You might also like
- Northern Ireland Management of Infection Guidelines For Primary and Community Care 2016Document48 pagesNorthern Ireland Management of Infection Guidelines For Primary and Community Care 2016dreneavalentinstefanNo ratings yet
- Drug CardsDocument3 pagesDrug CardsDave HillNo ratings yet
- (CV2) Pharmacology of AnticoagulantsDocument6 pages(CV2) Pharmacology of AnticoagulantsHanifa Shereen B. AliNo ratings yet
- Mu 002Document10 pagesMu 002chandanNo ratings yet
- Antibiotic GuideDocument6 pagesAntibiotic GuideAnnTran100% (1)
- Gout DrugsDocument1 pageGout DrugsMichael BrownNo ratings yet
- Opioid Analgesics Just in Time TrainingDocument16 pagesOpioid Analgesics Just in Time TrainingYel CMNo ratings yet
- AntibioticsDocument2 pagesAntibioticsPGI Custodio, Ed KristianNo ratings yet
- Aerovent, Apovent Atronase, Ipraxa, Ipvent Rhinovent, Rinatecrinovagos, Atrovent, Atrovent HfaDocument4 pagesAerovent, Apovent Atronase, Ipraxa, Ipvent Rhinovent, Rinatecrinovagos, Atrovent, Atrovent HfaGwyn RosalesNo ratings yet
- Pharmacology Drug ChartDocument50 pagesPharmacology Drug ChartEssentialForLivingNo ratings yet
- Renal Guide and Charts: AlbuminDocument16 pagesRenal Guide and Charts: AlbuminYaima JimenezNo ratings yet
- CANCER CHEMOTHERAPY REGIMENS AND THEIR TOXICITIESDocument13 pagesCANCER CHEMOTHERAPY REGIMENS AND THEIR TOXICITIESVaibhav Bharat100% (1)
- NERVOUS MnemonicsDocument4 pagesNERVOUS MnemonicsHimNo ratings yet
- 3 Treatment of HypertensionDocument7 pages3 Treatment of HypertensiontiaraNo ratings yet
- Mechanism of Action For Each Class of AntiDocument146 pagesMechanism of Action For Each Class of AntiReynaldo RiveraNo ratings yet
- Generic Name T Rade Name Classification Minitran Anti Angina NitroglycerinDocument1 pageGeneric Name T Rade Name Classification Minitran Anti Angina NitroglycerinChristopher LeeNo ratings yet
- Hypolipidemic DrugsDocument47 pagesHypolipidemic DrugsDr.U.P.Rathnakar.MD.DIH.PGDHM100% (1)
- Pharmacology A - NSAIDSDocument14 pagesPharmacology A - NSAIDSselflessdoctorNo ratings yet
- Critical Care Drug Reference SheetDocument12 pagesCritical Care Drug Reference SheetYanina CoxNo ratings yet
- Potassium-Sparing Diuretic Aldacton GuideDocument8 pagesPotassium-Sparing Diuretic Aldacton GuideJoy CalmerinNo ratings yet
- Antibiotics.: Prepared by L.Mbise OCTOBER 2012Document40 pagesAntibiotics.: Prepared by L.Mbise OCTOBER 2012Moses MberwaNo ratings yet
- Antidiarrheal DrugsDocument4 pagesAntidiarrheal DrugsNadhirah ZulkifliNo ratings yet
- Drugs Acting on Autonomic Nervous SystemDocument72 pagesDrugs Acting on Autonomic Nervous SystemDebashis ParidaNo ratings yet
- SAR of Macrolides, Penicillins, and Other AntibioticsDocument36 pagesSAR of Macrolides, Penicillins, and Other AntibioticsBen Paolo Cecilia RabaraNo ratings yet
- Vancomycin Protocol RQHRDocument15 pagesVancomycin Protocol RQHRl1o2stNo ratings yet
- Family Names of DrugsDocument1 pageFamily Names of DrugsangelNo ratings yet
- Indomethacin 392Document17 pagesIndomethacin 392Mahadie Hasan JahadNo ratings yet
- NHS Antibiotice PDFDocument2 pagesNHS Antibiotice PDFHoratiu OanaNo ratings yet
- Cardiovascular AgentsDocument22 pagesCardiovascular AgentsEsther Faith GabrielNo ratings yet
- Pharm Drug Outline AdrDocument1 pagePharm Drug Outline AdrCess Lagera YbanezNo ratings yet
- Classification of Drugs PDFDocument15 pagesClassification of Drugs PDFmuhammad ihtisham ul hassanNo ratings yet
- Drug TerminologyDocument5 pagesDrug Terminologyimdaking123No ratings yet
- DrugsDocument155 pagesDrugsAkankshaNo ratings yet
- ANTIDEPRESSANT DRUGS: Types, Mechanisms and Side EffectsDocument21 pagesANTIDEPRESSANT DRUGS: Types, Mechanisms and Side EffectsKashis SharmaNo ratings yet
- Drugs For GI DisordersDocument5 pagesDrugs For GI DisordersAalap ShahNo ratings yet
