You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Kjim 2016 360Document11 pagesKjim 2016 360berriandi_arwanNo ratings yet
- News in SurgeryDocument9 pagesNews in Surgerymuthia khairunnisaNo ratings yet
- News in SurgeryDocument9 pagesNews in Surgerymuthia khairunnisaNo ratings yet
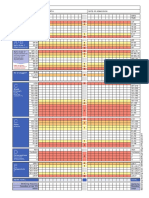
- NEWS2 Chart 3 - NEWS Observation Chart - 0Document1 pageNEWS2 Chart 3 - NEWS Observation Chart - 0muthia khairunnisaNo ratings yet
- Peripheral Vascular Disease Surgical PresentationDocument26 pagesPeripheral Vascular Disease Surgical PresentationqreenNo ratings yet
- NEWS2 Chart 1 - The NEWS Scoring System - 0 - 0Document1 pageNEWS2 Chart 1 - The NEWS Scoring System - 0 - 0Flouria Stefanny SimatupangNo ratings yet
- Physical Examination Vascular System: of TheDocument63 pagesPhysical Examination Vascular System: of TheyuniayuuuNo ratings yet
- Neonatal Sepsis Highlighting The Principles of Dia PDFDocument5 pagesNeonatal Sepsis Highlighting The Principles of Dia PDFmuthia khairunnisaNo ratings yet
- Tutor A21Document8 pagesTutor A21muthia khairunnisaNo ratings yet
- Review Article: Postcoital Bleeding: A Review On Etiology, Diagnosis, and ManagementDocument9 pagesReview Article: Postcoital Bleeding: A Review On Etiology, Diagnosis, and ManagementAnonymous i9mBoeOuNo ratings yet
- Jurnal EKG Abnormal Arif Rahman HakimDocument8 pagesJurnal EKG Abnormal Arif Rahman Hakimmuthia khairunnisaNo ratings yet
- Teknik Sungai Dan Rawa-05Document60 pagesTeknik Sungai Dan Rawa-05muthia khairunnisaNo ratings yet
- Lampiran Perhitungan Bab IvDocument5 pagesLampiran Perhitungan Bab Ivmuthia khairunnisaNo ratings yet
- Viral MeningitisDocument6 pagesViral Meningitismuthia khairunnisaNo ratings yet
- 1.c. What's The Impact of Shortness of Breath? AnswerDocument7 pages1.c. What's The Impact of Shortness of Breath? Answermuthia khairunnisaNo ratings yet
- Thacypnea PDFDocument4 pagesThacypnea PDFmuthia khairunnisaNo ratings yet
- Art 40930 PDFDocument13 pagesArt 40930 PDFBrahma MishraNo ratings yet
- SPSSDocument5 pagesSPSSmuthia khairunnisaNo ratings yet
- Jawaban Hakim Sken ADocument3 pagesJawaban Hakim Sken Amuthia khairunnisaNo ratings yet
- MUBESDocument2 pagesMUBESmuthia khairunnisaNo ratings yet
- Laporan Tugas Pengenalan Profesi Blok Xvi Sistem Sensoris Dan Integumentum "Identifikasi Gangguan Pendengaran Di Ypac"Document1 pageLaporan Tugas Pengenalan Profesi Blok Xvi Sistem Sensoris Dan Integumentum "Identifikasi Gangguan Pendengaran Di Ypac"muthia khairunnisaNo ratings yet
- Laporan Penanggungjawaban Lomba Cepat Tepat Spices 2018 FK Um PalembangDocument1 pageLaporan Penanggungjawaban Lomba Cepat Tepat Spices 2018 FK Um Palembangmuthia khairunnisaNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Controlled Delivery SystemsDocument12 pagesControlled Delivery SystemsSusan NyaguthiìNo ratings yet
- Clinical Pharmacology of Dobutamine and Dopamine in Preterm NeonatesDocument9 pagesClinical Pharmacology of Dobutamine and Dopamine in Preterm Neonatesmateri posNo ratings yet
- Clinical Research Regulatory Associate in Philadelphia PA Resume Deborah BaldwinDocument3 pagesClinical Research Regulatory Associate in Philadelphia PA Resume Deborah BaldwinDeborahBaldwinNo ratings yet
