You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5806)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (842)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- QuizBowl QuestionsDocument84 pagesQuizBowl QuestionsJowel MercadoNo ratings yet
- SEC - Connection Guidelines - v3 - CleanDocument54 pagesSEC - Connection Guidelines - v3 - CleanFurqan HamidNo ratings yet
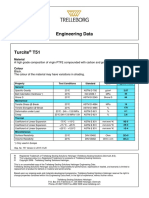
- Turcite T51 Engineering DataDocument1 pageTurcite T51 Engineering DataAntonio Rivera VillavicencioNo ratings yet
- Irving Hallowell - Ojibwa Ontology, Behavior and World ViewDocument24 pagesIrving Hallowell - Ojibwa Ontology, Behavior and World ViewFa Di LaNo ratings yet
- Sarmatian Swords 2 - ROMECDocument12 pagesSarmatian Swords 2 - ROMECkulcsarv100% (2)
- Spesifikasi Vista 120 S Patient Monitor - StandardDocument2 pagesSpesifikasi Vista 120 S Patient Monitor - StandardHadi AtmojoNo ratings yet
- Unit Operation QBDocument7 pagesUnit Operation QBsmg26thmayNo ratings yet
- BCB NO1) Bearing CatalogDocument17 pagesBCB NO1) Bearing CatalogGabriela TorresNo ratings yet
- Training Sinal PDFDocument15 pagesTraining Sinal PDFlobitoferoz81No ratings yet
- Bastidas Et Al, 2010Document8 pagesBastidas Et Al, 2010Panji Satria N.No ratings yet
- RymesDocument6 pagesRymesFarida YesminNo ratings yet
- RfI SB Listening ScriptsDocument18 pagesRfI SB Listening ScriptsKate PolissyaNo ratings yet
- Our Changing WorldDocument3 pagesOur Changing Worlddinesh869863% (8)
- Falsework For Concrete Structures - Guidelines: Indian StandardDocument24 pagesFalsework For Concrete Structures - Guidelines: Indian StandardLivinston JosephNo ratings yet
- Training Schedule April 2021 To March 22 - 0Document18 pagesTraining Schedule April 2021 To March 22 - 0sanrexiNo ratings yet
- Distance Relay BasicsDocument58 pagesDistance Relay Basicsaalamz93_854917254100% (1)
- Wednesday 12 June 2019: ChemistryDocument32 pagesWednesday 12 June 2019: ChemistryMohammad KhanNo ratings yet
- FAB-3021117-01-M01-ER-001 - Rev-0 SK-01 & 02Document91 pagesFAB-3021117-01-M01-ER-001 - Rev-0 SK-01 & 02juuzousama1No ratings yet
- Catchment CharacterisationDocument48 pagesCatchment CharacterisationSherlock BaileyNo ratings yet
- Ecs C42iix Rev C Vit m2400 1Document36 pagesEcs C42iix Rev C Vit m2400 1Victor Pic100% (1)
- GFB V2 - VNT Boost Controller: (Part # 3009)Document2 pagesGFB V2 - VNT Boost Controller: (Part # 3009)blumng100% (1)
- Keeling 1960 PDFDocument4 pagesKeeling 1960 PDFErick AmâncioNo ratings yet
- AUSMAT Student Guide 2011Document16 pagesAUSMAT Student Guide 2011Sunway UniversityNo ratings yet
- Radiation Physics and Chemistry: L.T. Hudson, J.F. SeelyDocument7 pagesRadiation Physics and Chemistry: L.T. Hudson, J.F. SeelyThư Phạm Nguyễn AnhNo ratings yet
- 2b. TESDA-OP-CO-01-F14 TOOLSDocument2 pages2b. TESDA-OP-CO-01-F14 TOOLSRommel SelgaNo ratings yet
- Idioms & PhrasesDocument4 pagesIdioms & PhrasesHimadri Prosad RoyNo ratings yet
- Installiation of Automatic Fire Sprinkler System and Design CalculationDocument8 pagesInstalliation of Automatic Fire Sprinkler System and Design CalculationSat AungNo ratings yet
- Unit 2Document9 pagesUnit 2Quinn LilithNo ratings yet
- Montague Street Cable Car, Wall Street FerryDocument23 pagesMontague Street Cable Car, Wall Street FerryBob DiamondNo ratings yet
- Mary Szybist On Visual Poetry Compressed PDFDocument5 pagesMary Szybist On Visual Poetry Compressed PDFcarlos.enrique.fonseca1440No ratings yet