- Pharmacology of Volume and Vascular Tone RegulationDocument2 pagesPharmacology of Volume and Vascular Tone RegulationgraycorypNo ratings yet
- Anti Tubercular DrugsDocument63 pagesAnti Tubercular DrugsYasir KhanNo ratings yet
- Pharmacology Medical Suffixes Cheat SheetDocument1 pagePharmacology Medical Suffixes Cheat SheetPattyNo ratings yet
- Antibiotic Summary - DraftDocument10 pagesAntibiotic Summary - DraftStrept Pneumonia100% (1)
- Drug SuffixesDocument3 pagesDrug SuffixesjeromeasuncionNo ratings yet
- Different Body Receptors PDFDocument1 pageDifferent Body Receptors PDFSantosh patelNo ratings yet
- Pharmacology FirecrackerDocument37 pagesPharmacology FirecrackerRehan Usman100% (1)
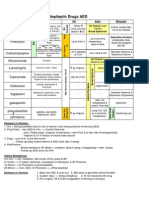
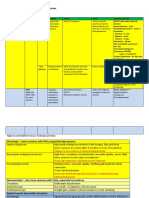
- Antiepileptic Drugs AED: D' DI Disadv SE AdvDocument1 pageAntiepileptic Drugs AED: D' DI Disadv SE Advrayooona88No ratings yet
- AntiemeticsDocument25 pagesAntiemeticsPridho GaziansyahNo ratings yet
- Drugclasses Pharmacologypart 1 PDFDocument25 pagesDrugclasses Pharmacologypart 1 PDFSutanya100% (2)
- Hypertension Drugs Cheat Sheet: by ViaDocument3 pagesHypertension Drugs Cheat Sheet: by ViaGulzaib KhokharNo ratings yet
- Classification of DrugsDocument10 pagesClassification of DrugsSafura IjazNo ratings yet
- Anxiety Disorders Treatment OptionsDocument5 pagesAnxiety Disorders Treatment OptionsJohn HolmesNo ratings yet
- Drug ClassDocument13 pagesDrug ClassEdfren Salazar Colon100% (1)
- Pharma GI CardsDocument16 pagesPharma GI CardsDoctorsHangout.comNo ratings yet
- Er-Drug StudyDocument41 pagesEr-Drug Studyrc_lacampuinganyahooNo ratings yet
- GI Pharmacology OverviewDocument24 pagesGI Pharmacology OverviewjenniferluzonNo ratings yet
- Tricyclic antidepressants overviewDocument2 pagesTricyclic antidepressants overviewAaLona RobinsonNo ratings yet
- Neuro Psych - Antiepileptic Drug ChartDocument5 pagesNeuro Psych - Antiepileptic Drug ChartMonica J Ortiz Pereira100% (1)
- Antibiotics 9Document11 pagesAntibiotics 9Beth Morales100% (1)
- ClindamycinDocument3 pagesClindamycinShaira TanNo ratings yet
- MedicineDocument3 pagesMedicineIntanNurjannahNo ratings yet
- Common infections and recommended antibioticsDocument3 pagesCommon infections and recommended antibioticsNicole BerryNo ratings yet
- RespiratoryDocument2 pagesRespiratoryJohn SmithNo ratings yet
- Pharmacology Table - GonzalesDocument14 pagesPharmacology Table - GonzalesMark Angelo PonferradoNo ratings yet
- Antipsychotic Medications To Know Table Jan 18Document5 pagesAntipsychotic Medications To Know Table Jan 18azhar hussinNo ratings yet
- Medications Table Part 2 Mood DisordersDocument2 pagesMedications Table Part 2 Mood Disordersazhar hussinNo ratings yet
- Eating Disorder and Obesity Two Main Types:: Emaciation, Amenorrhea, Brittle HairDocument2 pagesEating Disorder and Obesity Two Main Types:: Emaciation, Amenorrhea, Brittle Hairazhar hussinNo ratings yet
- 5 Antianxiety Medications Review TableDocument1 page5 Antianxiety Medications Review Tableazhar hussinNo ratings yet
- Review of ManuscriptDocument1 pageReview of Manuscriptazhar hussinNo ratings yet
- Uworld FileDocument2 pagesUworld Fileazhar hussinNo ratings yet
- USMLE Data12Document10 pagesUSMLE Data12azhar hussinNo ratings yet
- CBSE CalenderDocument12 pagesCBSE Calenderazhar hussinNo ratings yet
- Current Biologics of Spine Surgery APADocument11 pagesCurrent Biologics of Spine Surgery APAazhar hussinNo ratings yet
- Cbse ScheduleDocument4 pagesCbse Scheduleazhar hussinNo ratings yet
- Intravascular Extravascular: Fe Storage Tibc SerumDocument2 pagesIntravascular Extravascular: Fe Storage Tibc Serumazhar hussinNo ratings yet
- USMLE Data AzharDocument10 pagesUSMLE Data Azharazhar hussinNo ratings yet
- CBSE CalenderDocument12 pagesCBSE Calenderazhar hussinNo ratings yet
