yet
- Cochlear ImplantsDocument53 pagesCochlear ImplantsSovitJungBaralNo ratings yet
- WP Stratasys TopFiveReasonsDocument7 pagesWP Stratasys TopFiveReasonscititorulturmentatNo ratings yet
- Maximize muscle gains with reverse pyramid trainingDocument8 pagesMaximize muscle gains with reverse pyramid trainingMusadiq Ahmed100% (1)
- Animals Pets Board GameDocument1 pageAnimals Pets Board GameOlga ZasNo ratings yet
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (402)
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (17)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsFrom EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo ratings yet