You might also like
- Outsmarting Diabetes: A Dynamic Approach for Reducing the Effects of Insulin-Dependent DiabetesFrom EverandOutsmarting Diabetes: A Dynamic Approach for Reducing the Effects of Insulin-Dependent DiabetesRating: 3.5 out of 5 stars3.5/5 (3)
- Small Fiber Neuropathy and Related Syndromes: Pain and NeurodegenerationFrom EverandSmall Fiber Neuropathy and Related Syndromes: Pain and NeurodegenerationSung-Tsang HsiehNo ratings yet
- Diabetic Peripheral NeuropathyDocument15 pagesDiabetic Peripheral NeuropathyValerie hongNo ratings yet
- Diabetic Neuropathy: What Does The Future Hold?Document7 pagesDiabetic Neuropathy: What Does The Future Hold?O. floriceNo ratings yet
- Balance Interventions For Diabetic Peripheral.3Document8 pagesBalance Interventions For Diabetic Peripheral.3Michael SelvarajNo ratings yet
- Neuropatia DiabéticaDocument18 pagesNeuropatia DiabéticaGustavo PestanaNo ratings yet
- Chemotherapy Related Cog. Dysf.Document9 pagesChemotherapy Related Cog. Dysf.Manuel Guerrero GómezNo ratings yet
- Validation of The Filipino-Translated Version of TDocument11 pagesValidation of The Filipino-Translated Version of TRoger Jr BrazilNo ratings yet
- Diabetic Peripheral Neuropathy: Epidemiology, Diagnosis, and PharmacotherapyDocument22 pagesDiabetic Peripheral Neuropathy: Epidemiology, Diagnosis, and PharmacotherapykaremiaNo ratings yet
- Diabetic Neuropathy CLINTHERDocument22 pagesDiabetic Neuropathy CLINTHERValerie hongNo ratings yet
- A Practical Two-Step Quantitative Clinical and Electrophysiological Assessment For The Diagnosis and Staging of Dianetic NeuropathyDocument9 pagesA Practical Two-Step Quantitative Clinical and Electrophysiological Assessment For The Diagnosis and Staging of Dianetic NeuropathyGhislaino ItabgaNo ratings yet
- Diabetes and Brain Health 2: Type 2 Diabetes and Cognitive Dysfunction-Towards Effective Management of Both ComorbiditiesDocument11 pagesDiabetes and Brain Health 2: Type 2 Diabetes and Cognitive Dysfunction-Towards Effective Management of Both ComorbiditiesAndreaPacsiNo ratings yet
- Symptomatic Therapy and Neurorehabilitation in Multiple SclerosisDocument10 pagesSymptomatic Therapy and Neurorehabilitation in Multiple Sclerosissarawu9911No ratings yet
- Prevalence and Spectrum of Diabetic Peripheral Neuropathy and Its Correlation With Insulinresistance - An Experience From Eastern IndiaDocument10 pagesPrevalence and Spectrum of Diabetic Peripheral Neuropathy and Its Correlation With Insulinresistance - An Experience From Eastern IndiaIJAR JOURNALNo ratings yet
- Treatment of Psychiatric Disorders in CKDDocument13 pagesTreatment of Psychiatric Disorders in CKDmplennaNo ratings yet
- PIIS0085253817308104Document3 pagesPIIS0085253817308104Freddy Shanner Chávez VásquezNo ratings yet
- Type 2 Diabetes: Annals of Internal MedicineDocument17 pagesType 2 Diabetes: Annals of Internal MedicinenicoolNo ratings yet
- Drug-Induced Peripheral Neuropathy, A Narrative ReviewDocument11 pagesDrug-Induced Peripheral Neuropathy, A Narrative ReviewMaksum Muh MaksumNo ratings yet
