Professional Documents
Culture Documents
Jurnal Untuk Analisis 5
Jurnal Untuk Analisis 5
Uploaded by
Ester Yunita PuspitasariCopyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
Jurnal Untuk Analisis 5
Jurnal Untuk Analisis 5
Uploaded by
Ester Yunita PuspitasariCopyright:
Available Formats
quality in action
Ensuring Effective Care Transition
Communication: Implementation of an Electronic
Medical Record–Based Tool for Improved Cancer
Treatment Handoffs Between Clinic and
Infusion Nurses
Chintan Pandya, PhD, MPH, MBBS1; Tammy Clarke, RN, MS, OCN, BMTCN1; Elizabeth Scarsella, MSBA, RN, BSN, OCN1;
Alex Alongi, BS1; Stephanie Buia Amport, MBA, CPHQ2; Lauren Hamel, PhD3; David Dougherty, MD, MBA4
abstract
PURPOSE Ineffective handoffs contribute to gaps in patient care and medication errors, which jeopardize patient
safety and lead to poor-quality care. The project aims are to develop and implement a standardized handoff
process using an electronic medical record (EMR)–based tool to ensure optimal communication of treatment-
related information for patients receiving cancer treatment between oncology nurses.
METHODS A multidisciplinary team convened to develop a standard and safe treatment handoff process. The
intervention was developed over a series of phases using Plan-Do-Study-Act methodology, including current
workflow process mapping; identifying gaps, limitations, and potential causes of ineffective handoffs; and
prioritizing these using a Pareto chart. An EMR-based tool incorporating a standardized treatment handoff
process was developed. Study outcomes included proportion of handoff-related medication errors, tool utili-
zation, handoff completion, patient waiting time, and nurse satisfaction with tool. All outcomes were evaluated
before and after the intervention over a 1-year period.
RESULTS The proportion of medication errors as a result of ineffective handoffs was reduced from 10 of 17 (60%)
pre-intervention to 11 of 34 (32%) postintervention (P = .07). The EMR-based handoff tool was used in 9,274 of
10,910 (85%) patient treatment visits, and the handoff completion rate increased from 32% pre-intervention to
86% postintervention. Patient waiting time showed an average reduction of 2 minutes/patient/month. A majority
of nurses reported that the new tool conveyed necessary information (85% of nurses) and was effective in
preventing errors (81% of nurses).
CONCLUSION Multidisciplinary stakeholders guided the development and implementation of a standard handoff
process and an EMR-based tool to optimize communication between nurses during patient transition. The
intervention was associated with a reduction in the proportion of medication errors as the result of ineffective
handoffs. In addition, the intervention improved communication between nurses.
J Oncol Pract 15:e480-e489. © 2019 by American Society of Clinical Oncology
ASSOCIATED
CONTENT BACKGROUND handoff form with or without verbal exchange of es-
Appendix Wilmot Cancer Institute (WCI) at University of sential treatment-related information between nurses
Author affiliations Rochester Medical Center is a Quality Oncology is an expected practice at WCI. However, only 32% of
and support
Practice Initiative–certified cancer center that serves text-based handoff forms were completed between
information (if July 2014 and June 2016. In the same period, quality
applicable) appear
more than 6,000 analytic cancer cases throughout the
at the end of this upstate New York region. In 2011, WCI transitioned to evaluation of reported safety events with review of
article. the Epic electronic medical record (EMR) system. This medical records indicated that 60% of medication
Accepted on February required changes to cancer care delivery patterns, error events (10 of 17 events) were because of in-
11, 2019 and workflows, and clinical documentation including effective handoff communication between clinic and
published at infusion nurses. Ineffective handoffs can contribute to
handoff communication between nurses to exchange
jop.ascopubs.org on
April 4, 2019:
critical information about patients. During the transi- gaps in patient care, jeopardize patient safety, result in
DOI https://doi.org/10. tion of patients from the clinic to the infusion center to medication error, and lead to poor quality care
1200/JOP.18.00245 receive cancer treatment, the use of a text-based delivery.1,2
e480 Volume 15, Issue 5
EMR-Based Intervention for Effective Nurse Communication
The WCI quality and safety team participated in ASCO’s errors as the result of ineffective handoffs/total medication
