You might also like
- Name: Muhyee S. Idjad Year&Sec: BSNIII-B: What Is in A Emergency Cart?Document3 pagesName: Muhyee S. Idjad Year&Sec: BSNIII-B: What Is in A Emergency Cart?Yeng Cries50% (2)
- Preterm Labor and PROMDocument102 pagesPreterm Labor and PROMDan Matthew BuriasNo ratings yet
- 6.antifungal AgentsDocument51 pages6.antifungal Agentsmulatumelese0% (1)
- Principles of Aseptic TechniqueDocument3 pagesPrinciples of Aseptic TechniqueDane CaumeranNo ratings yet
- Total Parenteral NutritionDocument33 pagesTotal Parenteral Nutritionzamurd76No ratings yet
- Drug StudyDocument15 pagesDrug StudyMarc AnchetaNo ratings yet
- Syphilis in Pregnancy Case ReportDocument28 pagesSyphilis in Pregnancy Case ReportmuhammadrubaiNo ratings yet
- Appraising Therapy Articles on Fondaparinux for STEMIDocument35 pagesAppraising Therapy Articles on Fondaparinux for STEMIExequiel DimaanoNo ratings yet
- CoughDocument47 pagesCoughKesava Dass100% (1)
- Fosfomycin TromethamineDocument9 pagesFosfomycin Tromethamine:)No ratings yet
- Drug Study: Memantine, Piperacillin/Tazobactam, Rivastigmine, Losartan, Aspirin, ClopidogrelDocument37 pagesDrug Study: Memantine, Piperacillin/Tazobactam, Rivastigmine, Losartan, Aspirin, ClopidogrelCarlmeister Ambray JudillaNo ratings yet
- Therapeutic Effects: Death of Rapidly Replicating Cells, ParticularlyDocument3 pagesTherapeutic Effects: Death of Rapidly Replicating Cells, ParticularlyMarc Louise DatoyNo ratings yet
- Paracetamol Dosage For ChildrenDocument14 pagesParacetamol Dosage For Childrenkevinhabakuk_88No ratings yet
- Aseptic TechniqueDocument3 pagesAseptic TechniqueAndreea FloryNo ratings yet
- Equivalent To Caffeine 5mg/ml Equivalent To Caffeine 5mg/mlDocument2 pagesEquivalent To Caffeine 5mg/ml Equivalent To Caffeine 5mg/mlatawa1No ratings yet
- Drug Analysis: Submitted By: GALICINAO, Gretta Shalou GDocument9 pagesDrug Analysis: Submitted By: GALICINAO, Gretta Shalou GggalicinaoNo ratings yet
- DOT for TB Treatment: Minnesota Health Dept GuideDocument2 pagesDOT for TB Treatment: Minnesota Health Dept Guideahsanraja123No ratings yet
- Nursing Management of SeizuresDocument7 pagesNursing Management of SeizuresEcaroh Hew SmailliwNo ratings yet
- Survanta PiDocument10 pagesSurvanta PiBas BaylonNo ratings yet
- Total Parenteral NutritionDocument6 pagesTotal Parenteral Nutritionpam23lozadaNo ratings yet
- Securing Airways and Suctioning Endotracheal TubesDocument28 pagesSecuring Airways and Suctioning Endotracheal TubesJohn Mark ParacadNo ratings yet
- Addison's DiseaseDocument9 pagesAddison's Diseaseash ashNo ratings yet
- Chikungunya FeverDocument15 pagesChikungunya FeverAyomide AlayandeNo ratings yet
- New Patient Assessment and Care PlanDocument4 pagesNew Patient Assessment and Care PlanRalph Lawrence Ruiz Tagorda0% (1)
- Approach to Febrile Child SeminarDocument52 pagesApproach to Febrile Child SeminarwoldemariamNo ratings yet
- Lactulose: (Enuluse, Kristalose, Duphalac, Chronulac Syrup)Document30 pagesLactulose: (Enuluse, Kristalose, Duphalac, Chronulac Syrup)FEllis LEoNo ratings yet
- Graves DseDocument5 pagesGraves DseHester Marie SimpiaNo ratings yet
- Web KFOG-jan-11Document16 pagesWeb KFOG-jan-11kutra3000No ratings yet
- TENOFOVIR (Tenofovir Disoproxil, Tenofovir Disoproxil Fumarate)Document1 pageTENOFOVIR (Tenofovir Disoproxil, Tenofovir Disoproxil Fumarate)maeNo ratings yet
- MimsDocument59 pagesMimsjalabanzaNo ratings yet