- Diabetic Neuropathies. 2023Document17 pagesDiabetic Neuropathies. 2023Arbey Aponte PuertoNo ratings yet
- Integrative Neuromuscular Medicine: Neuropathy and Neuropathic Pain: Consider The AlternativesDocument13 pagesIntegrative Neuromuscular Medicine: Neuropathy and Neuropathic Pain: Consider The AlternativesNawish SohailNo ratings yet
- Diabetes and Mental HealthDocument3 pagesDiabetes and Mental HealthVENNA FADILLAHNo ratings yet
- 7 DdeDocument5 pages7 DderahayuNo ratings yet
- PIIS0885392412001224Document12 pagesPIIS0885392412001224Catinca DobroghiiNo ratings yet
- Carmichael 2021Document25 pagesCarmichael 2021Andrei GeorgescuNo ratings yet
- Kepustakaan 2.1Document5 pagesKepustakaan 2.1Ikhsan FebriansyahNo ratings yet
- Archgenpsychiatry 2011 2Document8 pagesArchgenpsychiatry 2011 2ruba azfr-aliNo ratings yet
- Chemotherapy Induced Peripheral Neuropathy Risk ... 2010Document9 pagesChemotherapy Induced Peripheral Neuropathy Risk ... 2010gemita aldeaNo ratings yet
- 88 535 2 PBDocument8 pages88 535 2 PBHellyatill HasanahNo ratings yet
- Diagnosis and Management of Depression in Primary CareDocument8 pagesDiagnosis and Management of Depression in Primary CareMaria Jose OcNo ratings yet
- TX No Farmacologico QX NeuropsiquiatricosDocument16 pagesTX No Farmacologico QX NeuropsiquiatricosCONSEJO R4No ratings yet
- Kelley 2018Document1 pageKelley 2018GNNo ratings yet
- The Promise of Symptom-Targeted Intervention To Manage Depression in Dialysis Patients - Part 1Document6 pagesThe Promise of Symptom-Targeted Intervention To Manage Depression in Dialysis Patients - Part 1melissa dannyNo ratings yet
- Antipsychotic-Related Movement Disorders: Drug-Induced Parkinsonism vs. Tardive Dyskinesia-Key Differences in Pathophysiology and Clinical ManagementDocument16 pagesAntipsychotic-Related Movement Disorders: Drug-Induced Parkinsonism vs. Tardive Dyskinesia-Key Differences in Pathophysiology and Clinical ManagementudzmaNo ratings yet
- High-Dose Thiamine Improves Parkinson's SymptomsDocument9 pagesHigh-Dose Thiamine Improves Parkinson's SymptomsSOCIETE S.T.HNo ratings yet
- Huizinga DAN PELTIER 2007Document10 pagesHuizinga DAN PELTIER 2007TriNo ratings yet
- Jama Vacas 2021 It 210019 1630095346.97965Document2 pagesJama Vacas 2021 It 210019 1630095346.97965Juan Carlos Perez ParadaNo ratings yet
- Bennett 2016Document3 pagesBennett 2016Nabila ChakourNo ratings yet
- Recent Research AnDocument9 pagesRecent Research AnloloasbNo ratings yet
- Therapeutic Opportunities For Food Supplements inDocument10 pagesTherapeutic Opportunities For Food Supplements inTomás TeodoroNo ratings yet
- nihms-79056Document14 pagesnihms-79056angsokasatuNo ratings yet
- A Practical Guide For Nephrologists: Depression and Anxiety in ESRDDocument2 pagesA Practical Guide For Nephrologists: Depression and Anxiety in ESRDAnonymous I5mV0vK3WNo ratings yet
- JDM 2017110814284359Document8 pagesJDM 2017110814284359Mochamad BilalNo ratings yet
- Articulo Laser and Vitamin D and Magnesium Neuropathy Diabetic 2019Document5 pagesArticulo Laser and Vitamin D and Magnesium Neuropathy Diabetic 2019Karen ParraNo ratings yet
