You might also like
- All Ceramic Inlays and Onlays For Posterior TeethDocument11 pagesAll Ceramic Inlays and Onlays For Posterior TeethNajeeb Ullah100% (1)
- Fixed Prosthodontics in Dental PracticeFrom EverandFixed Prosthodontics in Dental PracticeRating: 4 out of 5 stars4/5 (1)
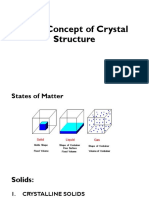
- Basic Concepts of Crystal StructureDocument46 pagesBasic Concepts of Crystal StructureHannah TaeHun60% (5)
- Ceramic Inlays A Case Presentation and LessonsDocument11 pagesCeramic Inlays A Case Presentation and LessonsStef David100% (1)
- Adhesive Restoration of Endodontically Treated TeethFrom EverandAdhesive Restoration of Endodontically Treated TeethRating: 3 out of 5 stars3/5 (2)
- Ceramic Defects TableDocument23 pagesCeramic Defects TableMohammad Youssefi87% (15)
- Fake Silk - The Lethal History of Viscose Rayon-Yale University Press (2016)Document263 pagesFake Silk - The Lethal History of Viscose Rayon-Yale University Press (2016)Juan CubasNo ratings yet
- Class Aand BabcDocument8 pagesClass Aand Babcal sigmanovaNo ratings yet
- Almeida. All-Ceramic Crowns and Extended Veneers in Anterior Dentition PDFDocument23 pagesAlmeida. All-Ceramic Crowns and Extended Veneers in Anterior Dentition PDFChelsea GarcíaNo ratings yet
- Consideraciones InlayDocument12 pagesConsideraciones InlayMarisha CastroNo ratings yet
- Clinical Case Reports - 2023 - Karimi - Veneer Crowns in Anterior Endodontically Treated Teeth A Case Report With 1 YearDocument8 pagesClinical Case Reports - 2023 - Karimi - Veneer Crowns in Anterior Endodontically Treated Teeth A Case Report With 1 YearOgie WijayantoNo ratings yet
- OVERLAYDocument24 pagesOVERLAYJose Luis Celis100% (3)
- Bonding To Atypical Tooth SurfacesDocument4 pagesBonding To Atypical Tooth SurfacesRomit SenNo ratings yet
- Case Report 2: Feldspathic Veneers: What Are Their Indications?Document6 pagesCase Report 2: Feldspathic Veneers: What Are Their Indications?Nol H. CenaNo ratings yet
- A New Design For Anterior Porcelain Fused To Metal Fixed Prosthetic Restorations PTU Type IIIDocument4 pagesA New Design For Anterior Porcelain Fused To Metal Fixed Prosthetic Restorations PTU Type IIIElian HomsiehNo ratings yet
- All-Ceramic Crowns and Extended Veneers in Anterior Dentition - A Case Report With Critical Discussion.Document23 pagesAll-Ceramic Crowns and Extended Veneers in Anterior Dentition - A Case Report With Critical Discussion.Andrei ConstantinoviciNo ratings yet
- Ultrathin Monolithic Zirconia Veneers: Reality or Future? Report of A Clinical Case and One-Year Follow-UpDocument9 pagesUltrathin Monolithic Zirconia Veneers: Reality or Future? Report of A Clinical Case and One-Year Follow-UpYovana Carolina Corimanya MoranNo ratings yet
- Minimumthickness Anteriorporcelain Restorations: Gary M. RadzDocument18 pagesMinimumthickness Anteriorporcelain Restorations: Gary M. RadzElize MachadoNo ratings yet
- Ceramics As Biomaterials For Dental RestorationDocument17 pagesCeramics As Biomaterials For Dental RestorationCatalina GómezNo ratings yet
- Esthetic Rehabilitation of Anterior Dentition WithDocument6 pagesEsthetic Rehabilitation of Anterior Dentition WithHugoo AmayaaNo ratings yet
- Comp v31n9 Rev Op 2ndDocument7 pagesComp v31n9 Rev Op 2ndsaladinhieroNo ratings yet
- All Ceramic Cementation A Key To Successful RestorationDocument9 pagesAll Ceramic Cementation A Key To Successful RestorationJUDITH ESTHER HIGUERA MESANo ratings yet