- Course in Obstetrics & Gynecology Contraception MethodsDocument44 pagesCourse in Obstetrics & Gynecology Contraception Methodsmustafa atayaNo ratings yet
- Case Presentation-ChickenpoxDocument41 pagesCase Presentation-ChickenpoxShaliniNo ratings yet
- Manage Urinary Incontinence & RetentionDocument13 pagesManage Urinary Incontinence & RetentionDeniela Jamaicy HerbertNo ratings yet
- Newborn Screening Policy Catarman Doctors Hospital, Inc.: University of Eastern PhilippinesDocument7 pagesNewborn Screening Policy Catarman Doctors Hospital, Inc.: University of Eastern PhilippinesGenn Medrano GirayNo ratings yet
- Hypovolemic Shock in Patient With Burn TraumaDocument11 pagesHypovolemic Shock in Patient With Burn TraumaSundhias Larashati100% (1)
- IV Medication Check-ListDocument7 pagesIV Medication Check-Listhewmour androidNo ratings yet
- Case Report UrticariaDocument9 pagesCase Report UrticariasunnnydayNo ratings yet
- Exercise As A Boost For The Health Promotion of The ElderlyDocument65 pagesExercise As A Boost For The Health Promotion of The ElderlyPeace OghoNo ratings yet
- Approach To HemoptysisDocument22 pagesApproach To HemoptysisNikhil PanjiyarNo ratings yet
- EMERGENCY DRUGS: A Drug StudyDocument8 pagesEMERGENCY DRUGS: A Drug StudyShaine WolfeNo ratings yet
- Chronic Otitis MediaDocument4 pagesChronic Otitis MediaOvyanda Eka MItraNo ratings yet
- Drug Study KidneyDocument9 pagesDrug Study Kidneymcnover22No ratings yet
- Pharmaceutical Care PlanDocument13 pagesPharmaceutical Care PlanMuhammad Mustafa IjazNo ratings yet
- Contraception Part1Document38 pagesContraception Part1zianab aliNo ratings yet
- Aklan State University Nursing Readings on Pyloric StenosisDocument5 pagesAklan State University Nursing Readings on Pyloric Stenosisensoooooooooo100% (1)
- د.عبد الزهره THE GYNAECOLOGICAL EXAMINATION-1 (Muhadharaty)Document29 pagesد.عبد الزهره THE GYNAECOLOGICAL EXAMINATION-1 (Muhadharaty)MohammedNo ratings yet
- Acute Urinary RetentionDocument14 pagesAcute Urinary RetentionTP RMadNo ratings yet
- Albacio Eddiva Dapli-An Magwilang MaspilDocument138 pagesAlbacio Eddiva Dapli-An Magwilang MaspilJustineNo ratings yet
- Postterm Pregnancy Risks & Management OptionsDocument5 pagesPostterm Pregnancy Risks & Management OptionsOmar MohammedNo ratings yet
- Sexually Transmitted InfectionsDocument34 pagesSexually Transmitted InfectionsMariana Creciun100% (1)
- Case Study Presented by Group 22 BSN 206: In-Depth View On CholecystectomyDocument46 pagesCase Study Presented by Group 22 BSN 206: In-Depth View On CholecystectomyAjiMary M. DomingoNo ratings yet
- Type B (Hib) Vaccine: Haemophilus InfluenzaeDocument2 pagesType B (Hib) Vaccine: Haemophilus InfluenzaeEnce MalatambanNo ratings yet
- Emily B. Baglione CRNA, BSN, MS,: Chief OB CRNA, Anesthesia Group of AlbanyDocument55 pagesEmily B. Baglione CRNA, BSN, MS,: Chief OB CRNA, Anesthesia Group of AlbanyAsyfiyaTami100% (1)
- Antipyretic: Emelia Mei Syarah (1748201110099)Document5 pagesAntipyretic: Emelia Mei Syarah (1748201110099)Rahma Amah100% (1)
- WHO - Acute Diarrhea - Racecadotril - Utk Stop DiareDocument29 pagesWHO - Acute Diarrhea - Racecadotril - Utk Stop Diaremarkus_danusantosoNo ratings yet
- Abruptio PlacentaeDocument4 pagesAbruptio PlacentaeMelissa Aina Mohd YusofNo ratings yet
- Cardiac Testing Role Risk Stratifying ED Chest PainDocument17 pagesCardiac Testing Role Risk Stratifying ED Chest PainGiorgiana pNo ratings yet