Quality Training Program in 2016 to develop an intervention errors). These data were obtained from the incident reporting
to improve and standardize communication during hand- system, and the cause of error was determined through chart
offs between clinic and infusion nurses for patients re- review by an oncology quality nurse manager. Secondary
ceiving cancer treatments. The aims of this quality process outcomes were objective handoff communication
improvement project were as follows: (1) to develop and measures. These included the following: (1) handoff tool
implement an intervention consisting of a standard treat- utilization rate, which was whether the clinic nurse com-
ment handoff process using the EMR-based tool, and (2) to pleted the tool before the patient received treatment; (2)
evaluate the effect of the intervention on the primary study handoff completion rate, which was utilization rate plus
outcome (ie, medication errors as the result of ineffective whether the handoff tool was reviewed by the infusion nurse
handoffs) and secondary outcomes (ie, tool utilization, before treatment was administered; and (3) patient waiting
handoff completion, patient waiting time, and nurse sat- time, which was the time from patient check-in at the in-
isfaction with tool). fusion center to the time treatment was started. Last, we
elicited nurse satisfaction with the tool by conducting pre-
METHODS implementation and 1-month post-implementation follow-up
We implemented a formal quality improvement (QI) in- assessment surveys. Descriptive statistics were used to
tervention using the well-established Plan-Do-Study-Act analyze the primary and secondary outcomes. Bivariate
methodology to develop a standard and safe treatment analysis was performed using the t test and x2/Fisher’s exact
handoff process and an EMR-based handoff tool.3 A test in SAS version 9.4 (SAS Institute Inc., Cary, NC).
multidisciplinary team consisting of clinic and infusion
nurses, oncologists, pharmacists, a medical informaticist, RESULTS
and an information analyst was assembled. First, the team The proportion of medication errors as the result of in-
developed a project charter, conducted a review of baseline effective handoffs was 32% (11 of 34 errors) during the
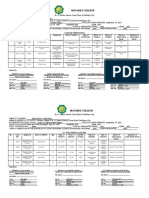
data, and formulated an aim statement. Second, a handoff 1-year postintervention period compared with 60% (10 of 17
process map (Appendix Fig A1, online only) was created to errors) during the 2 years before intervention (P = .07). The
highlight barriers to effective communication during patient WCI handoff tool was used in 9,274 of 10,910 patient visits
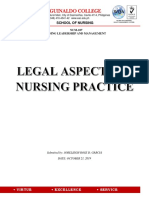
transition from clinic to infusion center. Third, with input (85%) and completed in 86% of those visits (7,976 of
from nurses involved in patient treatment handoff, a cause- 9,274) during the 1-year study period (Fig 1B). Patient
and-effect diagram (Fig A2, online only) and a Pareto chart waiting time was reduced by an average of 2 minutes/
(Fig 1A) were created to identify the most significant bar- patient/month between pre- and postintervention periods,
riers to an effective handoff process and to guide devel- but this finding was not statistically significant (Appendix
opment of the new handoff process. Table A1, online only).
Through cause-and-effect analysis and multivoting, it was Of the 60 clinic and infusion nurses who received the pre-
determined that the most commonly reported barriers to intervention assessment survey (presurvey), 42 nurses (26
effective handoffs were “handoff tool was not user-friendly” clinic and 16 infusion) completed it (70% response rate). A
and “a lack of standardization of handoff workflow.” Using majority of nurses (64%; 27 of 42 nurses) responded to a
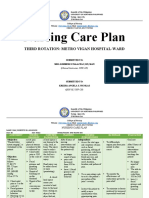
the Situation-Background-Assessment-Recommendation postintervention follow-up survey (postsurvey). A majority of
(SBAR) framework, which captures the four central com- nurses in postsurvey (85%) found the new tool to be
ponents of handoff communication, an EMR-based somewhat/very effective in preventing errors (v 48% pre-
handoff tool (WCI Handoff Tool) was developed to over- survey), and 81% (postsurvey) of nurses reported that the
come these barriers.4 On the basis of input and consensus new tool conveys all necessary information to treat patients
from providers involved in cancer treatment delivery and safely (v 58% presurvey; Table 1).
