You might also like
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (844)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5814)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- (Ebook - PDF - Semiotics) - Ultimate Neuro-Linguistic Programming (NLP)Document169 pages(Ebook - PDF - Semiotics) - Ultimate Neuro-Linguistic Programming (NLP)ior2101100% (1)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- 2019 Fall Expo Contact List PDFDocument10 pages2019 Fall Expo Contact List PDFSoji AdimulaNo ratings yet
- University Physics Volume 2 Derived Copy For Ysc1213 1.75Document441 pagesUniversity Physics Volume 2 Derived Copy For Ysc1213 1.75Soji AdimulaNo ratings yet
- SAS LAS4 Toxicology Lab Activity Sheet No. 4Document8 pagesSAS LAS4 Toxicology Lab Activity Sheet No. 4Jackielou MaquisoNo ratings yet
- CHAPTER 8 MedtechDocument17 pagesCHAPTER 8 MedtechKisen DiazNo ratings yet
- Gauss Law ReviewDocument61 pagesGauss Law ReviewSoji AdimulaNo ratings yet
- Son of South Korean Immigrants, Bucks County's Andrew Heo Carries Family's Olympic Dream To BeijingDocument8 pagesSon of South Korean Immigrants, Bucks County's Andrew Heo Carries Family's Olympic Dream To BeijingSoji AdimulaNo ratings yet
- Chapter 11Document12 pagesChapter 11Soji AdimulaNo ratings yet
- Tree Care Industry MagazineDocument44 pagesTree Care Industry MagazineSoji AdimulaNo ratings yet
- DiagramsDocument62 pagesDiagramsSoji AdimulaNo ratings yet
- Sun Hasn't Set On Sunrise Packaging - Minneapolis - St. Paul Business JournalDocument4 pagesSun Hasn't Set On Sunrise Packaging - Minneapolis - St. Paul Business JournalSoji AdimulaNo ratings yet
- Molecular Orbitals and Curved ArrowsDocument51 pagesMolecular Orbitals and Curved ArrowsSoji AdimulaNo ratings yet
- Bio-Med 350: Normal Heart Function and Congestive Heart FailureDocument59 pagesBio-Med 350: Normal Heart Function and Congestive Heart FailureSoji AdimulaNo ratings yet
- Chem 14CL - Lecture 1 - Amino - AcidDocument17 pagesChem 14CL - Lecture 1 - Amino - AcidSoji AdimulaNo ratings yet
- RC Circuits: Instructor: Kazumi TolichDocument11 pagesRC Circuits: Instructor: Kazumi TolichSoji AdimulaNo ratings yet
- Faculty Version With Model Answers: Body FluidsDocument10 pagesFaculty Version With Model Answers: Body FluidsSoji AdimulaNo ratings yet
- What Is An Argument?: ConclusionDocument25 pagesWhat Is An Argument?: ConclusionSoji AdimulaNo ratings yet
- Periodic Properties of The Elements: Theodore L. Brown H. Eugene Lemay, Jr. and Bruce E. BurstenDocument82 pagesPeriodic Properties of The Elements: Theodore L. Brown H. Eugene Lemay, Jr. and Bruce E. BurstenSoji AdimulaNo ratings yet
- Inflammation and Repair: Definition of Inflammation Acute Inflammation Vascular Events in InflammationDocument35 pagesInflammation and Repair: Definition of Inflammation Acute Inflammation Vascular Events in InflammationSoji AdimulaNo ratings yet
- Happy Labor Day: Tuesday, September 8, 2020Document1 pageHappy Labor Day: Tuesday, September 8, 2020Soji AdimulaNo ratings yet
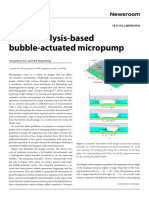
- An Electrolysis-Based Bubble-Actuated Micropump: Cheng-Hsien Liu and Chih Ming ChengDocument3 pagesAn Electrolysis-Based Bubble-Actuated Micropump: Cheng-Hsien Liu and Chih Ming ChengSoji AdimulaNo ratings yet
- Interleukin 6 in Exhaustive Exercises and Its Correlation To Bacteremia A Pilot StudyDocument9 pagesInterleukin 6 in Exhaustive Exercises and Its Correlation To Bacteremia A Pilot StudyAbdullah ElgeddawyNo ratings yet
- Flashcards - Topic 13 Excretion in Humans - CAIE Biology IGCSEDocument35 pagesFlashcards - Topic 13 Excretion in Humans - CAIE Biology IGCSEAleeza FatimaNo ratings yet
