You might also like
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Acute MastoiditisDocument15 pagesAcute MastoiditisSul FadlyNo ratings yet
- Sertifikat Utbk LTMPT 321712070700Document1 pageSertifikat Utbk LTMPT 321712070700Sul FadlyNo ratings yet
- Jsafog 9 323 PDFDocument4 pagesJsafog 9 323 PDFSul FadlyNo ratings yet
- Sul Fadly, S.Ked: Certificate of CompletionDocument1 pageSul Fadly, S.Ked: Certificate of CompletionSul FadlyNo ratings yet
- Management of Eyelid Lacerations: CornerDocument6 pagesManagement of Eyelid Lacerations: CornerSul FadlyNo ratings yet
- Ase Report: Anesthetic Management of A Case of Umbilical Cord ProlapseDocument3 pagesAse Report: Anesthetic Management of A Case of Umbilical Cord ProlapseSul FadlyNo ratings yet
- F1901132530 PDFDocument6 pagesF1901132530 PDFSul FadlyNo ratings yet
- Efektivitas Vaksin VaricellaDocument21 pagesEfektivitas Vaksin VaricellaSul FadlyNo ratings yet
- The Description of Factors That Influence The Level of Mother's Knowledge Regarding Basic Immunization of InfantsDocument12 pagesThe Description of Factors That Influence The Level of Mother's Knowledge Regarding Basic Immunization of InfantsSul FadlyNo ratings yet
- Hydralazine Vs Nifedipine For Acute Hypertensive Emergency in Pregnancy: A Randomized Controlled TrialDocument6 pagesHydralazine Vs Nifedipine For Acute Hypertensive Emergency in Pregnancy: A Randomized Controlled TrialSul FadlyNo ratings yet
- Long-Term Memory in Amnesia: Cued Recall, Recognition Memory, and Confidence RatingsDocument8 pagesLong-Term Memory in Amnesia: Cued Recall, Recognition Memory, and Confidence RatingsSul FadlyNo ratings yet
- Rapamycin Treatment Benefits Glucose Metabolism in Mouse Models of Type 2 DiabetesDocument11 pagesRapamycin Treatment Benefits Glucose Metabolism in Mouse Models of Type 2 DiabetesSul FadlyNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Preterm LaborDocument17 pagesPreterm LaborInd Matthew100% (1)
- Exposé Sur Le SIDA en AnglaisDocument5 pagesExposé Sur Le SIDA en AnglaisBarro SoloNo ratings yet
- PatographDocument2 pagesPatographEvans Rogers NkanzaNo ratings yet
- Dewi Puspa Ratna Sari - 1308150 - Nonfull PDFDocument33 pagesDewi Puspa Ratna Sari - 1308150 - Nonfull PDFwahyuni yuniNo ratings yet
- Ncidence and Risk Factors of Bacterial Vaginosis AmongDocument9 pagesNcidence and Risk Factors of Bacterial Vaginosis AmongradenbagasNo ratings yet
- Jurnal Internasional PDFDocument8 pagesJurnal Internasional PDFMahasiswa PEBRIANINo ratings yet
- Care of Mother and Child (Well-Client)Document67 pagesCare of Mother and Child (Well-Client)Jake Padua100% (2)
- Environmental TeratogensDocument14 pagesEnvironmental TeratogensAbdul bariNo ratings yet
- Maternal Health Nursing SkillsDocument279 pagesMaternal Health Nursing SkillsSharm ManlangitNo ratings yet
- Procedure Assignment For ManagementDocument7 pagesProcedure Assignment For ManagementPatel Amee100% (1)
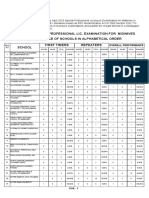
- April 2023 Special Professional Lic. Examination For MidwivesDocument2 pagesApril 2023 Special Professional Lic. Examination For MidwivesRapplerNo ratings yet
- Faal Partus: Naifah Luthfiyah Putri 15-009Document58 pagesFaal Partus: Naifah Luthfiyah Putri 15-009NaifahLuthfiyahPutriNo ratings yet
- Sexual Reproduction PDFDocument4 pagesSexual Reproduction PDFPerry SinNo ratings yet
- Men, Desire Women But Do Not Need Them. Women, Both Desire Men and Need Them.Document3 pagesMen, Desire Women But Do Not Need Them. Women, Both Desire Men and Need Them.Jamiah HulipasNo ratings yet
- Your Family Tree: In-LawsDocument4 pagesYour Family Tree: In-LawszorzicaNo ratings yet
- Ginecologie An.v EngDocument67 pagesGinecologie An.v EngAhmad Abu KushNo ratings yet
- Fundal Height DefinedDocument2 pagesFundal Height Definedervin0122No ratings yet
- THBT Woman Older Than 40 Should Not Have ChildrenDocument2 pagesTHBT Woman Older Than 40 Should Not Have ChildrenElma Nur HafizahNo ratings yet
- Jharkhand ReportDocument133 pagesJharkhand ReportNutan TiggaNo ratings yet
- Married 1271-1280Document21 pagesMarried 1271-1280a10navazpNo ratings yet
- The Pros and Cons of Legalizing ProstitutionDocument3 pagesThe Pros and Cons of Legalizing ProstitutionVincentAysonNo ratings yet
- Discussion TextDocument6 pagesDiscussion TextIndri FitrialstiNo ratings yet
- History What Is STI? BackgroundDocument4 pagesHistory What Is STI? BackgroundAko Si LibroNo ratings yet
- What Makes People Gay?Document9 pagesWhat Makes People Gay?Anthony McCartneyNo ratings yet
- Non Stress TestDocument5 pagesNon Stress TestPadma100% (1)
- Picot AnalysisDocument4 pagesPicot AnalysisLittle StarNo ratings yet
- Ethics Moral DevelopmentDocument2 pagesEthics Moral DevelopmentJanna Rose HusmilloNo ratings yet
- Human Reproduction PDFDocument35 pagesHuman Reproduction PDFsqhaa100% (4)
- Care of Mother, Child, Adolescent: NCM 207 / MCN / PrelimsDocument17 pagesCare of Mother, Child, Adolescent: NCM 207 / MCN / PrelimsCharlie AbagonNo ratings yet
- KIK KI-1 PREGNANCY RELATED DEATH NOTIFICATION FORM Revised 2020Document1 pageKIK KI-1 PREGNANCY RELATED DEATH NOTIFICATION FORM Revised 2020syamimi amalinaNo ratings yet