- Step-by-Step Ultraconservative Esthetic Rehabilitation Using LithiumDocument19 pagesStep-by-Step Ultraconservative Esthetic Rehabilitation Using LithiumAlfred OrozcoNo ratings yet
- Vonlays: A Conservative Esthetic Alternative To Full-Coverage CrownsDocument6 pagesVonlays: A Conservative Esthetic Alternative To Full-Coverage CrownsDavid Gomez0% (1)
- Vonlays 2015 3Document7 pagesVonlays 2015 3Patrick Castillo SalazarNo ratings yet
- 1 s2.0 S0022391310601114 Main PDFDocument9 pages1 s2.0 S0022391310601114 Main PDFPatty ChuNo ratings yet
- Coronas y Otras Restauraciones ExtracoronalesDocument10 pagesCoronas y Otras Restauraciones Extracoronalesjuan929No ratings yet
- Fiber-Reinforced Onlay Composite (Unlocked by WWW - Freemypdf.com)Document7 pagesFiber-Reinforced Onlay Composite (Unlocked by WWW - Freemypdf.com)Adrian DjohanNo ratings yet
- Minimally Invasive Vertical Preparation Design For Ceramic VeneersDocument12 pagesMinimally Invasive Vertical Preparation Design For Ceramic VeneersdanielaNo ratings yet
- Carillas de Porcelana - Nitesh Shetty - Savita Dandakeri - Shilpa DandekeriDocument5 pagesCarillas de Porcelana - Nitesh Shetty - Savita Dandakeri - Shilpa DandekeriJony OcañaNo ratings yet
- 1920-Article Text-4050-1-10-20191127Document5 pages1920-Article Text-4050-1-10-20191127CristinaNo ratings yet
- Am JEsthet Dent 2011 Almeidae Silva JSDocument23 pagesAm JEsthet Dent 2011 Almeidae Silva JSRuxandra FitaNo ratings yet
- Modern Adhesive Ceramic Onlay PDFDocument6 pagesModern Adhesive Ceramic Onlay PDFAl Azizul HakimNo ratings yet
- Inlay and Onlay PDFDocument13 pagesInlay and Onlay PDFrahmaNo ratings yet
- No31 Comparing Porcelain-fused-To-metal Versus Zirconium-Based RestorationsDocument4 pagesNo31 Comparing Porcelain-fused-To-metal Versus Zirconium-Based RestorationsIbrahim MohamedNo ratings yet
- Ultimate Ceramic Veneers: A Laboratory-Guided Preparation Technique For Minimally Invasive RestorationsDocument17 pagesUltimate Ceramic Veneers: A Laboratory-Guided Preparation Technique For Minimally Invasive RestorationsPablo BenitezNo ratings yet
- Ultimate Ceramic Veneers: A Laboratory-Guided Preparation Technique For Minimally Invasive RestorationsDocument17 pagesUltimate Ceramic Veneers: A Laboratory-Guided Preparation Technique For Minimally Invasive RestorationsAlfred OrozcoNo ratings yet
- 10) Galiatsatos AristidisDocument4 pages10) Galiatsatos AristidismnNo ratings yet
- Reproduci NG Opt I Cal Propert Ies of An T Eriorteeth After Ultra - Conservative PreparationDocument10 pagesReproduci NG Opt I Cal Propert Ies of An T Eriorteeth After Ultra - Conservative PreparationCaio BalbinotNo ratings yet
- CeramicsDocument3 pagesCeramicsFaizah Ayulia NawitaNo ratings yet
- The Carolina Bridge: A Novel Interim All-Porcelain Bonded ProsthesisDocument12 pagesThe Carolina Bridge: A Novel Interim All-Porcelain Bonded ProsthesissalmaNo ratings yet
- Ultimate Ceramic Veneer A Laboratory-Gui PDFDocument16 pagesUltimate Ceramic Veneer A Laboratory-Gui PDFHector Flores SotoNo ratings yet
- EPR2Document7 pagesEPR2RazvanAngheleNo ratings yet
- Ferraris Et Al IJED PIAR ARG 2 20212Document24 pagesFerraris Et Al IJED PIAR ARG 2 20212khaled emadNo ratings yet
- The Endocrown: An Alternative Approach For Restoring Extensively Damaged MolarsDocument8 pagesThe Endocrown: An Alternative Approach For Restoring Extensively Damaged MolarsHoàng Đình PhúcNo ratings yet