process, the team developed the contents for each com-
ponent of the SBAR framework. All components of the DISCUSSION
handoff process are entered into discrete data fields in the We designed and implemented a QI intervention consisting
WCI Handoff Tool to enable efficient capture of relevant of a standardized treatment handoff process and an EMR-
data and to automate tracking and reporting (Appendix based tool. Findings demonstrated improved handoff
Fig A3, online only). Education for implementation of the communication between nurses as well as improvement in
new handoff process and WCI Handoff Tool was provided quality and process outcomes. Specifically, the intervention
via group presentations and information sheets for clinic resulted in a lower proportion of medication errors as a
and infusion nurses. result of ineffective handoffs, increased utilization of the
handoff tool, decreased patient waiting times, and in-
MEASURES AND DATA ANALYSIS creased nurse satisfaction with the handoff process and
The primary outcome was the proportion of medication tool. The promise of EMR systems to enable improved
errors as the result of ineffective handoffs (medication processes, documentation, and reporting has yet to be
Journal of Oncology Practice e481
Pandya et al
A
9 100
8 100 90
94 97
90 80
7 87
Cumulative (%)
84
70
Frequency
6 77
71 60
5 65
55 50
4
40
3 42
30
2 20
26
1 10
8 5 4 3 2 2 2 1 1 1 1 1
0 0
...
...
..
...
t c nt nt
..
y
ly
g
e.
ol
d.
on
am
on
no me tie
dl
et
in
om ...
or
nt
om
to
te
n
pl
lv
i
i
f i a pa
ec
re
et
te
le
ie
ta
e
vo
rs
e
pl
eR
th
fr
en
om
iff
be
e
th
m
r
ng
fd
m
se
in
or
co
m
co
fr
on
e
cu
di
tu
of
cu
tr
ol
e
ed
ol
to
an
bl
ng
do
to
nd
s
no
to
s
pl
ila
d
st
i
di
of
ha
he
re
f
w
is
er
a
do
us
co
ie
av
fo
n
ft
pe
FIG 1. (A) Barriers to Wilmont Cancer
es
nd
ol
tio
an
un
ev
s
be
un
to
To
do
de
ay
U
H
ca
r
n
ar
on
Institute clinic and infusion completion
lw
e
io
ne
ly
Lo
ar
tio
tp
si
et
ta
nt
yo
a
za
fu
no
pl
re
of handoff tool. (B) Utilization (blue)
no
at
er
in
ili
m
ffe
D
ff
Ev
ut
ol
co
in
do
di
and completion (red) of the Wilmot
To
ol
nt
ol
an
ed
To
tie
To
H
us
Cancer Institute handoff tool in patient
Pa
ol
To
B visits during the 1-year study period.
100
88 88 88 90 90
85 85 86 86
83
Utilization and Completion
80
76 77 87
80 85 85 86 86 84 86
81 82 83
65
Rates (%)
60
46
40
Completion
34 Utilization
20
0
6
17
17
17
17
7
17
17
17
17
17
7
01
01
01
01
20
20
20
20
20
20
20
20
20
,2
,2
,2
,2
1,
2,
3,
5,
4,
6,
7,
8,
9,
12
11
10
12
n
n
n
n
n
n
n
n
Ja
Ja
Ja
Ja
Ja
Ja
Ja
Ja
Ja
Ja
Ja
Ja
Ja
realized for a large number of health care organizations. nurses was significant and sustained during the study
This is largely because of a lack of comprehensive, mul- period. Intervention components that may have contributed
tidisciplinary design of tools as well as a lack of optimal to such significant improvement in outcomes potentially
integration in clinical care workflows.5 In this QI in- include a user-friendly and efficient EMR-based tool, nurse
tervention, early engagement of multidisciplinary stake- training on standardized workflow and tool use, continuous
holders resulted in standardization of the handoff process, education, a monthly report tracking utilization of the tool,
development of an optimal handoff tool, and higher uptake and provider accountability. Moreover, the WCI Handoff
and integration of the intervention in routine clinic Tool was designed using the SBAR framework to capture
workflows. important information necessary for accurate chemother-
apy administration. Hence, the tool is user-agnostic and
The proportion of medication errors as the result of in-
can be used by any health care team member involved in
effective handoff decreased after intervention (11 of 34 v 10
the treatment administration workflow.
