You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5796)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Stuart Stress Adaptation Model of Psychiatric Nursing CareDocument3 pagesThe Stuart Stress Adaptation Model of Psychiatric Nursing CareScott PuckettNo ratings yet
- Newborn Complications PowerPoint OutlineDocument8 pagesNewborn Complications PowerPoint OutlineScott PuckettNo ratings yet
- Chapter 20 Managing Quality and Risk (Ian)Document8 pagesChapter 20 Managing Quality and Risk (Ian)Scott PuckettNo ratings yet
- Chapter 1 OutlineDocument7 pagesChapter 1 OutlineScott PuckettNo ratings yet
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- 2010 First Yr First I Sem SyllabusDocument36 pages2010 First Yr First I Sem SyllabusNarayana SwamyNo ratings yet
- Cat Oxsilan InternetDocument49 pagesCat Oxsilan InternetAnonymous 1vuTwJVDjYNo ratings yet
- Export Value DeclarationDocument1 pageExport Value DeclarationdocrmpjodNo ratings yet
- IDOC As Web ServiceDocument40 pagesIDOC As Web ServiceUmesh Nanjaiah100% (2)
- Tesla - Tunguska Explosion 1908 PDFDocument9 pagesTesla - Tunguska Explosion 1908 PDFMircea Gabriel BalanNo ratings yet
- Design of Septic TankDocument6 pagesDesign of Septic TankJanissaries NivercaNo ratings yet
- Healthcare SCM in Malaysia - Case StudyDocument10 pagesHealthcare SCM in Malaysia - Case StudyHussain Alam100% (1)
- A Three-Stage Layer-Based Heuristic To Solve The 3D Bin-Packing ProblemDocument7 pagesA Three-Stage Layer-Based Heuristic To Solve The 3D Bin-Packing ProblemEder NingunoNo ratings yet
- Applied Soft Computing: Sandeep Singh Chauhan, Prakash KotechaDocument20 pagesApplied Soft Computing: Sandeep Singh Chauhan, Prakash KotechaCESARPINEDANo ratings yet
- Mouthwash, PEG, Sulfate, Betaine FreeDocument2 pagesMouthwash, PEG, Sulfate, Betaine FreerekhilaNo ratings yet
- Bill Book SystermDocument10 pagesBill Book SystermNiraj MishraNo ratings yet
- Negotiable Instruments Amendment Act 2015Document6 pagesNegotiable Instruments Amendment Act 2015Latest Laws Team100% (1)
- RM Practical FileDocument59 pagesRM Practical Filegarvit sharmaNo ratings yet
- Midview of 2Document4 pagesMidview of 2api-285760777No ratings yet
- GRADE 9-National Reading ProgramDocument2 pagesGRADE 9-National Reading ProgramJulius Bayaga100% (1)
- Case Study Analysis On Reinventing The Wheel at Apex Door CompanyDocument5 pagesCase Study Analysis On Reinventing The Wheel at Apex Door CompanySivachandran RNo ratings yet
- On Tap Giua Ky 2 MoiDocument9 pagesOn Tap Giua Ky 2 MoiPhương LêNo ratings yet
- English For Military PersonnelDocument9 pagesEnglish For Military PersonnelGilang Satia LaksanaNo ratings yet
- Schramm 2014Document6 pagesSchramm 2014Sexy BooksNo ratings yet
- One Plus Case StudyDocument9 pagesOne Plus Case StudyShubham Shimpi50% (2)
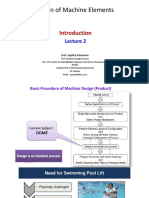
- Design of Machine Elements: Prof. Sujatha SrinivasanDocument27 pagesDesign of Machine Elements: Prof. Sujatha Srinivasanraviraj kumarNo ratings yet
- Revealed Comparative AdvantageDocument5 pagesRevealed Comparative AdvantageiamrahulkumarNo ratings yet
- 7UT51x Manual UsDocument232 pages7UT51x Manual UsMtdb Psd100% (1)
- CH 1 MCQ ETIDocument14 pagesCH 1 MCQ ETIShlok PurohitNo ratings yet
- A Level NdebeleDocument5 pagesA Level Ndebelenokwandadlamini2010No ratings yet
- Freshers - HR Interview Questions at AccentureDocument3 pagesFreshers - HR Interview Questions at Accenturebtrecio03No ratings yet
- ISO 261 EN 2010 - Page2 PDFDocument1 pageISO 261 EN 2010 - Page2 PDFd3bilNo ratings yet
- Lipa City Colleges Graduate SchoolDocument7 pagesLipa City Colleges Graduate SchoolRenz BrionesNo ratings yet
- Solar Brochure February 2023Document24 pagesSolar Brochure February 2023prakistaoNo ratings yet
- A Study On Customer Awareness and Satisfaction Towards Flipkart Shopping - With Special Reference To Pollachi TalukDocument4 pagesA Study On Customer Awareness and Satisfaction Towards Flipkart Shopping - With Special Reference To Pollachi TalukMukul SomgadeNo ratings yet