You might also like
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Typology of Nursing ProblemsDocument1 pageTypology of Nursing ProblemsMicaela Andrea CieloNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- COPAR Teaching Plan Malnutrition and Waste DisposalDocument5 pagesCOPAR Teaching Plan Malnutrition and Waste DisposalMicaela Andrea CieloNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- COPAR Crossing Bayabas Teaching PlanDocument12 pagesCOPAR Crossing Bayabas Teaching PlanMicaela Andrea CieloNo ratings yet
- ARTICLEREADING Acute Coronary SyndromeDocument3 pagesARTICLEREADING Acute Coronary SyndromeMicaela Andrea CieloNo ratings yet
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- DRUGSTUDY Tetanus ToxoidDocument1 pageDRUGSTUDY Tetanus ToxoidMicaela Andrea CieloNo ratings yet
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- COPAR Stray DogsDocument3 pagesCOPAR Stray DogsMicaela Andrea CieloNo ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- DRUGSTUDY TramadolDocument3 pagesDRUGSTUDY TramadolMicaela Andrea CieloNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- DRUGSTUDY AtorvastatinDocument2 pagesDRUGSTUDY AtorvastatinMicaela Andrea CieloNo ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- DRUGSTUDY TetanustoxoidDocument2 pagesDRUGSTUDY TetanustoxoidMicaela Andrea CieloNo ratings yet
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- DRUGSTUDY TamoxifenDocument2 pagesDRUGSTUDY TamoxifenMicaela Andrea CieloNo ratings yet
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
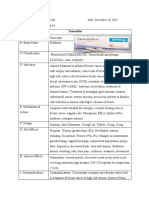
- Name: Micaela Andrea C. Cielo Date: Year & Section: BS Nursing 2A Drug Study: AlbendazoleDocument2 pagesName: Micaela Andrea C. Cielo Date: Year & Section: BS Nursing 2A Drug Study: AlbendazoleMicaela Andrea CieloNo ratings yet
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- DRUGSTUDY AmpicillinsodiumDocument3 pagesDRUGSTUDY AmpicillinsodiumMicaela Andrea CieloNo ratings yet
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Disposition: Dr. William Blake Bowler (Cpso# 50188)Document3 pagesDisposition: Dr. William Blake Bowler (Cpso# 50188)noNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Commonwealth of Massachusetts: One Ashburton Place, Room 1819 Boston, Massachusetts 02108Document53 pagesThe Commonwealth of Massachusetts: One Ashburton Place, Room 1819 Boston, Massachusetts 02108WBURNo ratings yet
- Aha Journal Stroke SecondaryDocument6 pagesAha Journal Stroke Secondaryfairuz syafira rahmahNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Vastarel MR 35mgDocument1 pageVastarel MR 35mgPhil Edgar Contreras RNNo ratings yet
- Curriculum For ProfessionalismDocument8 pagesCurriculum For ProfessionalismArham DurraniNo ratings yet
- Efficacy and Safety of Paliperidone Palmitate Eca ADocument14 pagesEfficacy and Safety of Paliperidone Palmitate Eca AMaria Fernanda AbrahamNo ratings yet
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- CMS DRGDocument14 pagesCMS DRGSean RNo ratings yet
- Imnci 130517223643 Phpapp02Document40 pagesImnci 130517223643 Phpapp02Archana SahuNo ratings yet
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Pharmacy ListDocument115 pagesPharmacy ListacroxmassNo ratings yet
- Macs 3mpq Jogc September 2011Document13 pagesMacs 3mpq Jogc September 2011Teresita BerenguerNo ratings yet
- List of 2 Years AffiliationDocument15 pagesList of 2 Years AffiliationAahad AmeenNo ratings yet
- Assignment Guidelines by The Teacher: Salman Ahmed KhanDocument3 pagesAssignment Guidelines by The Teacher: Salman Ahmed KhanHafsah JavedNo ratings yet
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The National Academies Press: Tracking Radiation Exposure From Medical Diagnostic Procedures: Workshop ReportDocument87 pagesThe National Academies Press: Tracking Radiation Exposure From Medical Diagnostic Procedures: Workshop ReportEdis ĐedovićNo ratings yet
- Psycho SocialDocument4 pagesPsycho Socialnkhadr2No ratings yet
- Generic Drug PresentationDocument47 pagesGeneric Drug PresentationNalini Koutha100% (1)
- Fundamentals of Nursing Letter AnswersDocument1 pageFundamentals of Nursing Letter AnswersEpaphras Joel MilitarNo ratings yet
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- 10.2 Major Surgical ProceduresDocument22 pages10.2 Major Surgical ProceduresishtiiiNo ratings yet
- Mary - Letter of RecommendationDocument1 pageMary - Letter of Recommendationapi-315592452No ratings yet
- Diagnóstico Pulpar 2009Document13 pagesDiagnóstico Pulpar 2009Eduardo Sáenz RiveraNo ratings yet
- Manifesto 2024Document64 pagesManifesto 2024uswah zahidNo ratings yet
- Extension Function of HEIsDocument14 pagesExtension Function of HEIsJuvy MojaresNo ratings yet
- The Different Types of IV Sets and Their UsesDocument1 pageThe Different Types of IV Sets and Their UsesPatricia VasquezNo ratings yet
- Request Letter For DEANSDocument1 pageRequest Letter For DEANSJenivic Empig PuedanNo ratings yet
- Conduct of LaborDocument8 pagesConduct of LaborChristine Evan HoNo ratings yet
- "Optimization of Instrumental Workflow in CSSD" at Hospital SectorDocument6 pages"Optimization of Instrumental Workflow in CSSD" at Hospital SectorIndra PratamaNo ratings yet
- Pharm.D 2nd Year SyllabusDocument21 pagesPharm.D 2nd Year Syllabus12 E 36 Yatri PatelNo ratings yet
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Every Patient Tells A Story by Lisa Sanders, M.D. - ExcerptDocument24 pagesEvery Patient Tells A Story by Lisa Sanders, M.D. - ExcerptCrown Publishing Group76% (17)
- On My Honor, I Have Neither Given Nor Received Aid On This Assignment or Test, and I Pledge That I Am in Compliance With The BSMCON Honor System.Document6 pagesOn My Honor, I Have Neither Given Nor Received Aid On This Assignment or Test, and I Pledge That I Am in Compliance With The BSMCON Honor System.api-273018832No ratings yet
- OSCE Instruction LetterDocument2 pagesOSCE Instruction Letterkenners100% (5)
- Medical - Strips (Medical Grade vs. "Hospital Grade")Document22 pagesMedical - Strips (Medical Grade vs. "Hospital Grade")Nirav DesaiNo ratings yet