of 17 medication errors), despite a relatively shorter post-
intervention period (1 v 2 years) and higher total medication These findings should be considered within the limitations
error events (17 v 34 events) reported in the incident of the project. First, the influence of intervention on patient
reporting system. The increase in overall reporting may be satisfaction was not evaluated. However, it would be hard to
as a result of an increase in nurse awareness of the handoff argue that a patient would be satisfied with receiving cancer
process and their role in patient safety. The WCI Handoff care in a setting where communication between providers
Tool utilization and handoff completion rate between is poor, treatment delays are commonplace, and patients
e482 © 2019 by American Society of Clinical Oncology Volume 15, Issue 5
EMR-Based Intervention for Effective Nurse Communication
TABLE 1. Pre- and Postintervention Survey Results (N = 27 nurses)
Pre-Intervention (%) Postintervention (%)
Effectiveness of patient handoff tool in ensuring safe
treatment*
Not at all effective 3.70 0
Somewhat ineffective 18.52 0
Neutral 22.22 11.11
Somewhat effective 37.04 40.74
Very effective 18.52 48.15
Effectiveness of patient handoff tool in preventing errors*
Not at all effective 7.41 0
Somewhat ineffective 18.52 0
Neutral 25.93 14.81
Somewhat effective 33.33 44.44
Very effective 14.81 40.74
Effectiveness of patient handoff tool in promoting patient
satisfaction*
Not at all effective 7.69 0
Somewhat ineffective 11.54 0
Neutral 46.15 25.93
Somewhat effective 26.92 55.56
Very effective 7.69 18.52
Frequency of use of the handoff tool for same-day
appointments
Never 14.81 3.70
Rarely 0 0
Sometimes 3.70 7.41
Frequently 29.63 33.33
Always 51.85 55.56
Staff-identified barriers (same-day appointments)
Time consuming 0 0
Not part of current workflow 18.52 3.70
Not a service-line priority 11.11 0.00
Not used by counterpart 7.41 3.70
Other 7.41 3.70
Nurses responding “yes”:
Patient handoff tool conveys necessary information to 57.69 81.48
treat patient safely
Patient handoff tool has all of the helpful information* 66.67 100.00
Patient handoff tool is easy/very easy to use 66.70 85.10
*P , .05, statistically significant difference.
experience adverse events from medication errors as the ones contributed to the medication error rate. This limited
result of ineffective handoff. Second, the handoff form that our ability to make meaningful and important comparisons
was used in the pre-intervention period—albeit relatively between the two. The review of medication errors and their
infrequently—was not standardized and did not have causes was performed by a single quality nurse manager,
discrete elements to allow evaluation of its salient char- which could have led to bias in the study outcome esti-
acteristics, such as what components of communication mates. Finally, medication errors are self-reported in the
were included (eg, incomplete laboratory results) or which incident system and susceptible to individual biases, such
Journal of Oncology Practice e483
Pandya et al
as the ability to identify error and under- or over-reporting. of the incident system reports or an objective outcome
For example, a decrease in the number of incidents may measure.
indicate high-work volume and a lack of time to enter in- The QI intervention resulted in a standardized treatment
cidents as opposed to an actual reduction in incidents. Or, handoff process and a reduction in the proportion of
it could represent an increased focus on another quality medication errors as a result of ineffective communication at
area (eg, infusion reactions) that overshadowed the need WCI; it can be used as a model for rapid cycle improvement.
to report medication incidents. Future work could be Future efforts will focus on addressing noncommunication-
strengthened by using a more robust method to capture related factors contributing to medication errors in patients
medication error rate, such as multiple independent reviews with cancer who are receiving treatment.
AFFILIATIONS AUTHOR CONTRIBUTIONS
1
University of Rochester Medical Center, Rochester, NY Conception and design: Chintan Pandya, Tammy Clarke, Elizabeth
2
Yale New Haven Health, New Haven, CT Scarsella, Alex Alongi, Stephanie Buia Amport, Lauren Hamel, David
3
Wayne State University School of Medicine, Detroit, MI Dougherty
4
Dana-Farber Cancer Institute, Boston, MA Administrative support: Stephanie Buia Amport
Collection and assembly of data: Chintan Pandya, Tammy Clarke,
Elizabeth Scarsella, Alex Alongi, David Dougherty
CORRESPONDING AUTHOR
Data analysis and interpretation: All authors
Chintan Pandya, PhD, James P. Wilmot Cancer Center, University of
Rochester Medical Center, 601 Elmwood Ave, Box 704, Rochester, NY Manuscript writing: All authors
14642; e-mail: chintan_pandya@urmc.rochester.edu. Final approval of manuscript: All authors
Accountable for all aspects of the work: All authors
AUTHORS’ DISCLOSURES OF POTENTIAL CONFLICTS OF INTEREST
AND DATA AVAILABILITY STATEMENT ACKNOWLEDGMENT
Disclosures provided by the authors and data availability statement (if We thank Elizabeth Guancial, Karen Mietus, Lynn Rich, Nathaniel Wade,
applicable) are available with this article at DOI https://doi.org/10.1200/ Sean Goonan, Margaret Blaney, Melanie Bobry, Jen Galdys, and
JOP.18.00245. Elizabeth Alvino for their participation and contribution to the study. We
also thank our project sponsors, Jonathan Friedberg and Brian Martin.