- Cardiac Effusions: Causes, Symptoms and DiagnosisDocument26 pagesCardiac Effusions: Causes, Symptoms and DiagnosisjsenocNo ratings yet
- The Comprehensiveness of Homoeopathy in Bronchial AsthmaDocument4 pagesThe Comprehensiveness of Homoeopathy in Bronchial AsthmaEditor IJTSRDNo ratings yet
- Athlete's FootDocument8 pagesAthlete's Footsneh1509No ratings yet
- Allergic Rhinitis: PathophysiologyDocument28 pagesAllergic Rhinitis: Pathophysiologysneh1509No ratings yet
- Carbon ChemistryDocument3 pagesCarbon Chemistrysneh1509No ratings yet
- Pathophysiology: Date of Revision: March 2, 2020 Peer Review Date: August 1, 2018Document30 pagesPathophysiology: Date of Revision: March 2, 2020 Peer Review Date: August 1, 2018sneh1509No ratings yet
- Blood Glucose Meter PDFDocument10 pagesBlood Glucose Meter PDFsneh1509No ratings yet
- Blood Glucose Meter PDFDocument10 pagesBlood Glucose Meter PDFsneh1509No ratings yet
- Chap 7 Mini Quiz AnswersDocument1 pageChap 7 Mini Quiz Answerssneh1509No ratings yet
- Stoichiometry Examples0Document3 pagesStoichiometry Examples0sneh1509No ratings yet
- Unit 2A Winter 2012Document70 pagesUnit 2A Winter 2012sneh1509No ratings yet
- UNIT 3A - Stiochiometry - Chemical Formulas & EquationsDocument119 pagesUNIT 3A - Stiochiometry - Chemical Formulas & Equationssneh1509No ratings yet
- UNIT 1 - Introduction: Matter & MeasurementDocument95 pagesUNIT 1 - Introduction: Matter & Measurementsneh1509No ratings yet
- UNIT 2C - Atoms, Ions and MoleculesDocument79 pagesUNIT 2C - Atoms, Ions and Moleculessneh1509No ratings yet
- UNIT 2C - Atoms, Ions and MoleculesDocument79 pagesUNIT 2C - Atoms, Ions and Moleculessneh1509No ratings yet
- Pharmacy PracticeDocument35 pagesPharmacy Practicesneh1509100% (1)
- Chem Lab ReportDocument6 pagesChem Lab Reportsneh1509No ratings yet
- (Canadian Public Health Association Safe School Study, 2003a) - (Solberg and Olweus, 2003)Document3 pages(Canadian Public Health Association Safe School Study, 2003a) - (Solberg and Olweus, 2003)sneh1509No ratings yet
- Lab ReportDocument5 pagesLab Reportsneh1509No ratings yet
- Lab ReportDocument5 pagesLab Reportsneh1509No ratings yet
- PDTDocument7 pagesPDTsneh1509No ratings yet
- EssayDocument3 pagesEssaysneh1509No ratings yet
- Chem Chap 5 Homework Winter 2012Document3 pagesChem Chap 5 Homework Winter 2012sneh1509No ratings yet
- Chap 5 Homework Winter 2012Document3 pagesChap 5 Homework Winter 2012sneh1509No ratings yet
- Biological Molecules ListDocument5 pagesBiological Molecules Listsneh1509No ratings yet
- Chemistry Lab Report - Qualitative AnalysisDocument4 pagesChemistry Lab Report - Qualitative Analysissneh1509100% (1)
- Parikh Sneh 100478966 List of HeadingsDocument5 pagesParikh Sneh 100478966 List of Headingssneh1509No ratings yet
- Industry Standard: What Are The Benefits For You?Document4 pagesIndustry Standard: What Are The Benefits For You?Zarnimyomyint MyintNo ratings yet
- Ari Globe Valve SupraDocument26 pagesAri Globe Valve SupraAi-samaNo ratings yet
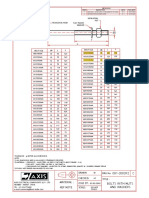
- Material: Ref Note: Rev # Description Appv. Rev DateDocument1 pageMaterial: Ref Note: Rev # Description Appv. Rev DateNimish TaterhNo ratings yet
- Polity by LaxmikantDocument3 pagesPolity by LaxmikantJk S50% (6)
- 737 Flow and ChecklistDocument7 pages737 Flow and ChecklistarelundhansenNo ratings yet
