You might also like
- Nursing Theories and ConceptsDocument6 pagesNursing Theories and ConceptsAinah Batua-anNo ratings yet
- Models of Health and WellnessDocument5 pagesModels of Health and WellnessGlory GloryNo ratings yet
- Test Your Nursing Knowledge: CA1 Module 3 ActivitiesDocument6 pagesTest Your Nursing Knowledge: CA1 Module 3 ActivitiesEsmareldah Henry SirueNo ratings yet
- Patient Positioning: Complete Guide For MidwivesDocument12 pagesPatient Positioning: Complete Guide For MidwivesRohlen BaguioNo ratings yet
- Fundamentals of Nursing (Midterm Topic 2)Document7 pagesFundamentals of Nursing (Midterm Topic 2)Manuel, Precious Marie B.No ratings yet
- Monitoring An IV Site and InfusionDocument4 pagesMonitoring An IV Site and InfusionAlex Cacayan CortinaNo ratings yet
- Assessment Tools and EquipmentsDocument32 pagesAssessment Tools and EquipmentsMingNo ratings yet
- Compilation of Reviewer For Fundamentals of Nursing PDF FreeDocument49 pagesCompilation of Reviewer For Fundamentals of Nursing PDF FreeTyler VintNo ratings yet
- Shampooing Hair in Bed Procedure ChecklistDocument2 pagesShampooing Hair in Bed Procedure ChecklistMarku LeeNo ratings yet
- Female Catheterization ProcedureDocument3 pagesFemale Catheterization ProcedureMacy Marquez100% (1)
- September 13 - NCM 112 (Mam G)Document2 pagesSeptember 13 - NCM 112 (Mam G)Aaron DayloNo ratings yet
- Filipino Culture, Values and Practices in Relation To Health Care of Individual and FamilyDocument15 pagesFilipino Culture, Values and Practices in Relation To Health Care of Individual and Familyfatima dasalNo ratings yet
- Chapter 24: Communication Communication and Nursing PracticeDocument4 pagesChapter 24: Communication Communication and Nursing PracticejoanneNo ratings yet
- TFN Prelim For PrintingDocument14 pagesTFN Prelim For PrintingjuNo ratings yet
- Pulse Oximetry and The Oxyhemoglobin Dissociation Curve: I. II. Iii. IV. A. B. C. D. V. VI. Vii. A. B. C. D. Viii. IX. XDocument11 pagesPulse Oximetry and The Oxyhemoglobin Dissociation Curve: I. II. Iii. IV. A. B. C. D. V. VI. Vii. A. B. C. D. Viii. IX. XDarryl Betts50% (2)
- Nursing As A ProfessionDocument6 pagesNursing As A Professionreyl MercadejasNo ratings yet
- CHN NotesDocument7 pagesCHN NotesAnvi Turingan PedronanNo ratings yet
- #1 - 1st Day NCM 01 - Lec - Reviewer PrelimDocument14 pages#1 - 1st Day NCM 01 - Lec - Reviewer PrelimNurse TinNo ratings yet
- Assessing Heart and Central VesselsDocument34 pagesAssessing Heart and Central VesselsGemmalene Pacleb100% (1)
- Health, Wellness and IllnessDocument4 pagesHealth, Wellness and Illnessmbx47No ratings yet
- Case Analysis RLE MODULE TEMPLATE Nursery 1 (One)Document7 pagesCase Analysis RLE MODULE TEMPLATE Nursery 1 (One)PanJan BalNo ratings yet
- SuctioningDocument30 pagesSuctioningbajaoc60% (5)
- #3 - 2nd Day NCM 01 - Lab - Reviewer PrelimDocument20 pages#3 - 2nd Day NCM 01 - Lab - Reviewer PrelimNurse TinNo ratings yet
- FUNDA Lab 11 Oxygen Therapy Suctioning Procedures23Document38 pagesFUNDA Lab 11 Oxygen Therapy Suctioning Procedures23loijhonmuchillasNo ratings yet
- Oxygen Therapy AdministrationDocument15 pagesOxygen Therapy AdministrationMike Faustino Solangon100% (1)
- Procedure Checklist Chapter 23: Using A Volume-Control Administration Set (E.g., Buretrol, Volutrol, Soluset)Document2 pagesProcedure Checklist Chapter 23: Using A Volume-Control Administration Set (E.g., Buretrol, Volutrol, Soluset)jthsNo ratings yet
- Administering Oral MedicationsDocument5 pagesAdministering Oral MedicationsAda Gay Olandia SerencioNo ratings yet
