You might also like
- Book Partituras - Richard Clayderman 3 - Piano Solo Best Collection PDFDocument49 pagesBook Partituras - Richard Clayderman 3 - Piano Solo Best Collection PDFMadirley Pimenta100% (1)
- Isometrics Mass ManualDocument41 pagesIsometrics Mass Manualassssssssss100% (6)
- The Secrets of Fulvic AcidDocument3 pagesThe Secrets of Fulvic Acidatpfacebook100% (3)
- Stop Anticoagulation Neuraxial AnesthesiaDocument3 pagesStop Anticoagulation Neuraxial AnesthesiaGihan NakhlehNo ratings yet
- Spirit Release TherapyDocument12 pagesSpirit Release Therapyravik38100% (6)
- Chapter 4 - Presentation Analysis InterpretationDocument45 pagesChapter 4 - Presentation Analysis InterpretationDiana MuañaNo ratings yet
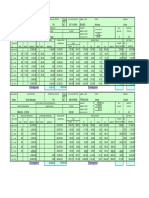
- Payroll Project PDFDocument39 pagesPayroll Project PDFUsmän Mïrżä100% (2)
- Practical Research 2 PDFDocument60 pagesPractical Research 2 PDFSargeant Oxford100% (1)
- Measuring OutcomesDocument58 pagesMeasuring OutcomesEbony2514100% (1)
- Critique of the CAM-ICU Delirium Assessment ToolDocument8 pagesCritique of the CAM-ICU Delirium Assessment Toolwaliworld100% (1)
- Oropharyngeal and Tongue Exercises (Myofunctional Therapy) For Snoring: A Systematic Review and Meta-AnalysisDocument7 pagesOropharyngeal and Tongue Exercises (Myofunctional Therapy) For Snoring: A Systematic Review and Meta-AnalysissirahNo ratings yet
- Evaluation of Emotional Excitation During Standardized Endotracheal Intubation in Simulated Conditionsannals of Intensive CareDocument8 pagesEvaluation of Emotional Excitation During Standardized Endotracheal Intubation in Simulated Conditionsannals of Intensive CareRoberto SanchezNo ratings yet
- Original Research: Intensive Care Unit Structure Variation and Implications For Early Mobilization PracticesDocument12 pagesOriginal Research: Intensive Care Unit Structure Variation and Implications For Early Mobilization Practicesandi kurniawanNo ratings yet
- Sedation in The Intensive Care Unit A Systematic RDocument13 pagesSedation in The Intensive Care Unit A Systematic RFebri Yudha Adhi KurniawanNo ratings yet
- Sedación ProtocolizadaDocument11 pagesSedación ProtocolizadaAlejandra LópezNo ratings yet
- Assessment and Management of Preoperative AnxietyDocument6 pagesAssessment and Management of Preoperative AnxietyFiorel Loves EveryoneNo ratings yet
- Epilepsy Duration and Seizure Outcome in Epilepsy Surgery: A Systematic Review and Meta-AnalysisDocument9 pagesEpilepsy Duration and Seizure Outcome in Epilepsy Surgery: A Systematic Review and Meta-Analysisbaba ababNo ratings yet
- Best Practices For Elderly Hip Fracture Patients. A Systematic Overview of The Evidence.Document7 pagesBest Practices For Elderly Hip Fracture Patients. A Systematic Overview of The Evidence.Tuấn Lê (jose)No ratings yet
- Jadad 1995Document4 pagesJadad 1995iglesiasowenNo ratings yet
- Assessment and Management of Preoperative Anxiety: London, United KingdomDocument6 pagesAssessment and Management of Preoperative Anxiety: London, United KingdomrsudabadiNo ratings yet
- ncc2021 1Document10 pagesncc2021 1api-519486875No ratings yet
- D3kepma2a - Putri Winda Nathaniella - P17210183047Document13 pagesD3kepma2a - Putri Winda Nathaniella - P17210183047mufid dodyNo ratings yet
- cc697 PDFDocument9 pagescc697 PDFGilbertLiemNo ratings yet
- D3kepma2a - Putri Winda Nathaniella - P17210183047Document13 pagesD3kepma2a - Putri Winda Nathaniella - P17210183047mufid dodyNo ratings yet
- Physical Restraint Use in Adult Patients Presenting To A General Emergency DepartmentDocument10 pagesPhysical Restraint Use in Adult Patients Presenting To A General Emergency DepartmentBeatrizNo ratings yet
