Professional Documents
Culture Documents
Vespignani Covid
Uploaded by
De Nicolas JaidarOriginal Title
Copyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
Vespignani Covid
Uploaded by
De Nicolas JaidarCopyright:
Available Formats
Articles
Evolving epidemiology and transmission dynamics of
coronavirus disease 2019 outside Hubei province,
China: a descriptive and modelling study
Juanjuan Zhang*, Maria Litvinova*, Wei Wang*, Yan Wang, Xiaowei Deng, Xinghui Chen, Mei Li, Wen Zheng, Lan Yi, Xinhua Chen, Qianhui Wu,
Yuxia Liang, Xiling Wang, Juan Yang, Kaiyuan Sun, Ira M Longini Jr, M Elizabeth Halloran, Peng Wu, Benjamin J Cowling, Stefano Merler,
Cecile Viboud, Alessandro Vespignani, Marco Ajelli†, Hongjie Yu†
Summary
Background The coronavirus disease 2019 (COVID-19) epidemic, caused by severe acute respiratory syndrome Lancet Infect Dis 2020;
coronavirus 2 (SARS-CoV-2), began in Wuhan city, Hubei province, in December, 2019, and has spread throughout 20: 793–802
China. Understanding the evolving epidemiology and transmission dynamics of the outbreak beyond Hubei would Published Online
April 2, 2020
provide timely information to guide intervention policy.
https://doi.org/10.1016/
S1473-3099(20)30230-9
Methods We collected individual information from official public sources on laboratory-confirmed cases reported See Comment page 756
outside Hubei in mainland China for the period of Jan 19 to Feb 17, 2020. We used the date of the fourth revision of *Contributed equally
the case definition (Jan 27) to divide the epidemic into two time periods (Dec 24 to Jan 27, and Jan 28 to Feb 17) as the
†Contributed equally
date of symptom onset. We estimated trends in the demographic characteristics of cases and key time-to-event
School of Public Health, Fudan
intervals. We used a Bayesian approach to estimate the dynamics of the net reproduction number (Rt) at the provincial University, Key Laboratory of
level. Public Health Safety, Ministry
of Education, Shanghai, China
(J Zhang PhD, W Wang MSc,
Findings We collected data on 8579 cases from 30 provinces. The median age of cases was 44 years (33–56), with an
Y Wang MSc, X Deng MSc,
increasing proportion of cases in younger age groups and in elderly people (ie, aged >64 years) as the epidemic Xing Chen BSc, M Li MSc,
progressed. The mean time from symptom onset to hospital admission decreased from 4·4 days (95% CI 0·0–14·0) W Zheng BSc, L Yi, Xin Chen BSc,
for the period of Dec 24 to Jan 27, to 2·6 days (0·0–9·0) for the period of Jan 28 to Feb 17. The mean incubation period Q Wu BSc, Y Liang BSc,
X Wang PhD, J Yang PhD,
for the entire period was estimated at 5·2 days (1·8–12·4) and the mean serial interval at 5·1 days (1·3–11·6). The
Prof H Yu PhD); ISI Foundation,
epidemic dynamics in provinces outside Hubei were highly variable but consistently included a mixture of case Turin, Italy (M Litvinova PhD,
importations and local transmission. We estimated that the epidemic was self-sustained for less than 3 weeks, with Prof A Vespignani PhD); Division
mean Rt reaching peaks between 1·08 (95% CI 0·74–1·54) in Shenzhen city of Guangdong province and of International Epidemiology
and Population Studies,
1·71 (1·32–2·17) in Shandong province. In all the locations for which we had sufficient data coverage of Rt, Rt was Fogarty International Center,
estimated to be below the epidemic threshold (ie, <1) after Jan 30. National Institutes of Health,
Bethesda, MD, USA (K Sun PhD,
Interpretation Our estimates of the incubation period and serial interval were similar, suggesting an early peak of C Viboud PhD); Department of
Biostatistics, College of Public
infectiousness, with possible transmission before the onset of symptoms. Our results also indicate that, as the Health, Health Professions, and
epidemic progressed, infectious individuals were isolated more quickly, thus shortening the window of transmission Emerging Pathogens Institute,
in the community. Overall, our findings indicate that strict containment measures, movement restrictions, and University of Florida,
increased awareness of the population might have contributed to interrupt local transmission of SARS-CoV-2 outside Gainesville, FL, USA
(Prof I M Longini Jr PhD);
Hubei province. Vaccine and Infectious Disease
Division, Fred Hutchinson
Funding National Science Fund for Distinguished Young Scholars, National Institute of General Medical Sciences, Cancer Research Center,
and European Commission Horizon 2020. Seattle, WA, USA
(Prof M E Halloran DSc);
Department of Biostatistics,
Copyright © 2020 Elsevier Ltd. All rights reserved. University of Washington,
Seattle, WA, USA
Introduction An early report5 on the epidemiology of the COVID-19 (Prof M E Halloran); WHO
Collaborating Centre for
Since December, 2019, an increasing number of atypical outbreak included analysis of the first 425 confirmed cases Infectious Disease
pneumonia cases caused by severe acute respiratory detected in Wuhan up to Jan 22, 2020. Since then, the Epidemiology and Control,
syndrome coronavirus 2 (SARS-CoV-2) have been reported temporal dynamics and spatial dissemination of COVID-19 School of Public Health, Li Ka
Shing Faculty of Medicine,
in Wuhan, a city in the Chinese province of Hubei.1 As of has changed, with 17% of cases reported outside of Hubei
University of Hong Kong, Hong
Feb 17, 2020, 72 436 cases of coronavirus disease 2019 in mainland China as of Feb 17. In provinces outside Kong Special Administrative
(COVID-19), including 1868 deaths, had been reported Hubei, the COVID-19 epidemic is characterised by a Region, China (P Wu PhD,
in mainland China.2 The outbreak has now spread to mixture of local transmission and importation of cases Prof B J Cowling PhD); Bruno
Kessler Foundation, Trento,
198 countries, areas, or territories beyond China.3 On from Hubei.6 A report6 based on the 44 672 confirmed
Italy (S Merler MSc,
Jan 30, 2020, WHO declared the COVID-19 outbreak a cases detected in mainland China up to Feb 11, gave a M Ajelli PhD); and Laboratory
public health emergency of international concern.4 description of the characteristics of COVID-19 cases for for the Modeling of Biological
www.thelancet.com/infection Vol 20 July 2020 793
Articles
and Socio-technical Systems,
Northeastern University, Research in context
Boston, MA USA
(Prof A Vespignani) Evidence before this study outside Hubei province up to Feb 17, accounting for 69% of all
Correspondence to: On March 12, 2020, we searched PubMed and Web of Science 12 447 reported cases at that time. We analysed changes in
Dr Marco Ajelli, Bruno Kessler for papers published after Jan 1, 2020, using the search terms demographic characteristics, key time-to-event intervals
Foundation, Trento, Italy (“nCoV” OR “COVID” OR “novel coronavirus” OR “severe acute (eg, incubation period, serial interval, and time from symptom
marco.ajelli@gmail.com
respiratory syndrome coronavirus 2”) AND (“evolving onset to hospital admission), and the dynamics of the net
or
epidemiology” OR “epidemiological characteristics” OR reproduction number (Rt) at the provincial level. We found
Prof Hongjie Yu, Fudan
“transmission dynamics” OR “net reproduction number”). significant differences in the epidemiology of COVID-19 as the
University, School of Public
Health, Key Laboratory of Public No language restrictions were applied. We identified 24 papers epidemic continued to spread across China. The time from
Health Safety, Ministry of published in peer-reviewed journals. We also included two symptom onset to hospital admission decreased from 4·4 days
Education, relevant papers that had yet to be indexed by PubMed or (95% CI 0·0–14·0) in the period of Dec 24 to Jan 27, to 2·6 days
Shanghai 200032, China
Web of Science. The study of the first confirmed 425 cases (0·0–9·0) in the period from Jan 28 to Feb 17. The mean
yhj@fudan.edu.cn
in Wuhan reported a mean incubation period of 5·2 days and incubation period was estimated at 5·2 days (95% CI 1·8–12·4)
a mean serial interval of 7·5 days. One study, based on and the mean serial interval at 5·1 days (1·3–11·6).