- Skill Performance Evaluation - Measuring Intake and OutputDocument2 pagesSkill Performance Evaluation - Measuring Intake and OutputLemuel Que100% (1)
- PDF NCM 103 Lecture NotesDocument5 pagesPDF NCM 103 Lecture Notesyoshi kento100% (2)
- Foley Catheter Insertion ProcedureDocument6 pagesFoley Catheter Insertion ProcedureJustine VillaflorNo ratings yet
- Principles of Sterile Technique: Them That Varies. These Principles Are Applied in TheDocument22 pagesPrinciples of Sterile Technique: Them That Varies. These Principles Are Applied in Thecoosa liquorsNo ratings yet
- At LTC N Theories Models 1Document35 pagesAt LTC N Theories Models 1Darin BransonNo ratings yet
- Heart and Neck VesselsDocument3 pagesHeart and Neck VesselsMark ElbenNo ratings yet
- Ambulating A PatientDocument5 pagesAmbulating A PatientSushmaNo ratings yet
- ICU NCP AirwayDocument3 pagesICU NCP AirwayLisa TandogNo ratings yet
- NURSES NOTES With CaseDocument4 pagesNURSES NOTES With CaseGrape JuiceNo ratings yet
- Module 1 Evolution of NursingDocument11 pagesModule 1 Evolution of NursingMelissa TesalonaNo ratings yet
- Text Book Rental FormDocument1 pageText Book Rental FormEphraim PryceNo ratings yet
- Health Assessment NCM 101 Lec Learning MatDocument5 pagesHealth Assessment NCM 101 Lec Learning MatSheen CatayongNo ratings yet
- IntraoperativeDocument4 pagesIntraoperativeLynette Roldan RN100% (1)
- Admitting Patient: When Admitting A Patient What Are The Basic Procedures?Document4 pagesAdmitting Patient: When Admitting A Patient What Are The Basic Procedures?diah ayuNo ratings yet
- Funda SummerDocument216 pagesFunda SummerNom NomNo ratings yet
- Colostomy Irrigation ProcedureDocument24 pagesColostomy Irrigation ProcedureJan Federick Bantay100% (1)
- CHNDocument12 pagesCHNJhara100% (1)
- Communication Process in NursingDocument37 pagesCommunication Process in NursingLalyn BalasbasNo ratings yet
- Health Education Prelim)Document3 pagesHealth Education Prelim)Joselyn Cabiles-GanhinhinNo ratings yet
- NCM 112 Lecture Notes (Respiratory System and Its Diseases)Document9 pagesNCM 112 Lecture Notes (Respiratory System and Its Diseases)Kyle FernandezNo ratings yet
- Tepid Sponge BathDocument5 pagesTepid Sponge BathJane LaquihonNo ratings yet
- Early Beliefs & Practices: History of Nursing in The PhilippinesDocument11 pagesEarly Beliefs & Practices: History of Nursing in The PhilippinesJifford AbayonNo ratings yet
- Proper Excreta Disposal, Food Safety and Environmental HealthDocument15 pagesProper Excreta Disposal, Food Safety and Environmental HealthEden LacsonNo ratings yet
- Let's Check - Divinagracia N AgravanteDocument2 pagesLet's Check - Divinagracia N AgravanteGladys YaresNo ratings yet
- Emergency Nursing CareDocument7 pagesEmergency Nursing CareCG Patron BamboNo ratings yet
- Chapter 36 Skin Integrity and Wound CareDocument7 pagesChapter 36 Skin Integrity and Wound CareKathleen FrugalidadNo ratings yet
- Assessing Musculoskeletal (MSK) SystemDocument8 pagesAssessing Musculoskeletal (MSK) SystemKeren GaciasNo ratings yet
- C C C M MMMM MM M MMM 3mm MMMMM MM M MMMMMDocument4 pagesC C C M MMMM MM M MMM 3mm MMMMM MM M MMMMMjohkieNo ratings yet
- Handwashing Techniques & ImportanceDocument15 pagesHandwashing Techniques & ImportanceNis DimagibaNo ratings yet
- Procedure Checklist On OxygenationDocument2 pagesProcedure Checklist On OxygenationKhatlen BagaresNo ratings yet
- COMPREHENSIVE NURSING ACHIEVEMENT TEST (RN): Passbooks Study GuideFrom EverandCOMPREHENSIVE NURSING ACHIEVEMENT TEST (RN): Passbooks Study GuideNo ratings yet