- Research ArticleDocument10 pagesResearch Articlerazaqhussain00No ratings yet
- The Pediatric Sedation Unit: A Mechanism For Pediatric SedationDocument9 pagesThe Pediatric Sedation Unit: A Mechanism For Pediatric SedationSantosa TandiNo ratings yet
- Early Sedation With Dexmedetomidine in Critically Ill PatientsDocument14 pagesEarly Sedation With Dexmedetomidine in Critically Ill PatientsPutra SetiawanNo ratings yet
- Review Article: Efficacy of Acupuncture in Reducing Preoperative Anxiety: A Meta-AnalysisDocument13 pagesReview Article: Efficacy of Acupuncture in Reducing Preoperative Anxiety: A Meta-AnalysisDyan TonyNo ratings yet
- Copia de 09enero Sedacion Prot Vs No ProtDocument22 pagesCopia de 09enero Sedacion Prot Vs No ProtMartin LafuenteNo ratings yet
- Defining A High-Performance lCU System For The - , 21st Century: A Position PaperDocument11 pagesDefining A High-Performance lCU System For The - , 21st Century: A Position PaperRodrigoSachiFreitasNo ratings yet
- JeradDocument10 pagesJeradzaimmuhtarNo ratings yet
- 1 - Outcomes ResearchDocument12 pages1 - Outcomes ResearchMauricio Ruiz MoralesNo ratings yet
- Safety of Robotic Thyroidectomy Approaches: Meta-Analysis and Systematic ReviewDocument7 pagesSafety of Robotic Thyroidectomy Approaches: Meta-Analysis and Systematic Reviewcabeza y cuello incNo ratings yet
- Enteral1 PDFDocument10 pagesEnteral1 PDFCarlos Eduardo FerrazNo ratings yet
- SedationDocument7 pagesSedationAurora Violeta Zapata RuedaNo ratings yet
- Study of Ideal Topical Pharyngeal Anesthesia in UpDocument6 pagesStudy of Ideal Topical Pharyngeal Anesthesia in UpRegina SantosoNo ratings yet
- Fan Therapy For The Treatment of Dyspnea in Adult, Sistematic ReviewDocument6 pagesFan Therapy For The Treatment of Dyspnea in Adult, Sistematic ReviewSaputra IanNo ratings yet
- 2014 - Effectiveness of Implementing A Wake Up and Breathe ProgramDocument10 pages2014 - Effectiveness of Implementing A Wake Up and Breathe ProgramgiseladlrNo ratings yet
- Esicm 2020Document612 pagesEsicm 2020FERNANDODEJESUS LOPEZ RUEDANo ratings yet
- Assesment of Patients's Self Perceived Intensive Care Unit DiscomfortDocument9 pagesAssesment of Patients's Self Perceived Intensive Care Unit Discomfortrisa setiaNo ratings yet
- Protocolos Weaining 2011Document14 pagesProtocolos Weaining 2011perla islasNo ratings yet
- Penggunaan Sedasi Pada Anak Dengan VentilatorDocument5 pagesPenggunaan Sedasi Pada Anak Dengan VentilatorCalvin AffendyNo ratings yet
- N375 Literature Tables, Guideline and Grading RubricDocument7 pagesN375 Literature Tables, Guideline and Grading RubricfaizaNo ratings yet
- Reducing Anxiety and Pain with Guided ImageryDocument7 pagesReducing Anxiety and Pain with Guided ImageryKevin Miguel RiveraNo ratings yet
- Pain Assessment Tools For Older Adults With Dementia in Long-Term Care Facilities: A Systematic ReviewDocument14 pagesPain Assessment Tools For Older Adults With Dementia in Long-Term Care Facilities: A Systematic Review12099964No ratings yet
- Patient-Initiated Device Removal in Intensive Care Units - A National Prevalence StudyDocument7 pagesPatient-Initiated Device Removal in Intensive Care Units - A National Prevalence StudyJim LinNo ratings yet
- ICU vs. Ward PU PreventionDocument59 pagesICU vs. Ward PU PreventionrantiNo ratings yet
- Af 75Document13 pagesAf 75Ola ZahraNo ratings yet
- What Are The Patterns of Compliance Whith Early Warning TrackDocument9 pagesWhat Are The Patterns of Compliance Whith Early Warning TrackPAULA SORAIA CHENNo ratings yet
- Strategies of Decresing Anxiety in The Perioperative SettingsDocument16 pagesStrategies of Decresing Anxiety in The Perioperative SettingsFiorel Loves EveryoneNo ratings yet