291 patients in China, estimated a median incubation period Most importantly, as of Feb 8, 2020, we estimated Rt to be
of 4 days, and another four studies estimated the incubation below the epidemic threshold in provinces outside Hubei that
period of cases outside Wuhan or Hubei ranging from 5 to have reported the largest number of cases (Hunan, Shandong,
6·7 days. One mathematical modelling study estimated that Shenzhen city [Guangdong province], Anhui, Henan,
the median daily net reproduction number in Wuhan declined Jiangsu, Jiangxi, Shaanxi, and Zhejiang).
from 2·35 (95% CI 1·15–4·77) 1 week before travel restrictions
Implications of all the available evidence
were introduced on Jan 23 to 1·05 (0·41–2·39) 1 week after.
We show that the epidemiology and transmission dynamics of
A report from the Chinese Center for Disease Control and
the COVID-19 epidemic are rapidly changing and should be
Prevention that was based on the analysis of 44 672 confirmed
closely monitored. Our findings suggest that strict containment
cases up to Feb 11, 2020, provided an overall description of
measures, movement restrictions, and increased awareness of
the characteristics of coronavirus disease 2019 (COVID-19)
the population might have contributed to controlling the
cases in China as a whole and in Hubei province. However, that
COVID-19 outbreak outside Hubei province in China. Given that
study did not provide estimates of key time-to-event intervals
the reproduction number is positively related to the growth rate
nor of the reproduction number. Until now, there has been
of the epidemic and the length of the serial interval, the shorter
scarce information to understand the changing
serial interval estimated here (5·1 days vs 7·5 days) implies that
epidemiological features and transmission dynamics of the
transmissibility of severe acute respiratory syndrome
COVID-19 outbreak beyond Hubei province.
coronavirus 2 might not be as high as previous estimates
Added value of this study suggest. More broadly, our findings are crucial to inform
We collected individual information from official, publicly intervention policy in real-time for other countries, given the
available sources on 8579 laboratory-confirmed cases detected international expansion of the COVID-19 epidemic.
mainland China and in Hubei. Until now, there has surveillance system, first in Wuhan, then extended
been little information on the epidemiological features to the entire country, to record information about
See Online for appendix and trans mission dynamics of the COVID-19 outbreak COVID-19 cases (appendix pp 2–3).1,5 Guidelines on
beyond Hubei. This information will be crucial to inform the diagnosis and treatment of patients with novel
intervention policy in real-time, not only for China, but coronavirus-infected pneumonia (NCIP) were pub
also for other countries with COVID-19 transmission. lished, with the first issued on Jan 15, 2020, defining a
We aimed to describe the epidemiological characteristics suspected NCIP case as pneumonia that fulfilled
of the COVID-19 outbreak 50 days after it was recognised specific clinical criteria and had an epidemiological link
in Chinese provinces outside Hubei. We also estimated to the Huanan seafood wholesale market in Wuhan or
changes in key time-to-event intervals and reproduction had travelled to Wuhan in the 14 days before symptom
numbers to assess whether the strict control measures onset (appendix pp 2–3). The subsequent two versions
put in place in China have been successful in slowing of the guidelines (the first issued on Jan 18 and the
transmission. second on Jan 22) removed the clinical criterion of no
symptomatic improvement or deterioration after 3 days
Methods of antibiotic treat ment to accelerate identification of
Case definitions and surveillance cases. Additionally, the epidemiological link was revised
Since the outbreak of COVID-19 was first detected to include travel history to Wuhan, direct contact
in Wuhan, the Chinese Center for Disease Control with patients from Wuhan who had fever or respiratory
and Prevention (China CDC) has launched a new symptoms within 14 days before symptom onset, or part
794 www.thelancet.com/infection Vol 20 July 2020
Articles
of a COVID-19 cluster. In the fourth version of the Provincial Health Commission, Shenzhen Municipal
guidelines (issued on Jan 27), the clinical criteria were Health Commission, and Hunan Provincial Health
broadened to meet any two of the three remaining Commission (appendix p 12).
clinical criteria (ie, fever, radiographic findings of
pneumonia, and normal or reduced white blood cell Statistical analysis
count or reduced lymphocyte count at early stage of We restricted analyses to provinces other than Hubei
illness), and an epidemiological criterion was added where the majority of individual records were available—
(link with a confirmed COVID-19 case). In the fifth ie, 8579 (98%) of 8738. We used the date of the fourth
version issued on Feb 4, clinically diagnosed cases were revision of the guidelines to divide the epidemic into
defined as suspected cases with radiographic findings of two time periods. The first period ran from the emergence
pneumonia, to be used exclusively in Hubei.7 of COVID-19 in provinces outside Hubei, Dec 24 to Jan 27,
This study was approved by the institutional review when the definition of suspected cases was broadened
board of the School of Public Health, Fudan University to capture milder cases. The second period ran from
(Shanghai, China). All data were collected from publicly Jan 28 to Feb 17. We did statistical analyses of demographic
available sources. Data were deidentified, and informed and epidemiological characteristics of confirmed cases
consent was waived. stratified by the two epidemic periods. χ² test was used to
compare the age and sex structure. Two-sample t test was
Data sources and collection used to compare the key time-to-event intervals.
All of the provinces outside Hubei were included in the We estimated key time-to-event distributions for
analysis of demographic characteristics, key time-to- COVID-19 cases, including symptom onset to first
event intervals, incubation period, and serial interval. health-care consultation, hospital admission, and official
Nine locations for which we had sufficient data coverage reporting. We estimated the time from infection to
were used to estimate the net reproduction number. symptom onset (ie, the incubation period) by analysing
Daily aggregated data on the number of cumulative COVID-19 cases with confirmed epidemiological links
cases in mainland China were extracted from the official (clusters) identified by prospective contact tracing. The
websites of national, provincial, and municipal health date of presumed infection was estimated from history
commissions (appendix pp 3–10). Individual records on of exposure, after excluding cases with exposure to
laboratory-confirmed COVID-19 cases were collected from Wuhan. When multiple exposures were reported, we
two publicly available official sources: the websites of considered the interval between the first and last
national, provincial, and municipal health commissions, recorded dates of exposure. We fit three parametric
and the websites of national and local government news distributions (Weibull, gamma, and lognormal) to time-
media. Individual information was extracted by the data to-event data and selected the best fit based on the
collection team and entered into a structured database minimum Akaike information criterion. Confidence
comprising three sections: demographic characteristics; intervals for the estimated distributions were obtained
exposure and travel history; and key timelines, including with 2000 bootstrap simulations for either censored or
exposure timeline, date of symptom onset, date of hospital non-censored data.
