You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (842)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5806)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Story GridDocument346 pagesThe Story Gridjoel3edwards97% (36)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Goal and Scope of PsychotherapyDocument4 pagesGoal and Scope of PsychotherapyJasroop Mahal100% (1)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Chapter 1 Cell StructureDocument195 pagesChapter 1 Cell StructureVersha 2021100% (1)
- Administration of Total Parenteral Nutrition (TPN) - Adults and Children (Not NICU)Document15 pagesAdministration of Total Parenteral Nutrition (TPN) - Adults and Children (Not NICU)Giri SivaNo ratings yet
- Test Certificate: CM/L-NO:5530357Document10 pagesTest Certificate: CM/L-NO:5530357TARUNKUMARNo ratings yet
- Lesson-Exemplar-Template - ActivityDocument9 pagesLesson-Exemplar-Template - ActivityFrank Enciso Tronco100% (4)
- Idoc - Pub Medical Check Up FormDocument4 pagesIdoc - Pub Medical Check Up FormBobly SweaggerNo ratings yet
- Inc. Magazine - 09.2022Document172 pagesInc. Magazine - 09.2022Aman SharmaNo ratings yet
- COT 1 - (Science 7) - Cell To Biosphere 4as Semi-Detailed LPDocument10 pagesCOT 1 - (Science 7) - Cell To Biosphere 4as Semi-Detailed LPARLENE AGUNOD100% (1)
- mathematicsproficiencyattitudeandperformanceofgrade9studentsinprivatehighschoolsinBukidnonPhilippines PDFDocument15 pagesmathematicsproficiencyattitudeandperformanceofgrade9studentsinprivatehighschoolsinBukidnonPhilippines PDFNacivah BasherNo ratings yet
- Acalypha Indica and Curcuma Longa Plant Extracts Mediated ZNS Nanoparticles PDFDocument9 pagesAcalypha Indica and Curcuma Longa Plant Extracts Mediated ZNS Nanoparticles PDFRabeea NasirNo ratings yet
- Impact of COVID-19 On Student LifeDocument10 pagesImpact of COVID-19 On Student LifeZunii MalikNo ratings yet
- Unit IV Sheet Metal ProcessesDocument40 pagesUnit IV Sheet Metal ProcessesAJAY08No ratings yet
- CEOCOR 87 Cathodic Disbonding of Steelpipe CoatingsDocument26 pagesCEOCOR 87 Cathodic Disbonding of Steelpipe CoatingsMAHESH CHANDNo ratings yet
- Abb Acs604 (Es)Document94 pagesAbb Acs604 (Es)ndani10No ratings yet
- Christmas Book 2004Document98 pagesChristmas Book 2004Ron BarnettNo ratings yet
- Nabin Bhusal Oracle Developer (1)Document6 pagesNabin Bhusal Oracle Developer (1)HARSHANo ratings yet
- Good Practice Guide No. 120: Avoidance of Corrosion in Plumbing SystemsDocument16 pagesGood Practice Guide No. 120: Avoidance of Corrosion in Plumbing SystemsMochamad Irvan MaulanaNo ratings yet
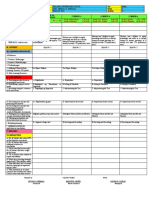
- DLL Q3 Week 4 Day5 WWDocument3 pagesDLL Q3 Week 4 Day5 WWCecilia Guevarra DumlaoNo ratings yet
- Unit Study Guides - CRCT Study GuidesDocument4 pagesUnit Study Guides - CRCT Study Guidesapi-37741282No ratings yet
- River System of BangladeshDocument3 pagesRiver System of Bangladeshtonmoy50% (2)
- Sociologia Şi Ştiinţa Naţiunii În Doctrina Lui Dimitrie GustiDocument35 pagesSociologia Şi Ştiinţa Naţiunii În Doctrina Lui Dimitrie GustiSaveanu RazvanNo ratings yet
- Theory Z Mini Research Term PaperDocument19 pagesTheory Z Mini Research Term PaperBirhanuNo ratings yet
- Challenges of Provision of Sewerage Service in The East Zone of Metro ManilaDocument11 pagesChallenges of Provision of Sewerage Service in The East Zone of Metro ManilaOswar MungkasaNo ratings yet
- Effects of Adiabatic Flame Temperature On Flames CharacteristicDocument12 pagesEffects of Adiabatic Flame Temperature On Flames CharacteristicAhmed YasiryNo ratings yet
- RIZALDocument6 pagesRIZALElaine Key MarasiganNo ratings yet
- Mobile Wireless Communications 1St Edition Schwartz Solutions Manual Full Chapter PDFDocument22 pagesMobile Wireless Communications 1St Edition Schwartz Solutions Manual Full Chapter PDFelysiarorym2ek100% (9)
- Harsh PatelDocument14 pagesHarsh PatelPradeepNo ratings yet
- (EIE529) Assignment 2Document3 pages(EIE529) Assignment 2JefferyMak100% (1)
- 9ER1 Question BookletDocument16 pages9ER1 Question BookletCSC TylerNo ratings yet