You might also like
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- EPT Practical 1Document10 pagesEPT Practical 1roshanleung11No ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5795)
- SAH & AneurysmDocument32 pagesSAH & Aneurysmroshanleung11No ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Cardio Practical 1Document6 pagesCardio Practical 1roshanleung11No ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Increased Intracranial PressureDocument38 pagesIncreased Intracranial Pressureroshanleung11No ratings yet
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Myasthenia GravisDocument21 pagesMyasthenia Gravisroshanleung11No ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Medical MXDocument8 pagesMedical MXroshanleung11No ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- GoutyDocument27 pagesGoutyroshanleung11No ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Respiratory TechniqueDocument6 pagesRespiratory Techniqueroshanleung11No ratings yet
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Tracking - 4x Per Week - BL - FLDocument16 pagesTracking - 4x Per Week - BL - FLroshanleung11No ratings yet
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- OMT Basic Spinal ManipulationDocument42 pagesOMT Basic Spinal Manipulationroshanleung11100% (1)
- Introduction + Ask For Consent Contraindications: Check MachineDocument10 pagesIntroduction + Ask For Consent Contraindications: Check Machineroshanleung11No ratings yet
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- MSK IV PracticalDocument10 pagesMSK IV Practicalroshanleung11No ratings yet
- 0612-88-510 Balanced Surg TechDocument60 pages0612-88-510 Balanced Surg TechAnonymous a3JsNXNNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Achilles Tendon Repair Protocol-PDF-EnDocument2 pagesAchilles Tendon Repair Protocol-PDF-Enckpravin7754No ratings yet
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Anita Williams - Footwear and Foot OrthosesDocument169 pagesAnita Williams - Footwear and Foot OrthosesRukaphuong100% (1)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Clubfoot PresentationDocument74 pagesClubfoot Presentationnovia khairulbaria100% (2)
- Patellofemoral Pain Syndrome (Runner'S Knee)Document2 pagesPatellofemoral Pain Syndrome (Runner'S Knee)Dewi IrfanNo ratings yet
- Pediatric Flatfoot Case StudyDocument1 pagePediatric Flatfoot Case StudyFirman Gilang MahardikaNo ratings yet
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Lower ExtremitiesDocument8 pagesLower ExtremitiesAngel Clarisse JariolNo ratings yet
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Chapter 19Document10 pagesChapter 19poNo ratings yet
- The Superficial Fibular Nerve - Course - Motor - TeachMeAnatomyDocument2 pagesThe Superficial Fibular Nerve - Course - Motor - TeachMeAnatomyLaiba AliNo ratings yet
- Front of Thigh, Femoral Triangle and Femoral VesselsDocument35 pagesFront of Thigh, Femoral Triangle and Femoral Vesselsgospel munkondya100% (1)
- Coughlin & MannDocument4,539 pagesCoughlin & MannNicholas CampitelliNo ratings yet
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Zumba Fitness Lesson PlanDocument2 pagesZumba Fitness Lesson PlanDivinity Of The Sun67% (3)
- Idoc - Pub - Kai Greene Leg Workoutpdf PDFDocument2 pagesIdoc - Pub - Kai Greene Leg Workoutpdf PDFPratap YedlaNo ratings yet
- Algoritma Pemilihan AFODocument4 pagesAlgoritma Pemilihan AFOYeanita Thenar100% (2)
- Supp Hip OnlyDocument20 pagesSupp Hip OnlyMark M. AlipioNo ratings yet
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Dr. Europa/ BaquiranDocument1 pageDr. Europa/ BaquiranSushmica BaquiranNo ratings yet
- ACL Rehabilitation ProgressionDocument8 pagesACL Rehabilitation ProgressionTomaž Radko Erjavec ŠnebergerNo ratings yet
- v1 500197 Reva Navio 7 All Knees Surgical Technique 06.19Document52 pagesv1 500197 Reva Navio 7 All Knees Surgical Technique 06.19febyan yohanesNo ratings yet
- MRI of The Foot: Muhammad Ali, MB BS Tim S. Chen, MD John V. Crues, III, MDDocument10 pagesMRI of The Foot: Muhammad Ali, MB BS Tim S. Chen, MD John V. Crues, III, MDOralBoards100% (1)
- Dr. Mike Israetel Training Volume Landmarks Hypertrophy Routine - LiftVault - Com - Sets Per Week SummaryDocument1 pageDr. Mike Israetel Training Volume Landmarks Hypertrophy Routine - LiftVault - Com - Sets Per Week SummaryrobertNo ratings yet
- Side Kick Height TrainingDocument12 pagesSide Kick Height TrainingTiago MinelliNo ratings yet
- Sports MannequinDocument64 pagesSports MannequinPalta HassNo ratings yet
- PPTDocument17 pagesPPTnimi mem0nNo ratings yet
- Ankle Sprain Rehab 1Document3 pagesAnkle Sprain Rehab 1John NixonNo ratings yet
- Propiocepcion RodillaDocument6 pagesPropiocepcion RodillaANDREA MONROY MEDRANONo ratings yet
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Primary THA in DDH Crow's 2&3: Manor Hospital Walsall A Teaching Trust of University of BirminghamDocument32 pagesPrimary THA in DDH Crow's 2&3: Manor Hospital Walsall A Teaching Trust of University of BirminghamDr Meenakshi ParwaniNo ratings yet
- Clubfoot (Congenital Talipes Equinovarus) - Pediatrics - OrthobulletsDocument8 pagesClubfoot (Congenital Talipes Equinovarus) - Pediatrics - OrthobulletsdewiswahyuNo ratings yet
- Kai Greene Leg WorkoutDocument2 pagesKai Greene Leg Workoutdr.menganeNo ratings yet
- How To Deadlift - The Definitive Guide - Stronger by ScienceDocument142 pagesHow To Deadlift - The Definitive Guide - Stronger by ScienceNilgunNo ratings yet
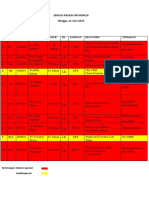
- Sensus Pasien Orthopedi Minggu, 21 JULI 2019: No Bed No - RM Nama Umur JK Jaminan Diagnosis TindakanDocument3 pagesSensus Pasien Orthopedi Minggu, 21 JULI 2019: No Bed No - RM Nama Umur JK Jaminan Diagnosis TindakanWa JulianiNo ratings yet