admission, and date of official reporting. A well trained We analysed clusters of COVID-19 cases with epi
data collection team of about 40 members from Fudan demiological links confirmed by prospective contact
University collected individual information (appendix tracing (all cases with travel history to Wuhan or Hubei—
pp 10, 11). Each individual record was cross-checked by ie, declared visiting or residing, where excluded) to
three coauthors (WW, MLi, and WZ), and consensus estimate the interval between onset of symptoms in a
was attained before finalising an entry in the database. primary (index) case and the onset of symptoms in
Conflicting information was resolved based on the secondary cases generated by that primary case (ie, the
original data source; for example, if individual records on serial interval). The serial interval was estimated by
local governmental websites and governmental news fitting a gamma distribution to the lag between the dates
media were inconsistent, we extracted the data from the of symptom onset in the index and secondary cases.
governmental website. We used information on age, sex, Using the estimated distribution of the serial interval,
location of detection, exposure history, dates of symptom we calculated the net reproduction number (Rt), which is
onset, hospital admission, and official reporting to des the mean number of secondary cases generated by a
cribe demographic characteristics of cases and estimate typical primary case at time t. Consecutive generations of
key time-to-event intervals, incubation period, serial inter cases arise after a period measured by the serial interval
val, and net reproduction number. Details on the collection or by the generation time.8 We used a Bayesian approach9,10
of individual data, the definitions of key variables, and the to estimate Rt from the time series of symptom onset dates
assessment of completeness of variables are provided in and the distribution of the serial interval, considering
the appendix (pp 3–11). importations and local transmission.11 For this analysis,
We validated our individual records against the official the last 9 days of the dataset were excluded to account
line lists obtained from the websites of Shandong for the possible incompleteness of the dataset due to
www.thelancet.com/infection Vol 20 July 2020 795
Articles
A
Hubei province
Shiyan
Heilongjiang
Xiangyang
Xinjiang Jilin Suizhou
Inner Mongolia
Shennongjia
Liaoning
Gansu
Beijing Jingmen
Xiaogan
Hebei Tianjin
Ningxia Shanxi Yichang Huanggang
Qinghai Shandong Tianmen Wuhan
Ezhou
Shaanxi Henan Qianjiang Xiantao
Tibet Jiangsu Enshi
Anhui Jingzhou Huangshi
Sichuan Hubei Shanghai
Chongqing Xianning
Jiangxi Zhejiang
Hunan
Guizhou
Yunnan Fujian
Guangxi Guangdong
Taiwan
Confirmed cases (N)
10–184
Guangdong 185−500
Hainan 501−1000
1001−2000
Macao Confirmed cases (N) 2001−3320
Hong Kong 0−100 1001−1328 42 752
101−200 59 989
201−500 Not applicable
Shenzhen 501−1000
B
Period 1 Period 2
550 Travel history to Wuhan or Hubei
Local transmission
COVID-19 incorporated as a notifiable disease in the
Infectious Disease Law and Health and Quarantine Law in China
500
Transportation leaving from Wuhan
temporarily locked down
450
400 The fourth version of the case
definition was issued
Number of confirmed cases (individual records)
350
WHO declared the COVID-19
outbreak a PHEIC
300
Test reagent issued to all provinces; first case
officially announced outside Hubei province
250
200
150
Huanan seafood RT-PCR reagents
100
First case in Wuhan wholesale market closed provided to Wuhan
50
0
1 4 7 10 13 16 19 22 25 28 31 3 6 9 12 15 18 21 24 27 30 2 5 8 11 14 17
December, 2019 January, 2020 February, 2020
Date of symptom onset
796 www.thelancet.com/infection Vol 20 July 2020
Articles
reporting delays. The methods used to estimate Rt are The presence of at least one known exposure was
reported in detail in the appendix (p 23). Throughout, reported by 6611 (77%) of 8579 cases (table 1). In the
95% CI refers to the 2·5th and 97·5th percentiles of the early epidemic period, most cases reported an exposure
estimated distribution. Statistical analyses were done in Wuhan or Hubei. Subsequently, an increasing
using R, version 3.6.0. Rt was estimated from a code number of cases reported exposure to COVID-19 cases
written by the authors, which is available online. or patients with acute respiratory infections (p<0·0001; For Rt code see https://github.
table 1). com/majelli/Rt
Role of the funding source The time from symptom onset to hospital admission
The funder of the study had no role in the study design, shortened as the epidemic progressed, decreasing from
data collection, data analysis, data interpretation, or 4·4 days (95% CI 0·0–14·0) during the first period of the
writing of the report. The corresponding authors had epidemic to 2·6 days (0·0–9·0) in the second period
full access to all the data in the study and had (table 2). A similar decreasing time trend was observed
final responsibility for the decision to submit for for the interval from symptom onset to first health-care
publication. consultation (table 2).
We analysed the time from exposure to illness onset for
Results 49 cases with no travel history who were identified by
As of Feb 17, 2020, 72 436 COVID-19 cases had been prospective contact tracing. These cases represented
reported in all 31 provinces of mainland China. 37 clusters. We estimated a mean incubation period of
42 752 (59%) of 72 436 cases were detected in Wuhan city 5·2 days (95% CI 1·8–12·4), with the 95th percentile of
of Hubei province, 17 237 (24%) were detected in cities the distribution at 10·5 days. The incubation period was
other than Wuhan in Hubei province, and 12 447 (17%) well approximated by a lognormal distribution (appendix
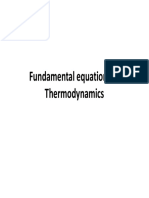
were reported in other provinces (figure 1A). We collected pp 17–19).
individual information on 8579 laboratory-confirmed We analysed the time between symptom onset in
cases detected outside Hubei up to Feb 17, accounting for 35 secondary cases and 28 corresponding primary cases
69% of the 12 447 cases reported at that time. For most of (appendix pp 19–22). One case who reported the onset of
the locations, there was consistency between the time symptoms on the same day as the index case was removed
series derived from our individual records and the official from the analysis. The serial interval followed a gamma
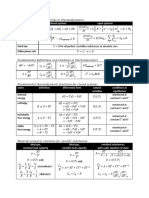
case reports (appendix pp 12–14). distribution with an estimated mean of 5·1 days (95% CI
Starting at the end of December, 2019, the COVID-19 1·3–11·6). A comparison of the distribution of the
epidemic grew rapidly outside Hubei and was characterised incubation period and the serial interval is reported in
by a mixture of local transmission and case importations figure 2, and shows overlap between the two distributions.
from Hubei (figure 1B). The median age of cases was As we cannot exclude that a fraction of these secondary
44 years (33–56), with the proportions of cases that were in cases had a previous exposure to an unidentified infection
age groups younger than 18 years (p<0·0001) and older source, we did a sensitivity analysis using different levels
than 64 years (p<0·0001) increasing from the earlier to of data censoring; the resulting estimates were between
the more recent time periods (appendix p 15). Overall, the 5·0 days (0·8–13·0) and 6·3 days (3·2–10·5; appendix
proportion of cases among individuals younger than p 22).