- Final NeuronotesDocument16 pagesFinal Neuronotesapi-479939114No ratings yet
- Tugas Mandiri Babak 8 Pasien Safety 2Document4 pagesTugas Mandiri Babak 8 Pasien Safety 2Andy NuriyantoNo ratings yet
- Gordon Feldman at 01 - 14 - 2023 09 - 19 PMDocument5 pagesGordon Feldman at 01 - 14 - 2023 09 - 19 PMschoolgirl7796No ratings yet
- Pradeep Project FileDocument25 pagesPradeep Project FilePradeep DhakadNo ratings yet
- Bioisosterismo - RevisãoDocument27 pagesBioisosterismo - RevisãoCLARA VITORIA CAVALCANTE CARVALHONo ratings yet
- Fmge Plan For June 2021Document4 pagesFmge Plan For June 2021holaNo ratings yet
- Drug Study (Aspirin)Document3 pagesDrug Study (Aspirin)Mae Therese B. MAGNONo ratings yet
- Anticoagulant Drugs (HEPARIN)Document1 pageAnticoagulant Drugs (HEPARIN)KyrrielJimenoCeladaNo ratings yet
- Cushing's Syndrome, Addison's Disease and Hyperparathyroidism.Document29 pagesCushing's Syndrome, Addison's Disease and Hyperparathyroidism.pranjl100% (1)
- Phytochemistry and Pharmacology of PhyllanthusDocument25 pagesPhytochemistry and Pharmacology of PhyllanthusGREESTYNo ratings yet
- Sacubitril/Valsartan (Entresto) : Safe Prescribing and Use ofDocument1 pageSacubitril/Valsartan (Entresto) : Safe Prescribing and Use ofpatricia wageyNo ratings yet
- Daftar Penawaran Harga PT Galoeh Husada Farma APRIL 2021Document2 pagesDaftar Penawaran Harga PT Galoeh Husada Farma APRIL 2021puskesmas tarokanNo ratings yet
- Aflac, Lumico, RNA Product InfoDocument12 pagesAflac, Lumico, RNA Product InfoJeromy KovatanaNo ratings yet
- 83 Siadh2 PDFDocument8 pages83 Siadh2 PDFAnonymous QNYOxtHNo ratings yet
- Drugfacts MdmaDocument5 pagesDrugfacts MdmaЕкатерина ДрагомирецкаяNo ratings yet
- Antibiotics FluoroquinolonesDocument35 pagesAntibiotics Fluoroquinolonesmirza_baig_46No ratings yet
- Promotional Medical Education Writer in New York City Resume Louise RozikDocument2 pagesPromotional Medical Education Writer in New York City Resume Louise RozikLouiseRozikNo ratings yet
- Shredder Capacity - Bio Medical WasteDocument3 pagesShredder Capacity - Bio Medical WasteYasser FathiNo ratings yet
- Tocolytic DrugDocument11 pagesTocolytic DrugWan Ahmad FaizFaizalNo ratings yet
- Pengenceran InjeksiDocument6 pagesPengenceran InjeksiMaria Wiji PangestuNo ratings yet
- Drug Lab Interaction FinalDocument133 pagesDrug Lab Interaction FinalJunnin Gay GarayNo ratings yet
- Obsessive-Compulsive Disorder Case Study - Group 3 (REVISED)Document41 pagesObsessive-Compulsive Disorder Case Study - Group 3 (REVISED)Mariah Ainna B. MatienzoNo ratings yet
- Flutivate e CreamDocument9 pagesFlutivate e Creamseema sharmaNo ratings yet
- Central Nervous System Concept Map (Ling)Document1 pageCentral Nervous System Concept Map (Ling)Jacob Kennedy LipuraNo ratings yet
- 2-1 Pharmaceutical Product Development 2340644 - 635535097882656250Document39 pages2-1 Pharmaceutical Product Development 2340644 - 635535097882656250Nadia PerezNo ratings yet
- Literature CitedDocument6 pagesLiterature CitedFlora Fauna FlavourNo ratings yet
- 3/2 CBC - Na - K - Crea - TPAG - CXR Post Intubation - ABG - Eta GscsDocument2 pages3/2 CBC - Na - K - Crea - TPAG - CXR Post Intubation - ABG - Eta GscserikaNo ratings yet