- Nursing Process DiagnosingDocument49 pagesNursing Process DiagnosingAnuchithra100% (2)
- Nursing Assessment ProcessDocument17 pagesNursing Assessment ProcessJustineNo ratings yet
- The Nervous System: EssentialsDocument18 pagesThe Nervous System: EssentialsAnna LaritaNo ratings yet
- Health EdDocument4 pagesHealth EdAnna LaritaNo ratings yet
- Breast and Lymphatic System AssessmentDocument31 pagesBreast and Lymphatic System AssessmentAnna LaritaNo ratings yet
- King'S Theory of Goal Attainment: Presented By: Group 5 Dapa Pasco Emanel Magtabog GametDocument16 pagesKing'S Theory of Goal Attainment: Presented By: Group 5 Dapa Pasco Emanel Magtabog GametAnna LaritaNo ratings yet
- Urinary System 1Document24 pagesUrinary System 1Anna LaritaNo ratings yet
- Notes To PrintDocument11 pagesNotes To PrintAnna LaritaNo ratings yet
- BUDESONIDEDocument1 pageBUDESONIDEAnna LaritaNo ratings yet
- CeftriaxoneDocument2 pagesCeftriaxoneAnna LaritaNo ratings yet
- Recipients of Nursing: American Nurses Association (ANA) Preventing IllnessDocument3 pagesRecipients of Nursing: American Nurses Association (ANA) Preventing IllnessAnna LaritaNo ratings yet
- Ce Fur OximeDocument1 pageCe Fur OximeAnna LaritaNo ratings yet
- Zinc SulfateDocument1 pageZinc SulfateAnna LaritaNo ratings yet
- Assessment Diagnosis Planning Intervention Evaluation: Name: Section: SubjectDocument2 pagesAssessment Diagnosis Planning Intervention Evaluation: Name: Section: SubjectAnna LaritaNo ratings yet
- Pharmacologi C: For Treatment Of: Maximum Dose: Minimum Dose: Available Forms: BeforeDocument2 pagesPharmacologi C: For Treatment Of: Maximum Dose: Minimum Dose: Available Forms: BeforeAnna LaritaNo ratings yet
- ALBUTEROLDocument1 pageALBUTEROLAnna LaritaNo ratings yet
- Fu Rose MideDocument2 pagesFu Rose MideAnna LaritaNo ratings yet
- CEFUROXIMEDocument1 pageCEFUROXIMEAnna LaritaNo ratings yet
- LayoutDocument8 pagesLayoutAnna LaritaNo ratings yet
- History: Allergies ToDocument2 pagesHistory: Allergies ToAnna LaritaNo ratings yet
- Cetirizine overviewDocument2 pagesCetirizine overviewAnna LaritaNo ratings yet
- Exotoxins Are Released From Bacterial Cells and May Act at Tissue Sites Removed From The Site ofDocument10 pagesExotoxins Are Released From Bacterial Cells and May Act at Tissue Sites Removed From The Site ofAnna LaritaNo ratings yet
- Pharmacologi C: Therapeutic: General: Maximum Dose: BeforeDocument2 pagesPharmacologi C: Therapeutic: General: Maximum Dose: BeforeAnna LaritaNo ratings yet
- Larita, Anna V. BSN-2A Nursing Care Plan NCM 107Document2 pagesLarita, Anna V. BSN-2A Nursing Care Plan NCM 107Anna LaritaNo ratings yet
- Gram-Negative Cocci and Coccobacilli of the Neisseriaceae FamilyDocument29 pagesGram-Negative Cocci and Coccobacilli of the Neisseriaceae FamilyAnna LaritaNo ratings yet
- STOOL MC3 REPORTsbgaufbDocument7 pagesSTOOL MC3 REPORTsbgaufbAnna LaritaNo ratings yet
- 6th Central Pay Commission Salary CalculatorDocument15 pages6th Central Pay Commission Salary Calculatorrakhonde100% (436)
- Assessment Diagnosis Planning Intervention Evaluation: Name: Section: SubjectDocument2 pagesAssessment Diagnosis Planning Intervention Evaluation: Name: Section: SubjectAnna LaritaNo ratings yet
- Tetanus: Treatment and Prevention VaccinationDocument29 pagesTetanus: Treatment and Prevention VaccinationAnna LaritaNo ratings yet
- Patient's Bill of RightsDocument5 pagesPatient's Bill of RightsKathrinna Palo100% (2)
- Case Study AdolescentDocument27 pagesCase Study AdolescentAnna Larita100% (2)