18 years was low (5%; table 1). The proportion of male cases The transmission dynamics of COVID-19 differed
decreased between the two epidemic periods (p=0·00012), between provinces outside Hubei. Here we report the
but remained around 50% (table 1; appendix p 15). results for a city (Shenzhen—a major city with more
than 12 million inhabitants in Guangdong province) and
two provinces (Hunan and Shandong) for which we
have validated our individual records against the full
Figure 1: Geographical distribution and temporal dynamics of confirmed
COVID-19 cases
official line lists (appendix pp 3–8). Results for the other
(A) Geographical distribution of confirmed COVID-19 cases (including clinically six locations are included in the appendix (p 24).
diagnosed cases for Hubei province), officially reported as of Feb 17, 2020 Although these locations were among those that
(n=72 436), in each province of mainland China (left) and in each city of Hubei reported the largest number of COVID-19 cases as of
province (right). Provinces or cities with a blue contour indicate those selected
for analysis of the net reproduction number. (B) Time series of COVID-19 cases Feb 17, 2020,3 they showed highly different transmission
for which we had individual records in provinces outside Hubei province, divided patterns. Specifically, in Shenzhen, we estimated that
into cases with travel history to Wuhan or Hubei and cases of local transmission. the mean Rt was above the epidemic threshold for about
If no information about the travel history of a patient was reported in the
1 week (approximately from Jan 18 to Jan 23), with a
individual records, we assumed that the patient acquired the infection locally.
This graph refers to 5683 cases with available symptom onset date (out of maximum value of 1·08 (95% CI 0·74–1·54) on Jan 22,
8579 individual cases available in our individual records). The decline in the and the outbreak was mostly sustained by cases with
number of cases in the last few days of February is in part due to the delay travel history to or from Wuhan or Hubei (figure 3). In
between the date of reporting of cases and the date of symptom onset. The first
Hunan province, we estimated the mean Rt to be above
period ran from Dec 24 to Jan 27. Dec 24 is the earliest symptom onset date of
the cases reported outside Hubei. COVID-19=coronavirus disease 2019. the epidemic threshold for about 2 weeks from Jan 13 to
PHEIC=public health emergency of international concern. Jan 28, with a peak value of 1·34 on Jan 20 (1·06–1·68;
www.thelancet.com/infection Vol 20 July 2020 797
Articles
All (n=8579) Period 1 Period 2 Unclassified*
(Dec 24 to Jan 27; n=4210) (Jan 28 to Feb 17; n=2379) (n=1990)
Age, years 44 (33–56) 43 (33–55) 46 (33–58) 44 (31–56)
Age group, years
0–6 124/8579 (1%) 28/4210 (1%) 44/2379 (2%) 52/1990 (3%)
7–17 233/8579 (3%) 65/4210 (2%) 81/2379 (3%) 87/1990 (4%)
18–24 477/8579 (6%) 248/4210 (6%) 106/2379 (4%) 123/1990 (6%)
25–49 4127/8579 (48%) 2147/4210 (51%) 1082/2379 (45%) 898/1990 (45%)
50–64 2113/8579 (25%) 990/4210 (24%) 631/2379 (27%) 492/1990 (25%)
≥65 1002/8579 (12%) 394/4210 (9%) 373/2379 (16%) 235/1990 (12%)
Sex
Female 3943/8579 (46%) 1841/4210 (44%) 1163/2379 (49%) 939/1990 (47%)
Male 4401/8579 (51%) 2258/4210 (54%) 1166/2379 (49%) 977/1990 (49%)
Exposure history
Presence of at least one exposure 6611/8579 (77%)† 3342/4210 (79%) 1708/2379 (72%) 1561/1990 (78%)
Exposure to animals and seafood markets, 34/6611 (1%) 23/3342 (1%) 7/1708 (0%) 4/1561 (0%)
or wild animals
Exposure to COVID-19 cases or patients 2978/6611 (45%) 855/3342 (26%) 1125/1708 (66%) 998/1561 (64%)
with acute respiratory infections
Exposure to Wuhan or Hubei 3672/6611 (56%) 2428/3342 (73%) 591/1708 (35%) 653/1561 (42%)
Residence in Wuhan‡ 1602/3672 (44%) 1135/2428 (47%) 216/591 (37%) 251/653 (38%)
Visited Wuhan 577/3672 (16%) 413/2428 (17%) 96/591 (16%) 68/653 (10%)
Residence in Hubei or visit Hubei§ 519/3672 (14%) 222/2428 (9%) 153/591 (26%) 144/653 (22%)
Data are median (IQR), or n/n (%). Lower denominators indicate missing data, excluded from the analysis. Percentages might not total 100% because of rounding.
COVID-19=coronavirus disease 2019. *We defined two time periods as the symptom onset date; if the date of symptom onset was missing and the date of official reporting,
hospital visit, or outcome was earlier than or equal to Jan 27, 2020, cases were classified into period 1, otherwise, they were unclassified. †77% of records contained specific
information on the exposure. ‡Wuhan residents or individuals who have lived in Wuhan for at least 14 days before symptom onset. §Hubei residents or individuals who
visited Hubei, without specific city where they lived or visited.
Table 1: Characteristics of laboratory-confirmed COVID-19 cases in provinces outside Hubei in mainland China by epidemic period, as of
Feb 17, 2020
All Period 1 (Dec 24 to Jan 27) Period 2 (Jan 28 to Feb 8)* Difference† (95% CI), p value
Time from symptom onset to 2·5 (0·0–10·0), n=2888 3·0 (0·0–11·1), n=1836 1·6 (0·0–7·0), n=1052 1·4 (1·2–1·6), p<0·0001
first health-care consultation, days‡
Time from symptom onset to 3·8 (0·0–12·0), n=2001 4·4 (0·0–14·0), n=1310 2·6 (0·0–9·0), n=691 1·8 (1·5–2·1), p<0·0001
hospital admission, days‡
Time from first health-care 1·5 (0·0–9·0), n=1725§ 1·4 (0·0–9·0); n=850 1·4 (0·0–9·0), n=353 0·0 (0·2–0·4), p=0·6551
consultation to hospital
admission, days‡
Time from symptom onset to official 7·4 (1·0–18·0), n=5024§ 8·9 (2·0–19·8), n=2727 5·4 (1·0–12·0), n=2079 3·5 (3·3–3·7), p<0·0001
reporting, days‡
Data are mean (95% CI), n, unless otherwise specified. *To account for reporting delays, we excluded the last 9 days of data (ie, data after Feb 8, 2020). †Difference between
periods 1 and 2; Welch two-sample t test was used to calculate the p value. ‡Estimated from empirical data through complete-case analysis; the estimates obtained by fitting
gamma, Weibull, and lognormal distributions are reported in the appendix (pp 15–17). §Sample size may be different from the sum of the two periods because it also includes
cases without recorded date of symptom onset, which was used for classification of cases into temporal periods.
Table 2: Key time-to-event intervals for laboratory-confirmed COVID-19 cases by epidemic period, as of Feb 17, 2020
figure 3). Shandong province showed a slightly longer Discussion
epidemic period than Hunan characterised by sustained We have provided an assessment of the rapidly changing
local transmission and a larger peak mean Rt of 1·71 on epidemiology and transmission dynamics of the COVID-19
Jan 23 (1·32–2·17; figure 3). In these three locations, the outbreak beyond Hubei province in mainland China.
mean Rt steadily decreased and has remained below the We found significant differences in the epidemiology of
epidemic threshold since the end of January, 2020. In COVID-19 as the epidemic continued to spread across
general, we found that in all the analysed areas (among China. We estimated that, as of Feb 8, 2020, Rt has been
the most affected provinces outside Hubei), Rt had below the epidemic threshold in the nine locations for
decreased below 1·0 from Feb 8. which we had sufficient data coverage, which were among
798 www.thelancet.com/infection Vol 20 July 2020
Articles
those with the largest number of reported cases (outside
A
Hubei). This finding suggests that China has made key
20 Incubation period
steps towards the interruption of COVID-19 transmission, Serial interval
owing to stringent containment measures, including
isolation of cases, quarantine of contacts, and strict res
15
trictions on personal movement (appendix pp 26–30), as
well as to increased awareness and behavioural change of
Probability (%)
the population.