REFERENCES
1. Kitch BT, Cooper JB, Zapol WM, et al: Handoffs causing patient harm: A survey of medical and surgical house staff. Jt Comm J Qual Patient Saf 34:563-570,
2008
2. Joint Commission on Accreditation of Healthcare Organizations: National Patient Safety Goals Hospital Version Manual Chapter, including implementation
expectations. 2007. https://www.jointcommission.org/PatientSafety/NationalPatientSafetyGoals/07_hap_cah_npsgs.htm
3. Arora VM, Johnson JK, Meltzer DO, et al: A theoretical framework and competency-based approach to improving handoffs. Qual Saf Health Care 17:11-14, 2008
4. Haig KM, Sutton S, Whittington J: SBAR: A shared mental model for improving communication between clinicians. Jt Comm J Qual Patient Saf 32:167-175, 2006
5. Asan O, Nattinger AB, Gurses AP, et al: Oncologists’ views regarding the role of electronic health records in care coordination. Clin Cancer Inform 2018:1-12,
2018
n n n
e484 © 2019 by American Society of Clinical Oncology Volume 15, Issue 5
EMR-Based Intervention for Effective Nurse Communication
AUTHORS’ DISCLOSURES OF POTENTIAL CONFLICTS OF INTEREST
Ensuring Effective Care Transition Communication: Implementation of an Electronic Medical Record–Based Tool for Improved Cancer Treatment Handoffs
Between Clinic and Infusion Nurses
The following represents disclosure information provided by authors of this manuscript. All relationships are considered compensated. Relationships are self-held
unless noted. I = Immediate Family Member, Inst = My Institution. Relationships may not relate to the subject matter of this manuscript. For more information about
ASCO’s conflict of interest policy, please refer to www.asco.org/rwc or ascopubs.org/jop/site/ifc/journal-policies.html.
David Dougherty
Honoraria: inPractice
No other potential conflicts of interest were reported.
Journal of Oncology Practice e485
Pandya et al
APPENDIX
Same-Day Infusion Handoff Process
Checks in at
Checks out Check in
clinic, arrived
of at
Patient
in EMR, and
clinic and infusion
has blood
makes and
drawn unless
follow-up arrived
done the day
appointments in EMR
before
MD/APP Makes
Provider
Communicate
sees patient decision
plan
and Seen without RN about
to
decision next
RN
to treat steps
Seen with RN
Handoff Information Makes prn
Identifies if
Clinic RN
tool is gathered phone call
patient going Information Yes Yes Release No Yes
initialized/ from EMR Finalize Urgent to infusion
to infusion known to initialize chemo-
loaded if and provider handoff? issue? RN to
for same-day handoff? therapy?
not started is entered update
treatment
prior into handoff the plan
No No Yes
No
Handoff tool Handoff tool
is not not
initialized completed
Yes Yes
Checks schedule Are
Reviews
printed for pods Checks chart Checks Are assessment,
Patient handoff tool No
and identifies for consent, flowcast Looks Yes laboratory laboratory results No
arrived in Is handoff and signs off Pages Issues
if patient coming orders, for for results within parameters,
initialized? whether team resolved?
Infusion RN
from clinic for laboratory schedule? appointment handoff consent and
complete or complete?
same-day results information orders
not
treatment signed?