- Neurocognitive Disorders NotesDocument8 pagesNeurocognitive Disorders NotesJuanchovieldiazNo ratings yet
- Renal Stone Types, Causes and SymptomsDocument29 pagesRenal Stone Types, Causes and Symptomsarim100% (1)
- Physical Education: Quarter 2 - Module 2: WEEK 2, Active RecreationDocument47 pagesPhysical Education: Quarter 2 - Module 2: WEEK 2, Active RecreationNiko Igie Albino Pujeda100% (4)
- A Case Study In:: Hirschsprung DiseaseDocument18 pagesA Case Study In:: Hirschsprung DiseaseJaimie La PenaNo ratings yet
- Focused Ultrasonography For Septic Shock ResuscitationDocument7 pagesFocused Ultrasonography For Septic Shock ResuscitationntnquynhproNo ratings yet
- Fistula in AnoDocument12 pagesFistula in AnoWenna Grace OdtujanNo ratings yet
- 2019 BerryDocument15 pages2019 BerrybryaneatscamerasNo ratings yet
- Tuberculosis Control PlanDocument12 pagesTuberculosis Control PlanDominic EmerencianaNo ratings yet
- Frequencies found by Richard Loyd and John Loyd as of 2/12/2021Document4 pagesFrequencies found by Richard Loyd and John Loyd as of 2/12/2021Ricardo GomesNo ratings yet
- OBGYN Revalida Review 2019Document74 pagesOBGYN Revalida Review 2019anonymous100% (1)
- O.level Human Bio Edexcel Past Papers Paper 1 2019 - 2020Document68 pagesO.level Human Bio Edexcel Past Papers Paper 1 2019 - 2020Tamer AhmedNo ratings yet
- Pregnancy Induced Hypertension Case StudyDocument77 pagesPregnancy Induced Hypertension Case StudyATEHAN BORDS100% (1)
- AAO - External Disease and CorneaDocument19 pagesAAO - External Disease and CorneaJohn Paul VillaflorNo ratings yet
- Plastic Surgery Exam Questions and Answers1 PDFDocument468 pagesPlastic Surgery Exam Questions and Answers1 PDFFeliciaDewi100% (1)
- Ayurveda, YogaDocument34 pagesAyurveda, Yogayandi permanaNo ratings yet
- Chapter 29: Perinatal Disorders Garzon Maaks: Burns' Pediatric Primary Care, 7th EditionDocument2 pagesChapter 29: Perinatal Disorders Garzon Maaks: Burns' Pediatric Primary Care, 7th EditionHelen UgochukwuNo ratings yet
- West Minin CaseDocument2 pagesWest Minin CaseEUNICE MANATADNo ratings yet
- Aproach To Patient With FeverDocument61 pagesAproach To Patient With Feverfatima fatima92% (12)
- Witches HerbsDocument3 pagesWitches HerbsAM PNo ratings yet
- Final Oxygen Therapy and Monitoring Devices FM CommentedDocument56 pagesFinal Oxygen Therapy and Monitoring Devices FM CommentedDesalegnNo ratings yet
- The Erlangen Salivary Gland Project: Part I: Sialendoscopy in Obstructive Diseases of The Major Salivary GlandsDocument60 pagesThe Erlangen Salivary Gland Project: Part I: Sialendoscopy in Obstructive Diseases of The Major Salivary GlandsRosa Silva100% (1)
- African Traditional Medicine's Contributions to Nigeria's HealthcareDocument12 pagesAfrican Traditional Medicine's Contributions to Nigeria's HealthcareAliNo ratings yet
- Head Injuries ( Lesiones de Cabeza)Document5 pagesHead Injuries ( Lesiones de Cabeza)Camila BenitezNo ratings yet
- Deworming of PetsDocument5 pagesDeworming of PetsRehan Ashraf BandeshaNo ratings yet
- Automated Detection of Diabetic Foot With and Without Neuropathy Using Double Density-Dual Tree-Complex Wavelet Transform On Foot ThermogramsDocument32 pagesAutomated Detection of Diabetic Foot With and Without Neuropathy Using Double Density-Dual Tree-Complex Wavelet Transform On Foot ThermogramsLuis Martínez RamírezNo ratings yet
- How Do We Walk?: Sujay Galen PT PHD FheaDocument52 pagesHow Do We Walk?: Sujay Galen PT PHD FheaColleen JohnsonNo ratings yet
- Bab Vii Daftar PustakaDocument5 pagesBab Vii Daftar Pustaka19 110 Setya Maharani KadirNo ratings yet
- Mule AaDocument37 pagesMule AaShabaka KashataNo ratings yet
- NCLEX-RN - REVIEW - NOTES.2018-2019 by Saeid AskariDocument150 pagesNCLEX-RN - REVIEW - NOTES.2018-2019 by Saeid Askarireza babaAli100% (1)
- Ulthera Australia IFU2Document64 pagesUlthera Australia IFU2Cheeken CharliNo ratings yet