At the beginning of the epidemic, COVID-19 cases were 10
mostly observed among elderly people.12 As the epidemic
progressed, we observed a further increase in number of
mean 5·1 mean 5·2
cases among people aged 65 years and older, as well as an 5
increase among younger individuals (<18 years). Since
Jan 28, 2020, however, the proportion of confirmed cases
that are in people younger than 18 years is still only about 0
5%, although this age group represents approximately
20% of the Chinese population.13 From the data available B
here, it is not possible to ascertain whether younger 100
individuals have a reduced risk of infection or an increased
propensity for a milder clinical outcome of infection (thus
80
resulting in a lower rate of detection). Schools in China
Cumulative probability (%)
were closed for most of the epidemic because of the 2020
Chinese New Year holidays;14 given studies15 showing that 60
children record the largest number of contacts among
all age groups on a regular weekday due to contacts at
schools, it is possible that children were less exposed than 40
normal during this time. It is unclear whether nationwide
school holidays contributed to the low proportion of con 20
firmed COVID-19 cases among school-age individuals
and whether reopening of schools will lead to a change in
the transmission patterns of COVID-19.16 0
At the beginning of the epidemic, a disproportionate 0 2 4 6 8 10 12 14
Time (days)
fraction of COVID-19 cases were male.12 As of Feb 17, 2020,
however, we observed about the same number of cases Figure 2: Distributions of the incubation period and serial interval
among men and women (51% of cases are male). This (A) Comparison between the best-fitting distributions of the incubation period and of the serial interval;
the vertical dashed lines represent the means of the two distributions. (B) Cumulative density function of the
finding suggests either differential exposure by sex best-fitting distributions of the incubation period and the serial interval.
occurring at the beginning of the epidemic (most cases
reported possible exposure to live markets because they
were shop owners, or worked at or visited the live might not be as high as initial estimates suggest. We
markets17,18) or possible bias in the detection of the first cannot rule out, however, that the serial interval might
few cases. differ between Wuhan and other Chinese provinces.
In provinces outside Hubei, we estimated the mean The short estimate of the serial interval that we obtained
incubation period to be 5·2 days, in agreement with might be linked to the short estimate for the interval
previous studies,5,19–21 although estimates between 4·0 from symptom onset to hospital admission (with a
and 6·7 days have been reported.22,23 The 95th percentile mean of about 2·6 days since Jan 28) for mainland
of the distribution (10·5 days) suggests contact tracing China outside Hubei. A longer admission delay was
and medical observations of contacts of people with reported in Wuhan in the early phase of the outbreak,5
COVID-19 are important to detect individuals with a which could drive longer serial intervals. It should be
long incubation period. In these provinces, the mean stressed also that serial interval estimates based on
serial interval was 5·1 days (95% CI 1·3–11·6). This household clusters might be up to 20% shorter than the
estimate is considerably shorter than a previous true value, as suggested by a theoretical study.10
estimate (7·5 days) derived from an analysis of We estimated that the serial interval was about as long
six observations of the serial interval in Wuhan.5 Given as the incubation period, which is in overall agreement
that the basic reproduction number is positively with an independent previous estimate.5 This finding
associated with the growth rate of the epidemic and the suggests the possibility of an early peak of infectiousness,
length of the serial interval,8 the shorter mean serial with possible transmission of SARS-CoV-2 before the
interval estimated here implies that transmissibility onset of symptoms. If confirmed, the presence of relevant
www.thelancet.com/infection Vol 20 July 2020 799
Articles
Shenzhen (Guangdong province)
A Period 1 Period 2 B Period 1 Period 2
60 3
50 Exposure in Wuhan or Hubei
Number of confirmed cases
Local transmission
(individual records)
40 2
30
Rt
20 1
10
0 0
Hunan province
Period 1 Period 2 Period 1 Period 2
60 3
50
Number of confirmed cases
(individual records)
40 2
30
Rt
20 1
10
0 0
Shandong province
Period 1 Period 2 Period 1 Period 2
60 3
50
Number of confirmed cases
(individual records)
40 2
30
Rt
20 1
10
0 0
24 27 30 02 05 08 11 14 17 20 23 26 29 01 04 07 24 27 30 02 05 08 11 14 17 20 23 26 29 01 04 07
December, 2019 January, 2020 February, 2020 December, 2019 January, 2020 February, 2020
Date of symptom onset Date of symptom onset
Figure 3: Temporal dynamics of Rt in three Chinese locations outside Hubei
Period 1 ran from Dec 24 to Jan 27, and period 2 from Jan 28 to Feb 8. (A) Daily number of new cases in Shenzhen city (Guangdong province), Hunan province, or Shandong province, divided into cases
with travel history to Wuhan or Hubei and cases resulting from local transmission. The insets show maps of China highlighting Hubei province (dark colour) and the analysed location (lighter colour).
(B) Estimated Rt over a 4-day moving average. We excluded the last 9 days of data (ie, data after Feb 8) to account for reporting delays. We estimated the 90th percentile of the distribution of the time
from onset to reporting in mainland China outside Hubei province during period 2 of the epidemic to be 9·0 days. Rt=net reproduction number.
presymptomatic transmission might hamper control appears to be reasonable given the intensity of contact
efforts, including contact tracing and timely isolation of tracing, community transmission cannot be fully ruled
index cases, as well as passenger screening at airports. By out.
contrast, strategies based on social distancing, such as The results presented thus far support a change in
limiting mass gatherings and contact in the workplace epidemiological characteristics of the COVID-19
and in schools, might still be effective.15,24,25 Evidence is outbreak over time and as the epidemic expanded to
accumulating to indicate the possibility of transmission multiple locations. Many of the key epidemiological
during the incubation phase.25–31 It is worth noting also time-delay distributions are different from those
that our estimates of the incubation period and serial reported in studies focusing on the early transmission
interval were based on analysis of cluster data, for which dynamics of COVID-19 in Wuhan.5 This difference is
we assumed that the risk of infection from the community probably the consequence of the increased awareness
was negligible compared with that from infected of the public and physicians, behavioural changes of
individuals in the cluster. Although this assumption the population with respect to respiratory disease
800 www.thelancet.com/infection Vol 20 July 2020
Articles
symptoms, increased health-care readiness, and elev estimate of Rt should be considered an upper bound
ated alert and response across mainland China. (appendix pp 25, 26). This finding lends further support
We estimated that Rt followed different patterns across to our conclusion that Rt has been decreasing since the
China. We found that the epidemic was self-sustained for end of January.
short periods of time only (no more than 3 weeks) in Despite these limitations, a real-time updated patient
provinces outside Hubei that reported a large number of line list such as the one we have compiled is crucial to
cases,32 and estimated that, since the end of January, 2020, assess the epidemiology and transmission dynamics of an
Rt has been below the epidemic threshold in all studied emerging pathogen, inform situational awareness, and
provinces. This finding is consistent with the gradual optimise responses to the outbreak. Since Jan 20, 2020,
decrease in the number of detected COVID-19 cases the National Health Commission of China has incor
reported across China and suggests a beneficial effect of porated COVID-19 as a notifiable disease.35 The Chinese
the strict public health intervention policies implemented Government has committed to timely disclosure of
in China. In particular, strict social-distancing measures COVID-19 information, a decision highly praised by
were implemented in all the analysed Chinese provinces WHO.36 Accordingly, the local health commissions and
and included close community management (eg, case the official data sources, from which our individual
isolation and household quarantine of close contacts), data originate, were authorised to release real-time
suspension of public activities, traffic restrictions, and information about epidemiological investigations on
school closure. A full list and timeline of the implemented COVID-19 cases. The data collected for this analysis
interventions in each of the analysed locations is reported represent a valuable source of information and highlight
in the appendix (26–30). It should be stressed that the importance of publicly available records.
