You might also like
- The Effect of Non-Growth Factors On Chondrogenic Differentiation of Mesenchymal Stem CellsDocument9 pagesThe Effect of Non-Growth Factors On Chondrogenic Differentiation of Mesenchymal Stem CellsAndy HongNo ratings yet
- Management and Aesthetic Results of Support Grafts in Saddle Nose SurgeryDocument6 pagesManagement and Aesthetic Results of Support Grafts in Saddle Nose SurgeryAndy HongNo ratings yet
- Transforming Growth Factor-/3 and The Initiation of Chondrogenesis and Osteogenesis in The Rat FemurDocument13 pagesTransforming Growth Factor-/3 and The Initiation of Chondrogenesis and Osteogenesis in The Rat FemurAndy HongNo ratings yet
- Foc 2003 14 2 9Document8 pagesFoc 2003 14 2 9Andy HongNo ratings yet
- Growth of The Face and Dental Arches: January 2016Document16 pagesGrowth of The Face and Dental Arches: January 2016Andy HongNo ratings yet
- Anthropometric Profile Evaluation of The Midface in Patients With Cleft Lip and PalateDocument10 pagesAnthropometric Profile Evaluation of The Midface in Patients With Cleft Lip and PalateAndy HongNo ratings yet
- Ear Deformities Otoplasty and Ear Reconstruction LOVDocument16 pagesEar Deformities Otoplasty and Ear Reconstruction LOVAndy HongNo ratings yet
- Commissuroplasty: Sean M Parsel, DO, Ryan D Winters, MDDocument5 pagesCommissuroplasty: Sean M Parsel, DO, Ryan D Winters, MDAndy HongNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Technical Information: Range-Free Controller FA-M3 System Upgrade GuideDocument33 pagesTechnical Information: Range-Free Controller FA-M3 System Upgrade GuideAddaNo ratings yet
- TNM History Updated June2017Document2 pagesTNM History Updated June2017Lucas AndreoNo ratings yet
- HCPL 316J 000eDocument34 pagesHCPL 316J 000eElyes MbarekNo ratings yet
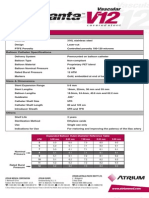
- Advanta V12 Data SheetDocument2 pagesAdvanta V12 Data SheetJuliana MiyagiNo ratings yet
- H107en 201906 r4 Elcor Elcorplus 20200903 Red1Document228 pagesH107en 201906 r4 Elcor Elcorplus 20200903 Red1mokbelNo ratings yet
- 1762 Ob8 PDFDocument16 pages1762 Ob8 PDFRodríguez EdwardNo ratings yet
- MarbiehistoryDocument6 pagesMarbiehistoryMarbie DalanginNo ratings yet
- Eng DS Epp-2314 1410Document2 pagesEng DS Epp-2314 1410MarkusAldoMaquNo ratings yet
- 18 Ray Optics Revision Notes QuizrrDocument108 pages18 Ray Optics Revision Notes Quizrraafaf.sdfddfaNo ratings yet
- Biology Accel Syllabus 2011-2012Document3 pagesBiology Accel Syllabus 2011-2012Mike DeleonNo ratings yet
- Anxiety Disorders - Causes, Types, Symptoms, & TreatmentsDocument5 pagesAnxiety Disorders - Causes, Types, Symptoms, & Treatmentsrehaan662No ratings yet
- Middle Range Theory Ellen D. Schulzt: Modeling and Role Modeling Katharine Kolcaba: Comfort TheoryDocument22 pagesMiddle Range Theory Ellen D. Schulzt: Modeling and Role Modeling Katharine Kolcaba: Comfort TheoryMerlinNo ratings yet
- Biomedical Engineering Handbook Revised 5 2015Document37 pagesBiomedical Engineering Handbook Revised 5 2015Teja GuttiNo ratings yet
- Significance of GodboleDocument5 pagesSignificance of GodbolehickeyvNo ratings yet
- 12.5 Collision Theory - ChemistryDocument15 pages12.5 Collision Theory - ChemistryAri CleciusNo ratings yet
- Purpose in LifeDocument1 pagePurpose in Lifeaashish95100% (1)
- RACI Matrix Design For Managing Stakeholders in PRDocument12 pagesRACI Matrix Design For Managing Stakeholders in PRRheza Nugraha Prabareswara100% (1)
- Potassium Fixation As Affected by Alternate Wetting and Drying in Some Soil Series of JharkhandDocument4 pagesPotassium Fixation As Affected by Alternate Wetting and Drying in Some Soil Series of JharkhandDr Amrit Kumar JhaNo ratings yet
- Column, Slab, Footing and Wall Footing Foundations: Class A MixingDocument47 pagesColumn, Slab, Footing and Wall Footing Foundations: Class A MixingGioharry Nul PanambulanNo ratings yet
- Assignment 2 Mat435Document2 pagesAssignment 2 Mat435Arsene LupinNo ratings yet
- Cathodic Protection Catalog - New 8Document1 pageCathodic Protection Catalog - New 8dhineshNo ratings yet
- Straight LineDocument15 pagesStraight LineAyanNo ratings yet
- Goliath 90 v129 eDocument129 pagesGoliath 90 v129 eerkanNo ratings yet
- De Vault 1996Document22 pagesDe Vault 1996Harumi OONo ratings yet
- SAT Practice TestDocument77 pagesSAT Practice TestfhfsfplNo ratings yet
- Shree New Price List 2016-17Document13 pagesShree New Price List 2016-17ontimeNo ratings yet
- Food Taste Panel Evaluation Form 2Document17 pagesFood Taste Panel Evaluation Form 2Akshat JainNo ratings yet
- Runyankore-Rukiga Dictionary Launch: President Yoweri Museveni's SpeechDocument28 pagesRunyankore-Rukiga Dictionary Launch: President Yoweri Museveni's SpeechThe New Vision50% (2)
- Kinematics in One DimensionDocument4 pagesKinematics in One DimensionAldrin VillanuevaNo ratings yet
- Nissan Copper LTDDocument11 pagesNissan Copper LTDankit_shahNo ratings yet