Yes
Holding
No pattern No Wait Release
Patient
until the for chemo-
No treated
clinic laboratory therapy
appointment results
is complete
Yes
Patient Problem area
FIG A1. Process map for same-day infusion handoff process. APP, advanced practice provider; EMR, electronic medical record; MD, medical doctor; prn,
pro re nata (as needed); RN, registered nurse.
e486 © 2019 by American Society of Clinical Oncology Volume 15, Issue 5
EMR-Based Intervention for Effective Nurse Communication
Tool process Ineffective communication Patient
Infusion RN “pull”
to use tool If provider decides not to give chemotherapy
Tool is not always used
but orders are signed and handoff is
Data in the tool can be to completion Patient issues
not complete, the infusion RN will
lost, depending on release the chemotherapy
individual usage Clinic RN edits handoff after
infusion RN reviews it
Patient arrives in infusion
before handoff is complete Required data are unavailable The patient is late
or evolving Note “needs cosigned height/weight”
Tool is used differently
depending on the team
or RN style Orders are not signed and
infusion RN may call clinic RN
Tool completion is uncoupled for orders, especially if System issues
from patient treatment provider doesn’t answer page
Note says OK to treat but
“CMP pending” is written in
Data in the tool may not be
accurate or updated
Understanding the use of the tool
Tool utilization review is too Handoff is not complete
cumbersome Incomplete
handoff between
Everyone does handoff different clinic and infusion
Layout of tool is not user friendly Handoff not started
Information/comments It takes time to type in multiple factors;
in flowcast are incorrect Clinic RN needs time
it is time consuming Time for infusion RN to keep to complete handoff
checking if handoff is finalized
Infusion RN does not by clinic RN
Clinic RN adds follow-up
check handoff
appointments needed to
handoff, but that is a message Handoff does not count Clinic RN is working with
Patient calendar
for secretaries (not infusion RNs) The location of the tool in eRecord toward patient documentation multiple providers
is incorrect
Handoff is only used for
Infusion RN is too busy some patients
Tool is uncoupled from to check for handoff
the patient encounter. Handoff is not completed Clinic volume or case load
Clinic RN does not see the by the clinic RN
patient with the provider
Schedule Tool structure User variability Time
Purple is clinic and infusion Pale highlight are identified
barriers
Red is infusion
Dark highlight is top 7
Blue is clinic identified barriers
FIG A2. Cause-and-effect diagram. CMP, comprehensive metabolic panel; RN, registered nurse.
Journal of Oncology Practice e487
Pandya et al
SITUATION
Scheduled treatment category for today
Cancer treatments Chemotherapy Antibody Immunotherapy Transfusion IV fluids
Electrolytes Bisphosphonate Immunization Antibiotics Injection
Growth factor Other
Is this a new cancer Yes No
treatment?
BACKGROUND
Consent obtained Yes No Not needed
Laboratory results
Yes Not needed Pending
complete
ASSESSMENT
Current patient Scheduled treatment Scheduled treatment with change
status
Urgent or emergent treatment New treatment plan
Additional Disease progression Difficult social/emotional situation
relevant
information Other
RECOMMENDATION
OK to treat for Yes No Pending
scheduled
treatment
FIG A3. Epic-based Wilmot Cancer Institute handoff tool. IV, intravenous.
e488 © 2019 by American Society of Clinical Oncology Volume 15, Issue 5
EMR-Based Intervention for Effective Nurse Communication
TABLE A1. Patient Waiting Times During Treatment Visit (5 months pre- and postintervention)
Median Time From Premedication Visit to Treatment Infusion Median Time From Patient Check-In to Treatment Infusion
Month Pre-intervention (h:min) Postintervention (h:min) Pre-intervention (h:min) Postintervention (h:min)
1 0:34 0:28 1:02 1:03
2 0:31 0:28 1:03 1:00
3 0:35 0:30 1:08 1:00
4 0:29 0:31 1:01 1:04
5 0:31 0:31 1:04 1:02
Average 0:32 0:296 1:036 1:018
Difference 0:024 0:02
Abbreviations: h, hour; min, minute.
Journal of Oncology Practice e489
Used with permission. Copyright © American Society of Clinical Oncology 2019. All rights
reserved.