- Ceramic Laminates in Conoid Teeth: An Integrative Literature ReviewDocument8 pagesCeramic Laminates in Conoid Teeth: An Integrative Literature ReviewIJAERS JOURNALNo ratings yet
- Modern Dental Ceramics An OverviewDocument6 pagesModern Dental Ceramics An OverviewDilesh PradhanNo ratings yet
- Chapter 5 Fundamental Concepts of Enamel andDocument24 pagesChapter 5 Fundamental Concepts of Enamel andJerome Tolentino TotingNo ratings yet
- Dental Ceramics For Restoration and Metal VeneeringDocument23 pagesDental Ceramics For Restoration and Metal VeneeringMichael XuNo ratings yet
- Articol Pu EnglDocument6 pagesArticol Pu EnglAntonela CeremușNo ratings yet
- CrownsDocument4 pagesCrownsNindy MsNo ratings yet
- Endocrown (DR - Roja)Document5 pagesEndocrown (DR - Roja)Shubham KingraNo ratings yet
- 15 Restorative MaterialsDocument9 pages15 Restorative MaterialsJohn CenaNo ratings yet
- Direct Posterior Composite 1Document33 pagesDirect Posterior Composite 1Rawzh Salih MuhammadNo ratings yet
- Fiber-Reinforced Composite in Dentistry - A ReviewDocument5 pagesFiber-Reinforced Composite in Dentistry - A ReviewLucianoNo ratings yet
- Crown in Paedatric DentistryDocument6 pagesCrown in Paedatric DentistrySTEFFI MIFTANo ratings yet
- Esthetic Rehabilitation of The Smile With No-Prep Porcelain Laminates and Partial Veneers PDFDocument7 pagesEsthetic Rehabilitation of The Smile With No-Prep Porcelain Laminates and Partial Veneers PDFSAMUELNo ratings yet
- Case Report: Esthetic Rehabilitation of The Smile With No-Prep Porcelain Laminates and Partial VeneersDocument6 pagesCase Report: Esthetic Rehabilitation of The Smile With No-Prep Porcelain Laminates and Partial VeneersMona CameliaNo ratings yet
- Crowns For Paediatric Teeth Stainless Steel CrownDocument6 pagesCrowns For Paediatric Teeth Stainless Steel CrownFisa AhrNo ratings yet
- A Prospective Evaluation of Zirconia Anterior Partial Fixed Dental Prostheses: Clinical Results After Seven YearsDocument7 pagesA Prospective Evaluation of Zirconia Anterior Partial Fixed Dental Prostheses: Clinical Results After Seven YearsBianca DimofteNo ratings yet
- Using Modi Fied Polyetheretherketone (PEEK) As An Alternative Material For Endocrown Restorations: A Short-Term Clinical ReportDocument5 pagesUsing Modi Fied Polyetheretherketone (PEEK) As An Alternative Material For Endocrown Restorations: A Short-Term Clinical ReportRohiniNo ratings yet
- Using Modified Polyetheretherketone (PEEK) As An Alternative Material For Endocrown Restorations - A Short-Term Clinical ReportDocument5 pagesUsing Modified Polyetheretherketone (PEEK) As An Alternative Material For Endocrown Restorations - A Short-Term Clinical Reportdody rahman100% (1)
- Survival of Resin-Bonded Porcelain Veneer Crowns Placed With and Without Metal ReinforcementDocument7 pagesSurvival of Resin-Bonded Porcelain Veneer Crowns Placed With and Without Metal ReinforcementDr Sai Govind GavaraNo ratings yet
- 1 s2.0 S0300571220300889 Main PDFDocument11 pages1 s2.0 S0300571220300889 Main PDFpablogdv956No ratings yet
- Guidelines For Occlusion Strategy in Imp PDFDocument7 pagesGuidelines For Occlusion Strategy in Imp PDFpablogdv956No ratings yet
- And The Tooth CrackedDocument20 pagesAnd The Tooth Crackedpablogdv956No ratings yet
- Reviewing The Concept of Dahl: S S A J. SDocument5 pagesReviewing The Concept of Dahl: S S A J. Spablogdv956No ratings yet