the effectiveness of containment measures only applies In conclusion, our study provides a detailed overview of
while they are in place, and a relaxation of public health the changing epidemiology and transmission dynamics
interventions or a substantial change in human behaviour of COVID-19 in mainland China outside Hubei province.
might lead to a subsequent increase in transmission. Our findings suggest a slowing down of the COVID-19
Furthermore, our findings are based on analysis of outbreak in mainland China (outside Hubei province),
nine of the most affected provinces in mainland indicating that the initial steps taken towards interruption
China outside Hubei. Therefore, although unlikely, it is of COVID-19 transmission might have been effective.
possible that other provinces reporting only a few However, the epidemic is not yet under control, and a
cases could still have self-sustained outbreaks. Finally, large proportion of the population is still susceptible. The
the contribution of asymptomatic and presymptomatic trajectory of the outbreak in China and beyond will
infections to COVID-19 transmission remains unclear, as depend on the effectiveness of control policies and
does the amount of asymptomatic or presymptomatic human behaviour in the coming months.
transmission captured in existing datasets.28–31,33,34 Contributors
This study is prone to the usual limitations pertaining MA and HY designed the experiments. JZ, WW, YW, XD, XingC, MeL,
to analysis of rapidly evolving infectious disease out WZ, XW, LY, XinhC, QW, and YL collected data. JZ, MaL, WW, YW, XD,
and MA analysed data. JZ, MaL, WW, JY, KS, IML, MEH, PW, BJC, SM,
breaks, including biases due to case ascertainment, non- CV, AV, MA, and HY interpreted the results. MA and HY wrote the Article.
homogeneous sampling over time and by location, as JZ, MaL, XW, JY, MEH, PW, BJC, CV, and AV edited and revised the
well as hidden and unmodelled correlations. Thus, the Article.
uncertainty might be larger than estimated. Our Declaration of interests
estimates of Rt are most robust, when assuming that BJC has received honoraria from Roche and Sanofi Pasteur. AV has
under-reporting and the frequency of asymptomatic or received funding from Metabiota. HY has received research funding
from Sanofi Pasteur, GlaxoSmithKline, Yichang HEC Changjiang
presymptomatic transmission remain constant. Our Pharmaceutical Company, and Shanghai Roche Pharmaceutical
estimates, however, are sensitive to marked changes in Company. All other authors declare no competing interests.
reporting rates and in the proportion of SARS-CoV-2 Data sharing
infections that lead to clinically identifiable symptoms. The individual line list analysed in this study is available online. For the individual line list see
Individual records were retrieved from different data https://github.com/Juan-ZJ/
Acknowledgments COVID-19-line-list
sources and thus might be affected by geographical We thank Wenkai Yang, Jingyuan Feng, Jialu Cheng, Qiuyi Xu,
differences in sampling of cases with specific exposures Haixin Ju, Xufang Bai, Zi Yu, Yumin Zhang, Wei Guo, Zeyao Zhao,
Xin Chen, Sihong Zhao, Rong Du, Jiaxian Chen, Jiangnan Li,
(eg, imported or locally acquired infections) and available
Geshu Zhang, Hong Peng, Xin Shen, Zeyu Li, and Yuheng Feng from
dates of symptom onset. However, we compared our data Fudan University (Shanghai, China) for assisting with data collection.
for Shenzhen city, Hunan province, and Shandong We thank Nicole Samay for her assistance in preparing the figures.
province with official line lists and found the datasets to HY acknowledges financial support from the National Science Fund
for Distinguished Young Scholars (number 81525023), Key Emergency
be of similar quality. It should also be stressed that the
Project of Shanghai Science and Technology Committee (number
case definition has been changed several times since the 20411950100), and the National Science and Technology Major Project
start of the epidemic, and in particular, it was broadened of China (numbers 2018ZX10201001–010, 2018ZX10713001–007, and
on Jan 27. Therefore, because potentially more cases were 2017ZX10103009–005). MEH acknowledges financial support from the
National Institute of General Medical Sciences (U54-GM111274).
identified since this change in case definition, our
www.thelancet.com/infection Vol 20 July 2020 801
Articles
SM and MA acknowledge financial support from the European 19 Backer JA, Klinkenberg D, Wallinga J. Incubation period of 2019
Commission Horizon 2020 MOOD project. novel coronavirus (2019-nCoV) infections among travellers from
Wuhan, China, 20–28 January 2020. Euro Surveill 2020; published
Editorial note: the Lancet Group takes a neutral position with respect to online Feb 6. DOI:10.2807/1560-7917.ES.2020.25.5.2000062.
territorial claims in published maps and institutional affiliations. 20 Linton NM, Kobayashi T, Yang Y, et al. Incubation period and other
References epidemiological characteristics of 2019 novel coronavirus infections
1 Chinese Center for Disease Control and Prevention. Epidemic with right truncation: a statistical analysis of publicly available case
update and risk assessment of 2019 novel coronavirus 2020. 2020. data. J Clin Med 2020; 9: e538.
http://www.chinacdc.cn/yyrdgz/202001/P020200128523354919292. 21 Lauer SA, Grantz KH, Bi Q, et al. The Incubation period of
pdf (accessed Feb 18, 2020). coronavirus disease 2019 (COVID-19) from publicly reported
2 National Health Commission of the People’s Republic of China. confirmed cases: estimation and application. Ann Intern Med 2020;
Update on COVID-19 as of 24:00 on March 10, 2020. 2020. published online March 10. DOI:10.7326/M20-0504.
http://www.nhc.gov.cn/xcs/yqfkdt/202003/b4abcf83e 22 Guan WJ, Ni ZY, Hu Y, et al. Clinical characteristics of coronavirus
53d4284b2981c75917385eb.shtml (accessed March 11, 2020). disease 2019 in China. N Engl J Med 2020; published online Feb 28.
3 World Health Organization. Coronavirus disease 2019 (COVID-19) DOI:10.1056/NEJMoa2002032.
situation report–47. 2020. https://www.who.int/docs/default-source/ 23 Tian S, Hu N, Lou J, et al. Characteristics of COVID-19 infection in
coronaviruse/situation-reports/20200307-sitrep-47-covid-19. Beijing. J Infect 2020; published online Feb 27.
pdf?sfvrsn=27c364a4_2 (accessed March 8, 2020). DOI:10.1016/j.jinf.2020.02.018.
4 World Health Organization. Statement on the second meeting of 24 Cowling BJ, Lau EHY, Lam CLH, et al. Effects of school closures,
the International Health Regulations (2005) Emergency Committee 2008 winter influenza season, Hong Kong. Emerg Infect Dis 2008;
regarding the outbreak of novel coronavirus (2019-nCoV). 2020. 14: 1660–62.
https://www.who.int/news-room/detail/30-01-2020-statement-on- 25 Ministry of Culture and Tourism of the People’s Republic of China.
the-second-meeting-of-the-international-health-regulations-(2005)- Notice on extending the spring festival holiday of 2020. 2020.
emergency-committee-regarding-the-outbreak-of-novel-coronavirus- https://www.mct.gov.cn/whzx/whyw/202001/t20200127_850576.
(2019-ncov) (accessed Feb 18, 2020). htm (accessed March 11, 2020).