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5819)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (845)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Subjective:: Low Family Income As A Health ThreatDocument2 pagesSubjective:: Low Family Income As A Health ThreatJenniferValmocena50% (2)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Nurse Instructor Intake Supervisor Patient Care Manager in NYC Resume Malgorzata BladekDocument6 pagesNurse Instructor Intake Supervisor Patient Care Manager in NYC Resume Malgorzata BladekMalgorzataBladekNo ratings yet
- 0626nursing ConferencesDocument56 pages0626nursing ConferencesDainty Detuya-Bito Morales80% (10)
- Nurse Application LetterDocument5 pagesNurse Application LetterYano Sipit100% (1)
- Restraint of A Person - Adults OnlyDocument21 pagesRestraint of A Person - Adults OnlyAmbika SuwalNo ratings yet
- Establishing A Dedicated Difficult Vascular Access Team in The Emergency DepartmentDocument6 pagesEstablishing A Dedicated Difficult Vascular Access Team in The Emergency DepartmentOnur KNo ratings yet
- The Nursing Process-NCP and QUIZDocument43 pagesThe Nursing Process-NCP and QUIZMary Margareth GonzalesNo ratings yet
- Nursing Students Perceptions of Nursing MetaparadDocument9 pagesNursing Students Perceptions of Nursing MetaparadJustine Mae JayonaNo ratings yet
- (Clinica San Gabriel 05.07 GSA.P.20 PROCEDIMIENTO DE TRASLADO DE PACIENTES ENTRE UNIDADES DE ATENCION V.02) (Translated)Document13 pages(Clinica San Gabriel 05.07 GSA.P.20 PROCEDIMIENTO DE TRASLADO DE PACIENTES ENTRE UNIDADES DE ATENCION V.02) (Translated)Cesar GarciaNo ratings yet
- PDF Medical Evaluation of Child Sexual Abuse A Practical Guide 4Th Edition Martin A Finkel Editor Ebook Full ChapterDocument53 pagesPDF Medical Evaluation of Child Sexual Abuse A Practical Guide 4Th Edition Martin A Finkel Editor Ebook Full Chapterdaniel.mann336100% (4)
- ScriptDocument7 pagesScriptD A M N E R ANo ratings yet
- Emilio Aguinaldo College: School of NursingDocument11 pagesEmilio Aguinaldo College: School of NursingJor GarciaNo ratings yet
- Leyna Slivka-5Document1 pageLeyna Slivka-5api-490419585No ratings yet
- GEO-NSS-UM Belum PDFDocument271 pagesGEO-NSS-UM Belum PDFsukma wirabuanaNo ratings yet
- Chinese Nursing Research: Research Progress in Disaster Nursing Competency Framework of Nurses in ChinaDocument4 pagesChinese Nursing Research: Research Progress in Disaster Nursing Competency Framework of Nurses in ChinaSyahrizal FahmiantoNo ratings yet
- Fundamentals of Nursing Part 1Document10 pagesFundamentals of Nursing Part 1Nissie DegulacionNo ratings yet
- Maternal and Child Health Nursing Key TermsDocument3 pagesMaternal and Child Health Nursing Key TermsQuennie UmaliNo ratings yet
- Welcome To 4 West: Children's Healthcare of Atlanta at Egleston 404-785-6281 4 Floor of Tower 2, Butterfly ElevatorsDocument40 pagesWelcome To 4 West: Children's Healthcare of Atlanta at Egleston 404-785-6281 4 Floor of Tower 2, Butterfly ElevatorsHuy LeNo ratings yet
- Cases Ni MckoyDocument5 pagesCases Ni MckoycbuyazzNo ratings yet
- Healthcare HRM 2e PPT CH 01Document15 pagesHealthcare HRM 2e PPT CH 01Gumz100% (2)
- Chapter 3 Nursing Health HistoryDocument25 pagesChapter 3 Nursing Health HistoryLiezel Cauilan100% (2)
- Monica DraegerDocument1 pageMonica Draegerapi-310977516No ratings yet
- FAMILY CARE STUDY (PBBSC)Document11 pagesFAMILY CARE STUDY (PBBSC)JEEJANo ratings yet
- NCP PsychDocument2 pagesNCP PsychJray Inocencio50% (4)
- Dissertation Topics RguhsDocument6 pagesDissertation Topics RguhsWhereToBuyResumePaperNorman100% (1)
- Internship Journal 6Document2 pagesInternship Journal 6api-609630655No ratings yet
- Nursing Care Plan: Third Rotation: Metro Vigan Hospital-WardDocument5 pagesNursing Care Plan: Third Rotation: Metro Vigan Hospital-WardKrizha Angela NicolasNo ratings yet
- Traits of A Successful Nurse ManagerDocument2 pagesTraits of A Successful Nurse ManagerBethChay Lacson100% (1)
- Department of Health - Use, Collection, and Reporting of Infection Control DataDocument58 pagesDepartment of Health - Use, Collection, and Reporting of Infection Control DataNews10NBCNo ratings yet
- Bahasa InggrisDocument2 pagesBahasa InggrisAde Muliana LestariNo ratings yet