- Response of Hollow-Core Slab Floors To Concentrated LoadsDocument16 pagesResponse of Hollow-Core Slab Floors To Concentrated LoadsJuan Carlos GonzálezNo ratings yet
- Editable Classroom Officers TemplateDocument6 pagesEditable Classroom Officers TemplateRachelle AbalosNo ratings yet
- Republic of The Philippines, Petitioner, vs. Sandiganbayan, Major General Josephus Q. Ramas and Elizabeth Dimaano, RespondentsDocument23 pagesRepublic of The Philippines, Petitioner, vs. Sandiganbayan, Major General Josephus Q. Ramas and Elizabeth Dimaano, RespondentsKenzo RodisNo ratings yet
- KEB GM 2014 3 - enDocument109 pagesKEB GM 2014 3 - envankarpNo ratings yet
- ADUHAI @herman & Rhoca - Lyrics and Music by Rhoma Irama Arranged by - HERMAN - BOY - SmuleDocument4 pagesADUHAI @herman & Rhoca - Lyrics and Music by Rhoma Irama Arranged by - HERMAN - BOY - SmuleHERMAN BOYNo ratings yet
- Project Feasibility Study For The Establishment of Footwear and Other AccessoriesDocument12 pagesProject Feasibility Study For The Establishment of Footwear and Other Accessoriesregata4No ratings yet
- Macalintal v. PETDocument5 pagesMacalintal v. PETJazem AnsamaNo ratings yet
- Davall Stock Gears Worm Wheel Gear Sets 17pages PDFDocument17 pagesDavall Stock Gears Worm Wheel Gear Sets 17pages PDFharish ahireNo ratings yet
- Assignment 1 Front Sheet: Qualification BTEC Level 4 HND Diploma in BusinessDocument14 pagesAssignment 1 Front Sheet: Qualification BTEC Level 4 HND Diploma in BusinessQuan PhanNo ratings yet
- Experienced Welder Seeks New OpportunityDocument2 pagesExperienced Welder Seeks New OpportunityLen HebronNo ratings yet
- As 3566.1-2002 Self-Drilling Screws For The Building and Construction Industries General Requirements and MecDocument7 pagesAs 3566.1-2002 Self-Drilling Screws For The Building and Construction Industries General Requirements and MecSAI Global - APAC0% (2)
- Nov 2018 Pathfinder SkillsDocument162 pagesNov 2018 Pathfinder SkillsWaidi AdebayoNo ratings yet
- Post-Operative Nutrition: Things You Need To Know AboutDocument2 pagesPost-Operative Nutrition: Things You Need To Know AboutJannen CasasNo ratings yet
- 122 - Motion For Leave To File Rule 11 MotionDocument3 pages122 - Motion For Leave To File Rule 11 MotionRipoff ReportNo ratings yet
- Cameron VBR-II (Variable Bore Ram) PackerDocument2 pagesCameron VBR-II (Variable Bore Ram) Packerjuan olarteNo ratings yet
- EIE Resume FormatDocument1 pageEIE Resume FormatRakesh MandalNo ratings yet
- AfghanistanLML OnlinDocument117 pagesAfghanistanLML Onlinعارف حسینNo ratings yet
- (GUIDE) Advanced Interactive Governor Tweaks Buttery Smooth and Insane Battery Life! - Page 519 - Xda-DevelopersDocument3 pages(GUIDE) Advanced Interactive Governor Tweaks Buttery Smooth and Insane Battery Life! - Page 519 - Xda-Developersdadme010% (2)
- PMDC Renewal FormDocument3 pagesPMDC Renewal FormAmjad Ali100% (1)
- Anand FDocument76 pagesAnand FSunil BharadwajNo ratings yet
- UntitledDocument29 pagesUntitledsav 1011100% (1)
- Meritor 210 220 230 240 2SpeedSingleAxlesDocument27 pagesMeritor 210 220 230 240 2SpeedSingleAxlesYhojan DiazNo ratings yet
- How To Recover An XP Encrypted FileDocument2 pagesHow To Recover An XP Encrypted FileratnajitorgNo ratings yet
- Nasrullah March23Document11 pagesNasrullah March23Angellin JoiceNo ratings yet
- Gek 106852aDocument10 pagesGek 106852awednetoxNo ratings yet