5 Li Q, Guan X, Wu P, et al. Early transmission dynamics in Wuhan, 26 Yu P, Zhu J, Zhang Z, Han Y, Huang L. A familial cluster of
China, of novel coronavirus-infected pneumonia. N Engl J Med infection associated with the 2019 novel coronavirus indicating
2020; published online Jan 29. DOI:10.1056/NEJMoa2001316. potential person-to-person transmission during the incubation
6 The Novel Coronavirus Pneumonia Emergency Response period. J Infect Dis 2020; published online Feb 18.
Epidemiology Team. The epidemiological characteristics of an DOI:10.1093/infdis/jiaa077.
outbreak of 2019 novel coronavirus diseases (COVID-19)—China, 27 Zou L, Ruan F, Huang M, et al. SARS-CoV-2 viral load in upper
2020. China CDC Weekly 2020; 2: 145–51. respiratory specimens of infected patients. N Engl J Med 2020;
7 National Health Commission of the People’s Republic of China. published online Feb 19. DOI:10.1056/NEJMc2001737.
Diagnosis and treatment guideline on pneumonia infection with 28 Zhao S, Gao D, Zhuang Z, et al. Estimating the serial interval of the
2019 novel coronavirus (5th trial edn). 2020 http://www.nhc.gov.cn/ novel coronavirus disease (COVID-19): a statistical analysis using
xcs/zhengcwj/202002/d4b895337e19445f8d728fcaf1e3e13a.shtml the public data in Hong Kong from January 16 to February 15, 2020.
(accessed Feb 18, 2020). medRχiv 2020: published online Feb 21.
8 Wallinga J, Lipsitch M. How generation intervals shape the DOI:10.1101/2020.02.21.20026559 (preprint).
relationship between growth rates and reproductive numbers. 29 Tong ZD, Tang A, Li KF, et al. Potential presymptomatic
Proc Biol Sci 2007; 274: 599–604. transmission of SARS-CoV-2, Zhejiang Province, China, 2020.
9 World Health Organization Ebola Response Team, Aylward B, Emerg Infect Dis 2020; 26: published online May 17.
Barboza P, et al. Ebola virus disease in West Africa—the first DOI:10.3201/eid2605.200198.
9 months of the epidemic and forward projections. N Engl J Med 30 Du Z, Xu X, Wu Y, Wang L, Cowling BJ, Meyers LA. The serial
2014; 371: 1481–95. interval of COVID-19 from publicly reported confirmed cases.
10 Liu QH, Ajelli M, Aleta A, Merler S, Moreno Y, Vespignani A. medRχiv 2020; published online March 13.
Measurability of the epidemic reproduction number in data-driven DOI:10.1101/2020.02.19.20025452 (preprint).
contact networks. Proc Natl Acad Sci USA 2018; 115: 12680–85. 31 Tindale L, Coombe M, Stockdale JE, et al. Transmission interval
11 Thompson RN, Stockwin JE, van Gaalen RD, et al. Improved estimates suggest pre-symptomatic spread of COVID-19. medRiv
inference of time-varying reproduction numbers during infectious 2020; published online March 6. DOI:10.1101/2020.03.03.20029983
disease outbreaks. Epidemics 2019; 29: 100356. (preprint).
12 Chen N, Zhou M, Dong X, et al. Epidemiological and clinical 32 Kucharski AJ, Russell TW, Diamond C, et al. Early dynamics of
characteristics of 99 cases of 2019 novel coronavirus pneumonia in transmission and control of COVID-19: a mathematical modelling
Wuhan, China: a descriptive study. Lancet 2020; 395: 507–13. study. Lancet Infect Dis 2020; published online March 11.
13 National Bureau of Statistics. China census in 2018. 2020. https://doi.org/10.1016/S1473-3099(20)30144-4.
http://www.stats.gov.cn/tjsj/ndsj/2019/indexch.htm (accessed 33 Mizumoto K, Kagaya K, Zarebski A, Chowell G. Estimating the
Feb 10, 2020). asymptomatic proportion of 2019 novel coronavirus onboard the
14 Ministry of Education of the People’s Republic of China. Princess Cruises ship, 2020. medRχiv 2020; published online
Notice on the postponement of the spring semester of 2020. 2020. March 6: DOI:10.1101/2020.02.20.20025866 (preprint).
http://www.moe.gov.cn/jyb_xwfb/gzdt_gzdt/s5987/202001/ 34 Bai Y, Yao L, Wei T, et al. Presumed asymptomatic carrier
t20200127_416672.html (accessed March 11, 2020). transmission of COVID-19. JAMA 2020; published online Feb 21.
15 Litvinova M, Liu QH, Kulikov ES, Ajelli M. Reactive school closure DOI:10.1001/jama.2020.2565.
weakens the network of social interactions and reduces the spread 35 National Health Commission of the People’s Republic of China.
of influenza. Proc Natl Acad Sci USA 2019; 116: 13174–81. Inclusion of 2019 novel coronavirus diseases (COVID-19) into
16 Zhang J, Litvinova M, Liang Y, et al. Age profile of susceptibility, statutory infectious disease management. 2020. http://www.nhc.
mixing, and social distancing shape the dynamics of the novel gov.cn/jkj/s7916/202001/44a3b8245e8049d2837a4f27529cd386.shtml
coronavirus disease 2019 outbreak in China. medRχiv 2020: (accessed Feb 18 2020).
published online March 20. DOI:10.1101/2020.03.19.20039107 36 McNeice A. WHO chief praises containment efforts. 2020
(preprint). http://www.chinadaily.com.cn/a/202001/31/
17 Huang C, Wang Y, Li X, et al. Clinical features of patients infected WS5e3335fba310128217273bff.html (accessed Feb 18 2020).
with 2019 novel coronavirus in Wuhan, China. Lancet 2020;
395: 497–506.
18 Wu P, Hao X, Lau EHY, et al. Real-time tentative assessment of the
epidemiological characteristics of novel coronavirus infections in
Wuhan, China, as at 22 January 2020. Euro Surveill 2020; 25: 2000044.