- Deep Brain Stimulation PDFDocument11 pagesDeep Brain Stimulation PDFTeodora FeliciaNo ratings yet
- HHS Public Access: Pilot Study of Exercise Therapy On Painful Diabetic Peripheral NeuropathyDocument16 pagesHHS Public Access: Pilot Study of Exercise Therapy On Painful Diabetic Peripheral NeuropathyParisha IchaNo ratings yet
- Articulo DiabetesDocument19 pagesArticulo DiabetesJosé Mario RodríguezNo ratings yet
- P71 NEJM DeliriumDocument10 pagesP71 NEJM DeliriumGabriel CampolinaNo ratings yet
- Park, 2019 - NEJM - DepressionDocument10 pagesPark, 2019 - NEJM - DepressionFabian WelchNo ratings yet
- Manejo Depresion 1Document10 pagesManejo Depresion 1Luis HaroNo ratings yet
- Lower Back PainDocument18 pagesLower Back PainmeganNo ratings yet
- Seminar: Epidemiology, Comorbidity, and DiagnosisDocument11 pagesSeminar: Epidemiology, Comorbidity, and DiagnosisMartin GiraudoNo ratings yet
- Evidence-Based Guideline: Treatment of Painful Diabetic NeuropathyDocument11 pagesEvidence-Based Guideline: Treatment of Painful Diabetic NeuropathyTriNo ratings yet
- Копия Towards prevention of diabetic peripheral neuropathy clinical presentation, pathogenesis, and new treatmentsDocument15 pagesКопия Towards prevention of diabetic peripheral neuropathy clinical presentation, pathogenesis, and new treatmentsn01zelolNo ratings yet
- ITC Type 2 Diabetes 2019Document16 pagesITC Type 2 Diabetes 2019ALEJANDRO DUEÑAS GUTIERREZNo ratings yet
- Everett 1995Document7 pagesEverett 1995yayan kurniawanNo ratings yet
- NIH Public Access: Diabetic Neuropathy: One Disease or Two?Document10 pagesNIH Public Access: Diabetic Neuropathy: One Disease or Two?AgunkRestuMaulanaNo ratings yet
- Mod8 Neurogenetics Reward Deficiency Syndrome As Root Cause Addiction Transfer 2023Document21 pagesMod8 Neurogenetics Reward Deficiency Syndrome As Root Cause Addiction Transfer 2023Jorge LabanowskiNo ratings yet
- Physical Exercise and Major Depressive Disorder in Adults Systematic Review and Meta AnalysisDocument17 pagesPhysical Exercise and Major Depressive Disorder in Adults Systematic Review and Meta AnalysisErick NunesNo ratings yet
- Efectos de La Manipulacion Esteopatica en El Desrden General de AnsiedadDocument11 pagesEfectos de La Manipulacion Esteopatica en El Desrden General de AnsiedadRafael MendietaNo ratings yet
- Diabetic NeuropathyDocument10 pagesDiabetic Neuropathyrafael rocha novaesNo ratings yet
- Cavanaugh 2014Document6 pagesCavanaugh 2014Jorge Luis Cifuentes EsparzaNo ratings yet
- Bu Bela 2018Document7 pagesBu Bela 2018Wafi HidayatNo ratings yet
- Anson 2017Document12 pagesAnson 2017Jorge Luis Cifuentes EsparzaNo ratings yet
- Cancel A Carral 2018Document6 pagesCancel A Carral 2018Jorge Luis Cifuentes EsparzaNo ratings yet
- CH 7b - Shift InstructionsDocument20 pagesCH 7b - Shift Instructionsapi-237335979100% (1)
- Anatomy Book For DoctorsDocument3 pagesAnatomy Book For DoctorsMuhammad JunaidNo ratings yet
- SoA DMI0037464664 130615102023Document2 pagesSoA DMI0037464664 130615102023sabkipolkholdeNo ratings yet