- Combining Traditional and Adhesive Dentistry To Reconstruct The Excessively Worn DentitionDocument21 pagesCombining Traditional and Adhesive Dentistry To Reconstruct The Excessively Worn Dentitionpablogdv956No ratings yet
- Strategies To Stabilise Dentine-Bonded Interfaces Through RemineralizingDocument19 pagesStrategies To Stabilise Dentine-Bonded Interfaces Through Remineralizingpablogdv956No ratings yet
- Rehabilitación de Hexágono ExternoDocument13 pagesRehabilitación de Hexágono Externopablogdv956No ratings yet
- Aesthetic Clasp Design For Removable Partial Dentures A Litewrature ReviewDocument5 pagesAesthetic Clasp Design For Removable Partial Dentures A Litewrature Reviewpablogdv956100% (1)
- Copyofapchemistrytakehometest 2Document7 pagesCopyofapchemistrytakehometest 2api-311739848No ratings yet
- Cleavage of MineralsDocument3 pagesCleavage of MineralsAlexandru StefanNo ratings yet
- Burtrand Lee, Sridhar Komarneni - 2005 - Chemical Processing of CeramicsDocument737 pagesBurtrand Lee, Sridhar Komarneni - 2005 - Chemical Processing of Ceramicsvanessa santanaNo ratings yet
- Histopath ReviewDocument389 pagesHistopath ReviewLucille MarieNo ratings yet
- Astm B242Document4 pagesAstm B242kashif ehsanNo ratings yet
- Assignment 1Document2 pagesAssignment 1Tony TroxNo ratings yet
- How Is Plastic Made A Simple Step-By-Step ExplanationDocument12 pagesHow Is Plastic Made A Simple Step-By-Step Explanationsalemg82No ratings yet
- Use of Partial Dissolution Techniques in Geochemical ExplorationDocument35 pagesUse of Partial Dissolution Techniques in Geochemical ExplorationMiguel Angel Catunta ZarateNo ratings yet
- 70-112 Gypsum Plaster Over ConcreteDocument2 pages70-112 Gypsum Plaster Over ConcretejcdaouNo ratings yet
- Incozol 2 DataDocument2 pagesIncozol 2 DataJeffrey Bempong100% (1)
- Sample Solution: PROBLEM 4.20Document8 pagesSample Solution: PROBLEM 4.20Nacho Araneda0% (1)
- LUBRICANTSDocument10 pagesLUBRICANTSRevanth PolicherlaNo ratings yet
- 2019 JC2 PE H2 Chemistry Paper 4 (Solutions - Comments For Students)Document23 pages2019 JC2 PE H2 Chemistry Paper 4 (Solutions - Comments For Students)Arthur SoonNo ratings yet
- Chemical Bonding Reading MaterialDocument6 pagesChemical Bonding Reading MaterialJohann Carlo C. AldecoaNo ratings yet
- Fiber Selectionforthe Productionof NonwovensDocument33 pagesFiber Selectionforthe Productionof NonwovensTimothy PonrathnamNo ratings yet
- Potassium AlumDocument5 pagesPotassium Alumneville almeidaNo ratings yet
- Journal of Chemical Engineering DataDocument5 pagesJournal of Chemical Engineering Dataedor29No ratings yet
- Rubber IndustryDocument9 pagesRubber IndustryifounditNo ratings yet
- Baking PowderDocument6 pagesBaking PowderHema HemaNo ratings yet
- Topic 14.0: Haloalkanes (Alkyl Halides)Document12 pagesTopic 14.0: Haloalkanes (Alkyl Halides)Supia NazmaNo ratings yet
- Filament Winding: Serkan CUBUK E6704Document17 pagesFilament Winding: Serkan CUBUK E6704Charaf Leo100% (1)
- S-Block Elments: Inorganic ChemistryDocument8 pagesS-Block Elments: Inorganic ChemistryRSLNo ratings yet
- Basic Concepts of Organic ChemistryDocument112 pagesBasic Concepts of Organic ChemistryNavya KuchanaNo ratings yet
- Investigating The Role of Irradiation Defects During UO Oxidative DissolutionDocument21 pagesInvestigating The Role of Irradiation Defects During UO Oxidative DissolutionriteshmohunNo ratings yet
- Lab Report 11 Electrochemical CellsDocument5 pagesLab Report 11 Electrochemical CellsAdlin Lina0% (1)
- Acetic AcidDocument19 pagesAcetic AcidEmre KOÇNo ratings yet