802 www.thelancet.com/infection Vol 20 July 2020
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Thermo PartDocument52 pagesThermo PartAmar kumarNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- EGU24 11940 PrintDocument1 pageEGU24 11940 PrintDe Nicolas JaidarNo ratings yet
- mathcal (PT) $-Symmetric Tight-Binding Chain With Gain and Loss: A Completely Solvable ModelDocument24 pagesmathcal (PT) $-Symmetric Tight-Binding Chain With Gain and Loss: A Completely Solvable ModelDe Nicolas JaidarNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Modeling Magnetohydrodynamic Turbulence by Low-Dimensional Dynamical SystemsDocument45 pagesModeling Magnetohydrodynamic Turbulence by Low-Dimensional Dynamical SystemsDe Nicolas JaidarNo ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Entrainment Instability Quasi PeriodicitDocument17 pagesEntrainment Instability Quasi PeriodicitDe Nicolas JaidarNo ratings yet
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Electricalcouple EarthcuakeDocument9 pagesElectricalcouple EarthcuakeDe Nicolas JaidarNo ratings yet
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Physics 111: Mechanics: Dale GaryDocument28 pagesPhysics 111: Mechanics: Dale GaryavgNo ratings yet
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Andre Barato-HoustonDocument5 pagesAndre Barato-HoustonDe Nicolas JaidarNo ratings yet
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Fundamental Laws and Rules in Thermodynamics: Name Closed Systems Open SystemsDocument3 pagesFundamental Laws and Rules in Thermodynamics: Name Closed Systems Open SystemsDe Nicolas JaidarNo ratings yet
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Electricalcouple EarthcuakeDocument9 pagesElectricalcouple EarthcuakeDe Nicolas JaidarNo ratings yet
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- A Dynamical Systems Approach To The Control of Chaotic Dynamics in A Spatiotemporal Jet OwDocument13 pagesA Dynamical Systems Approach To The Control of Chaotic Dynamics in A Spatiotemporal Jet OwDe Nicolas JaidarNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Cambridge-Martin J. ReesDocument7 pagesCambridge-Martin J. ReesDe Nicolas JaidarNo ratings yet
- Modeling Magnetohydrodynamic Turbulence by Low-Dimensional Dynamical SystemsDocument45 pagesModeling Magnetohydrodynamic Turbulence by Low-Dimensional Dynamical SystemsDe Nicolas JaidarNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- EarthquakeDocument12 pagesEarthquakeDe Nicolas JaidarNo ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Hramov Etal PRE71 05Document9 pagesHramov Etal PRE71 05De Nicolas JaidarNo ratings yet
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- ProblemasDocument1 pageProblemasDe Nicolas JaidarNo ratings yet
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Icarus: Research PaperDocument15 pagesIcarus: Research PaperDe Nicolas JaidarNo ratings yet
- Vespignani CovidDocument10 pagesVespignani CovidDe Nicolas JaidarNo ratings yet
- Photoabsorption of Carbon Monoxide: A Time-Dependent Quantum Mechanical StudyDocument10 pagesPhotoabsorption of Carbon Monoxide: A Time-Dependent Quantum Mechanical StudyDe Nicolas JaidarNo ratings yet
- The Pirouette Effect in Turbulent Ows: Nature Physics June 2011Document5 pagesThe Pirouette Effect in Turbulent Ows: Nature Physics June 2011De Nicolas JaidarNo ratings yet
- Río 2018 J. Phys. Commun. 2 055006Document14 pagesRío 2018 J. Phys. Commun. 2 055006De Nicolas JaidarNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- External SignalDocument11 pagesExternal SignalDe Nicolas JaidarNo ratings yet
- Monica de La Cruz - SarscovDocument8 pagesMonica de La Cruz - SarscovDe Nicolas JaidarNo ratings yet
- Oscillatory Activity Regulation in An Ensemble of Autonomous Mercury Beating Heart OscillatorsDocument7 pagesOscillatory Activity Regulation in An Ensemble of Autonomous Mercury Beating Heart OscillatorsDe Nicolas JaidarNo ratings yet
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- T2 6cDocument1 pageT2 6cDe Nicolas JaidarNo ratings yet
- T2 6aDocument1 pageT2 6aDe Nicolas JaidarNo ratings yet
- Inst. Ampl. PhaseDocument11 pagesInst. Ampl. PhaseDe Nicolas JaidarNo ratings yet
- MITRES 6 007S11 Lec09Document12 pagesMITRES 6 007S11 Lec09Megha PanchariyaNo ratings yet
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (120)
- Rosenblum Etal PRL76 96 PDFDocument4 pagesRosenblum Etal PRL76 96 PDFDe Nicolas JaidarNo ratings yet
- Case Study.... Group-BDocument33 pagesCase Study.... Group-BNazmul HossainNo ratings yet
- BSN 3-B (GROUP 2) - CLINICAL CASE ANALYSIS - Arthritis (REVISED)Document7 pagesBSN 3-B (GROUP 2) - CLINICAL CASE ANALYSIS - Arthritis (REVISED)Florence Dumawal FariñasNo ratings yet
- Hon 2005Document5 pagesHon 2005lenirizkiNo ratings yet
- Important Causes of Sudden Cardiac DeathDocument2 pagesImportant Causes of Sudden Cardiac DeathTausif AbbasNo ratings yet
- The Effect of Mangosteen (Garcinia Mangostana) Rind in The Blood Glucose Levels of Adult Patients With Type 2 Diabetes MellitusDocument4 pagesThe Effect of Mangosteen (Garcinia Mangostana) Rind in The Blood Glucose Levels of Adult Patients With Type 2 Diabetes MellitusFiqoh Puteri FauziNo ratings yet
- Derek C Angus Caring For Patients With AcuteDocument4 pagesDerek C Angus Caring For Patients With AcuteAnanth BalakrishnanNo ratings yet
- Fees and Charges - Summary From 1 July 2020 Version 1.0, June 2020Document51 pagesFees and Charges - Summary From 1 July 2020 Version 1.0, June 2020QualityMattersNo ratings yet
- Diagnosis and Management of Fetal Mummification in CowDocument5 pagesDiagnosis and Management of Fetal Mummification in CowAbdul Wahab Assya RoniNo ratings yet
- 83 Nutripuncture OverviewDocument12 pages83 Nutripuncture OverviewTimoteo Pereira TfmpNo ratings yet
- NCP EsrdDocument9 pagesNCP EsrdMarisol Dizon100% (1)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Pre Op NCPDocument1 pagePre Op NCPJoshua Kelly0% (2)
- Case Study Formate MSNDocument2 pagesCase Study Formate MSNLijoNo ratings yet
- Consent To Surgery/Anaesthesia: Ilocos Sur Provincial Hospital-Gabriela SilangDocument1 pageConsent To Surgery/Anaesthesia: Ilocos Sur Provincial Hospital-Gabriela SilangRyrey Abraham PacamanaNo ratings yet
- Danish Mask StudyDocument1 pageDanish Mask StudyJuana AtkinsNo ratings yet
- When Are Focused Assessments ConductedDocument26 pagesWhen Are Focused Assessments ConductedNozomi YukiNo ratings yet
- Objectives For Critical Care RotationDocument9 pagesObjectives For Critical Care Rotationsteviestevie333No ratings yet
- Referral LetterDocument3 pagesReferral LetterMa. Thea Diane BillonesNo ratings yet
- Global Idiopathic Pulmonary Fibrosis Treatment MarketDocument3 pagesGlobal Idiopathic Pulmonary Fibrosis Treatment MarketiHealthcareAnalyst, Inc.No ratings yet
- Konsensus IBDDocument15 pagesKonsensus IBDTaufikNo ratings yet
- Continue Renal Replacement Therapy: 1. CVVH 2. CVVHD 3. CVVHDFDocument21 pagesContinue Renal Replacement Therapy: 1. CVVH 2. CVVHD 3. CVVHDFhengki jokteryNo ratings yet
- Heroine Source: by Waqas, Email 21waqas@stu - Edu.cnDocument14 pagesHeroine Source: by Waqas, Email 21waqas@stu - Edu.cnwaqasNo ratings yet
- 3f - 1 (Division of Task)Document33 pages3f - 1 (Division of Task)Trisha ArtosNo ratings yet
- Literature ReviewDocument3 pagesLiterature Reviewapi-609233193No ratings yet
- Testicular CancerDocument24 pagesTesticular CancerJulianne LeeNo ratings yet
- CotrimoxazoleDocument3 pagesCotrimoxazolecsy123No ratings yet
- The Following Resources Related To This Article Are Available Online atDocument8 pagesThe Following Resources Related To This Article Are Available Online atFerdina NidyasariNo ratings yet
- Diabetic Ketoacidosis - WikipediaDocument32 pagesDiabetic Ketoacidosis - WikipediaSanket TelangNo ratings yet
- Dip HIV Man (SA) Regulations 24-1-2017Document9 pagesDip HIV Man (SA) Regulations 24-1-2017matentenNo ratings yet
- News Story 3Document2 pagesNews Story 3api-558280939No ratings yet