- Acid Base Disorder ABG AnalysisDocument53 pagesAcid Base Disorder ABG AnalysisAlemayehu beharuNo ratings yet
- Formation of Concentrated UrineDocument15 pagesFormation of Concentrated UrineNazia WasimNo ratings yet
- Allen: Final Neet (Ug) - 2021 ExaminationDocument6 pagesAllen: Final Neet (Ug) - 2021 ExaminationShahidNo ratings yet
- Applications of Tissue Engineering: Presented by Asmita Benichatage MBT-09039Document27 pagesApplications of Tissue Engineering: Presented by Asmita Benichatage MBT-09039asmita_8588No ratings yet
- HumanBiology May:June 2016 Paper1Document28 pagesHumanBiology May:June 2016 Paper1WendyNo ratings yet
- Balanced Salt SolutionDocument36 pagesBalanced Salt Solutionnaili nsnNo ratings yet
- Liver HealthDocument9 pagesLiver HealthperdidalmaNo ratings yet
- Magnetic Resonance Imaging Versus Serum Iron Status As Diagnostic Tools For Pituitary Iron Overload in Children With Beta ThalassemiaDocument13 pagesMagnetic Resonance Imaging Versus Serum Iron Status As Diagnostic Tools For Pituitary Iron Overload in Children With Beta ThalassemiaAbdurrahman HasanuddinNo ratings yet
- The Color Purple Essay TopicsDocument5 pagesThe Color Purple Essay Topicsfz75yesw100% (2)
- Dubai Seafex 2013 Fuari TalepleriDocument10 pagesDubai Seafex 2013 Fuari Talepleritapioca leNo ratings yet
- Test Bank For Body Structures and Functions 12th Edition ScottDocument9 pagesTest Bank For Body Structures and Functions 12th Edition ScottTonyRamosgbspc100% (32)
- Medicine Admitting Conference: University of Santo Tomas Faculty of Medicine and SurgeryDocument70 pagesMedicine Admitting Conference: University of Santo Tomas Faculty of Medicine and SurgerySTEPHANIE TANNo ratings yet
- Neuromuscular Facilitation Techniques: Miss Rojaramani Vasamshetty MPT Ii YrDocument24 pagesNeuromuscular Facilitation Techniques: Miss Rojaramani Vasamshetty MPT Ii YrdeepuphysioNo ratings yet
- Collegedekho 240507 180322Document8 pagesCollegedekho 240507 180322Tanmay singhNo ratings yet
- Kerja Kursus Biologi 1Document10 pagesKerja Kursus Biologi 1Teo Hui pingNo ratings yet
- Session #10 SAS - AnaPhy (Lab)Document4 pagesSession #10 SAS - AnaPhy (Lab)G INo ratings yet
- REFERAT OA OSTEO-SILVIA EMY 2017730112 (Autosaved)Document29 pagesREFERAT OA OSTEO-SILVIA EMY 2017730112 (Autosaved)Ufaira Nadila ArdiNo ratings yet
- Protozoa Darah (Malaria) : Dr. Dwi Handayani, Mkes Staf Bagian Parasitologi Fakultas Kedokteran UnsriDocument88 pagesProtozoa Darah (Malaria) : Dr. Dwi Handayani, Mkes Staf Bagian Parasitologi Fakultas Kedokteran UnsriGladis Aprilla RizkiNo ratings yet
- Full Download Test Bank For Histology and Cell Biology 2nd Edition Abraham L Kierszenbaum PDF Full ChapterDocument36 pagesFull Download Test Bank For Histology and Cell Biology 2nd Edition Abraham L Kierszenbaum PDF Full Chapteramandablevinsqakymroeiw100% (16)
- PHYSIO Revised + Extra QsDocument68 pagesPHYSIO Revised + Extra Qsdoaa naieemNo ratings yet
- 1 Biology For EngineersDocument24 pages1 Biology For EngineersDipak RajbharNo ratings yet
- 8 2 (A) Define The Term Excretion.: For Examiner's UseDocument2 pages8 2 (A) Define The Term Excretion.: For Examiner's UseMikiko Fujiwara SamaNo ratings yet
- Cap. 01 - Amphibian Anatomy and PhysiologyDocument12 pagesCap. 01 - Amphibian Anatomy and PhysiologyNailson JúniorNo ratings yet
- Icu ScoringDocument7 pagesIcu ScoringLizaNo ratings yet
- Exercise 2. Prokaryotic Algae: BOTANY3 Laboratory Hand-OutDocument3 pagesExercise 2. Prokaryotic Algae: BOTANY3 Laboratory Hand-OutAnna HarietNo ratings yet