- Intensive & Critical Care Nursing: Research ArticleDocument7 pagesIntensive & Critical Care Nursing: Research ArticleEviNo ratings yet
- Patient Centred Variables With Univariateassociations With Unplanned ICU Admissiona Systematic ReviewDocument9 pagesPatient Centred Variables With Univariateassociations With Unplanned ICU Admissiona Systematic ReviewsarintiNo ratings yet
- Indicadores Calidad en AnestesiaDocument18 pagesIndicadores Calidad en AnestesiaMijael Vega AcuñaNo ratings yet
- Indicadores Calidad en AnestesiaDocument18 pagesIndicadores Calidad en AnestesiaMijael Vega AcuñaNo ratings yet
- 7402 Ensuring Patient Safety in Emergency Peripheral Ultrasound Guided Nerve Blocks An Evaluation of A Quality Improvement Patient Safety InitiativeDocument7 pages7402 Ensuring Patient Safety in Emergency Peripheral Ultrasound Guided Nerve Blocks An Evaluation of A Quality Improvement Patient Safety Initiativemouxritsa_83No ratings yet
- Extubacion en NeurocriticoDocument3 pagesExtubacion en NeurocriticoJuan Soto FarfanNo ratings yet
- Lam Et Al. (2020)Document13 pagesLam Et Al. (2020)VINICIUS CAMARGO KISSNo ratings yet
- Telephone Validation of The Quality of Life in Epilepsy Inventory 89 (QOLIE 89)Document10 pagesTelephone Validation of The Quality of Life in Epilepsy Inventory 89 (QOLIE 89)David DeegbeNo ratings yet
- 1997-01 Stressors Revised - BDocument26 pages1997-01 Stressors Revised - BineNo ratings yet
- Simple Four-Variable Screening Tool For Identification of Patients With Sleep-Disordered BreathingDocument10 pagesSimple Four-Variable Screening Tool For Identification of Patients With Sleep-Disordered BreathingAuxiliares NeurofisiologíaNo ratings yet
- J Ijnurstu 2017 12 012Document8 pagesJ Ijnurstu 2017 12 012Osborn KhasabuliNo ratings yet
- Dyspnea ProjectDocument20 pagesDyspnea Projectfarah.abd97No ratings yet
- Development of A Modified Swallowing Screening TooDocument7 pagesDevelopment of A Modified Swallowing Screening TooNADISH MANZOORNo ratings yet
- 2019 Jurnal 4Document8 pages2019 Jurnal 4noviyantieliskaNo ratings yet
- Measuring A Caring Culture in Hospitals: A Systematic Review of InstrumentsDocument10 pagesMeasuring A Caring Culture in Hospitals: A Systematic Review of InstrumentsWinataria YantiNo ratings yet
- A Systematic Review and Meta-Analysis of Risk 2022Document10 pagesA Systematic Review and Meta-Analysis of Risk 2022Claudia Mei Lan JaeNo ratings yet
- Clinical Guideline Diagnosing Syncope Part 1: Value of History, Physical Examination, and ElectrocardiographyDocument8 pagesClinical Guideline Diagnosing Syncope Part 1: Value of History, Physical Examination, and ElectrocardiographyPriya JainNo ratings yet
- BIS-Guided Propofol vs Etomidate Induction: Hypotension and Hypertension RiskDocument9 pagesBIS-Guided Propofol vs Etomidate Induction: Hypotension and Hypertension RiskGihan NakhlehNo ratings yet
- Anesthesiology 2011 115 1209 1218Document10 pagesAnesthesiology 2011 115 1209 1218Gihan NakhlehNo ratings yet
- JCurrResSciMed5168-3449296 093452Document3 pagesJCurrResSciMed5168-3449296 093452Gihan NakhlehNo ratings yet
- BR J Anaesth 2014 112 529 539Document11 pagesBR J Anaesth 2014 112 529 539Gihan NakhlehNo ratings yet
- Amelie Theme Yann Tiersen PDFDocument4 pagesAmelie Theme Yann Tiersen PDFFabrizio BrezzoNo ratings yet
- EctopicDocument15 pagesEctopicquester1515No ratings yet
- Shoulder DystociaDocument43 pagesShoulder DystociaGihan NakhlehNo ratings yet
- Treatment of Opiate Withdrawal TableDocument4 pagesTreatment of Opiate Withdrawal TableGihan NakhlehNo ratings yet