- Fleet Management 101 Training Part 1:: Presenters Gary Hatfield, Mercury Associates William Gookin, Mercury AssociatesDocument22 pagesFleet Management 101 Training Part 1:: Presenters Gary Hatfield, Mercury Associates William Gookin, Mercury AssociatesAdolphe Hotereshi100% (1)
- Swollen EyelidsDocument4 pagesSwollen EyelidsNARENDRANo ratings yet
- VAT Registration Certificate UAEDocument1 pageVAT Registration Certificate UAEMaaz AzadNo ratings yet
- Indiga Indiga: Tech TechDocument32 pagesIndiga Indiga: Tech Techsunny100% (1)
- Ac-Ppt On Crystal OscillatorDocument10 pagesAc-Ppt On Crystal OscillatorRitika SahuNo ratings yet
- Autodesk 2016 Product Keys 1Document3 pagesAutodesk 2016 Product Keys 1EfrEn QuingAtuñaNo ratings yet
- Pashchimanchal Campus: Set ADocument1 pagePashchimanchal Campus: Set AAnonymous uTC8baNo ratings yet
- BCSP GuideDocument44 pagesBCSP GuideCarol Sarmiento DelgadoNo ratings yet
- Wall FootingDocument4 pagesWall FootingMunthir NumanNo ratings yet
- 304 TextsetlessonDocument18 pages304 Textsetlessonapi-506887728No ratings yet
- 04.1 Foreign Graduates1Document30 pages04.1 Foreign Graduates1Frederico CavalcanteNo ratings yet
- Chapter 12.1.2 Respiratory Substrates and RQDocument30 pagesChapter 12.1.2 Respiratory Substrates and RQnie20060301No ratings yet
- KV Admission EnclosureDocument1 pageKV Admission EnclosureLaishram PilotNo ratings yet
- Impromptu SpeechDocument44 pagesImpromptu SpeechRhea Mae TorresNo ratings yet
- Pink & Green Colorful Vintage Aesthetic Minimalist Manhwa Interior Decor Illustration Work From Home Basic PresentationDocument221 pagesPink & Green Colorful Vintage Aesthetic Minimalist Manhwa Interior Decor Illustration Work From Home Basic PresentationHứa Nguyệt VânNo ratings yet
- II If en April2015 EquitycompoundersDocument8 pagesII If en April2015 EquitycompoundersbgyggghjkkNo ratings yet
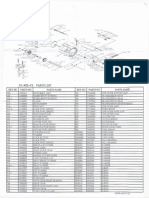
- Okuma CL302L Parts List & ManualDocument3 pagesOkuma CL302L Parts List & Manualcoolestkiwi100% (1)
- Bottom-Up Cost Evaluation of SOEC Systems (10-100MW)Document14 pagesBottom-Up Cost Evaluation of SOEC Systems (10-100MW)Roy JudeNo ratings yet
- Answer The Question According To The ListeningDocument10 pagesAnswer The Question According To The ListeningusuarioNo ratings yet
- Somatic TherapiesDocument170 pagesSomatic TherapiesDelyn Gamutan Millan100% (2)
- 2010 ATRA Technical SeminarDocument35 pages2010 ATRA Technical Seminartambache69100% (1)
- Essential information checklist for building plan submissionsDocument79 pagesEssential information checklist for building plan submissionsYu chung yinNo ratings yet
- Theory Best Suited For: Learning Theory Comparison ChartDocument1 pageTheory Best Suited For: Learning Theory Comparison ChartDAVE HOWARDNo ratings yet
- Pseudomonas aeruginosa identificationDocument26 pagesPseudomonas aeruginosa identificationNur AzizahNo ratings yet
- TCS303 Pumping Station ControllerDocument17 pagesTCS303 Pumping Station ControllerNAdreaNo ratings yet
- FD72 Technical Manual 28.10.09Document74 pagesFD72 Technical Manual 28.10.09cavgsi16vNo ratings yet
- Dallas Symphony Orchestra 2009 Annual ReportDocument14 pagesDallas Symphony Orchestra 2009 Annual ReportCharlie StephensonNo ratings yet