- Diagnosis and Management of Cystic Fibrosis: Rosalind L SmythDocument6 pagesDiagnosis and Management of Cystic Fibrosis: Rosalind L SmythMuhammadShahzadNo ratings yet
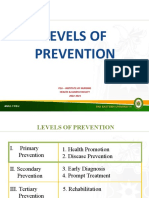
- Module 4 Levels of PreventionDocument29 pagesModule 4 Levels of PreventionZaren James D. RacaNo ratings yet
- Cancer ScreeningDocument8 pagesCancer Screeninglakshminivas PingaliNo ratings yet
- 5 Personality Traits and DynamicsDocument21 pages5 Personality Traits and DynamicsClara Del Castillo ParísNo ratings yet
- Post-Traumatic Stress Disorder - An Under-Diagnosed and Under-Treated Entity PDFDocument11 pagesPost-Traumatic Stress Disorder - An Under-Diagnosed and Under-Treated Entity PDFnegriRDNo ratings yet
- Tong Ren TechniqueDocument4 pagesTong Ren TechniqueEnshin100% (3)
- Med Term Syllabus (Liepe) 1.23Document5 pagesMed Term Syllabus (Liepe) 1.23mikeNo ratings yet
- DSM V PDFDocument33 pagesDSM V PDFRizky YantoroNo ratings yet
- Menumonic For DSM-IVDocument2 pagesMenumonic For DSM-IVbabygirl4u7465No ratings yet
- Sush Corrected-Unity PSYCH 1700 PDFDocument218 pagesSush Corrected-Unity PSYCH 1700 PDFDr-Jahanzaib GondalNo ratings yet
- Teerthanker Mahaveer College of Nursing: BATCH-2019-2021Document32 pagesTeerthanker Mahaveer College of Nursing: BATCH-2019-2021Prasann RoyNo ratings yet
- MSE DepressionDocument3 pagesMSE DepressionSam Raven AndresNo ratings yet
- Operationalizing the PDMDocument22 pagesOperationalizing the PDMRicardo LunaNo ratings yet
- TBH & TDAH Comorbidity of Attention Deficit Hyperactivity Disorder With Early - and Late-Onset BipDocument3 pagesTBH & TDAH Comorbidity of Attention Deficit Hyperactivity Disorder With Early - and Late-Onset BipVeio MacieiraNo ratings yet
- Pmh-Write Up-3-2Document5 pagesPmh-Write Up-3-2api-273372273No ratings yet
- Curriculum Vitae: ProfileDocument6 pagesCurriculum Vitae: ProfileMohammed ZahedNo ratings yet
- Assessme NT Diagnosis Inference Objectives Intervention / Implementatio N Rationale EvaluationDocument1 pageAssessme NT Diagnosis Inference Objectives Intervention / Implementatio N Rationale EvaluationAlakdan TorresNo ratings yet
- MouDocument3 pagesMouy jainNo ratings yet
- Improving The Accuracy of Medical Diagnosis With Causal Machine LearningDocument9 pagesImproving The Accuracy of Medical Diagnosis With Causal Machine Learningdrestadyumna ChilspiderNo ratings yet
- Egyptian Hospital Accreditation StandardsDocument71 pagesEgyptian Hospital Accreditation StandardskhayisamNo ratings yet
- Pathology Situational EthicsDocument28 pagesPathology Situational Ethicsmohitsingla_86No ratings yet
- Seminar on Childhood SchizophreniaDocument29 pagesSeminar on Childhood SchizophreniaRIYA MARIYATNo ratings yet
- CARE Checklist English 2013 PDFDocument1 pageCARE Checklist English 2013 PDFNithin NairNo ratings yet
- BFB For Psycmatric Disorders PDFDocument28 pagesBFB For Psycmatric Disorders PDFratusemut13No ratings yet
- Exploding Head SyndromeDocument11 pagesExploding Head SyndromeParsaant SinghNo ratings yet
- Toxic Epidermal Necrolysis (TEN) - The Chelsea Westminster Hospital Wound Management AlgorithmDocument31 pagesToxic Epidermal Necrolysis (TEN) - The Chelsea Westminster Hospital Wound Management AlgorithmKatNo ratings yet
- Virtual Clinical Duty Daily RequirementsDocument7 pagesVirtual Clinical Duty Daily RequirementsEdgie FabreNo ratings yet
- Mds SyllabusDocument78 pagesMds SyllabusFrancis PrathyushaNo ratings yet
- 21년도 SNOMED CT 활용 현황 설문조사 결과 보고서Document71 pages21년도 SNOMED CT 활용 현황 설문조사 결과 보고서Reina HatoriNo ratings yet
- Case StudyDocument7 pagesCase Studyapi-402806930No ratings yet