- Wrist AnatomyDocument33 pagesWrist AnatomyGihan NakhlehNo ratings yet
- Menopause PDFDocument25 pagesMenopause PDFGihan NakhlehNo ratings yet
- Chronic Venous Insufficiency: Causes, Symptoms, Diagnosis and TreatmentDocument40 pagesChronic Venous Insufficiency: Causes, Symptoms, Diagnosis and TreatmentGihan NakhlehNo ratings yet
- Chronic Venous Insufficiency: Causes, Symptoms, Diagnosis and TreatmentDocument40 pagesChronic Venous Insufficiency: Causes, Symptoms, Diagnosis and TreatmentGihan NakhlehNo ratings yet
- Plato 1Document2 pagesPlato 1Gihan NakhlehNo ratings yet
- Vaginal Discharge PresentationDocument2 pagesVaginal Discharge PresentationGihan NakhlehNo ratings yet
- Klatskin TumorDocument17 pagesKlatskin TumorGihan NakhlehNo ratings yet
- Grade 12 Outdoor RecreationDocument24 pagesGrade 12 Outdoor RecreationHeherson Mel AgaciaNo ratings yet
- Sexual Harassment Against Women in The FIFO Mining IndustryDocument178 pagesSexual Harassment Against Women in The FIFO Mining IndustryPramesthi Dinar Kirana RatriNo ratings yet
- Dove's Selfie Documentary CampaignDocument5 pagesDove's Selfie Documentary CampaignAqib AteeqNo ratings yet
- Chufa Tubers (Cyperus Esculentus L.) As A New Source of FoodDocument7 pagesChufa Tubers (Cyperus Esculentus L.) As A New Source of FoodMARIAFERNANDA YULISSA TICONA ARTEAGANo ratings yet
- Swiz RN ResumeDocument1 pageSwiz RN Resumeapi-281795745No ratings yet
- Factors Influenci NG Perceptio N Stages of Perceptio N Response Perceiver Target Situation Select Organize Interpret RetrieveDocument2 pagesFactors Influenci NG Perceptio N Stages of Perceptio N Response Perceiver Target Situation Select Organize Interpret RetrieveFrances Marella CristobalNo ratings yet
- Cardiac Anesthesia: Saudi Board Anesthesia CurriculumDocument6 pagesCardiac Anesthesia: Saudi Board Anesthesia CurriculumHany ElbarougyNo ratings yet
- Expat Insider 2019 - The InterNations Survey - 0Document116 pagesExpat Insider 2019 - The InterNations Survey - 0tarmiricmyNo ratings yet
- Ceylon Cinnamon ReviewDocument11 pagesCeylon Cinnamon ReviewSuresh KumarNo ratings yet
- Leyna Slivka-5Document1 pageLeyna Slivka-5api-490419585No ratings yet
- Care Plan: Assessment DataDocument15 pagesCare Plan: Assessment Dataapi-509452165No ratings yet
- Opioid-Free AnesthesiaDocument8 pagesOpioid-Free AnesthesiaPaulina LugoNo ratings yet
- Functional Training Benefits & Core ExercisesDocument11 pagesFunctional Training Benefits & Core ExercisesSunny EggheadNo ratings yet
- Mental Health DepressionDocument4 pagesMental Health DepressionKAIZEN KINGZNo ratings yet
- Screening of Endophytic Bacteria From Organic Rice Tissue For Indole Acetic Acid ProductionDocument7 pagesScreening of Endophytic Bacteria From Organic Rice Tissue For Indole Acetic Acid ProductionSyed Muazzam Shah PutraNo ratings yet
- Minor II-Sem 2022-23 NonUGFY r1 1675060326Document5 pagesMinor II-Sem 2022-23 NonUGFY r1 1675060326Ritwick RanjanNo ratings yet
- TIKI: Titles for Treating Hypoxemia with Non-Invasive VentilationDocument8 pagesTIKI: Titles for Treating Hypoxemia with Non-Invasive Ventilationcharlyn206No ratings yet
- CNUR 860 Stats - Winter 2023 Nurse Fatigue AbstractDocument3 pagesCNUR 860 Stats - Winter 2023 Nurse Fatigue AbstractAlvia MagnoNo ratings yet
- Ida InfographicDocument2 pagesIda InfographicErica Lim MagtuloyNo ratings yet
- Prism 3 L&S-51-100Document50 pagesPrism 3 L&S-51-100bui thangNo ratings yet
- Ovary Female Reproductive SystemDocument1 pageOvary Female Reproductive SystemtheodorastanerNo ratings yet
- Lesson 2 - BTVNDocument3 pagesLesson 2 - BTVNHoàng HiềnNo ratings yet
- PDF097Document1 pagePDF097Hao LuoNo ratings yet