Professional Documents
Culture Documents
Actividad 4 Artículo 2
Uploaded by
byronOriginal Title
Copyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
Actividad 4 Artículo 2
Uploaded by
byronCopyright:
Available Formats
Review Article
https://doi.org/10.1038/s41564-018-0278-4
The role of the microbiota in infectious diseases
Josie Libertucci1 and Vincent B. Young 1,2*
The human body is colonized by a diverse community of microorganisms collectively referred to as the microbiota. Here, we
describe how the human microbiota influences susceptibility to infectious diseases using examples from the respiratory, gas-
trointestinal and female reproductive tract. We will discuss how interactions between the host, the indigenous microbiota and
non-native microorganisms, including bacteria, viruses and fungi, can alter the outcome of infections. This Review Article will
highlight the complex mechanisms by which the microbiota mediates colonization resistance, both directly and indirectly,
against infectious agents. Strategies for the therapeutic modulation of the microbiota to prevent or treat infectious diseases
will be discussed, and we will review potential therapies that directly target the microbiota, including prebiotics, probiotics,
synbiotics and faecal microbiota transplantation.
F
ollowing birth, and possibly before, the human body becomes microbiota14. Conversely, the indigenous microbiota may directly
colonized with a diverse community of archaea, bacteria, fungi, inhibit non-native microorganisms through various mechanisms.
viruses and microeukaryotes1–4. This diverse community of Disruptions in the established community structure and subsequent
microorganisms and the environment that they occupy is referred function change the overall balance between the microbiota and
to as the microbiome (see Box 1 for definitions). Colonization by host to result in altered infection susceptibility.
microorganisms during the first year of life is influenced by mul-
tiple factors, and influences human health throughout the life of the The microbiota mediates colonization resistance to prevent
host5. The microbial communities that inhabit the human body pro- infections. Invading non-native microorganisms have to overcome
vide essential functions for the host, including immunomodulation, barriers created by the microbiota that work to limit the persistence
breakdown of complex carbohydrates required for complete nutri- and colonization of pathogens15. The availability of a niche, whether
tion, and metabolism of drugs and other xenobiotics6–8. in terms of nutritional or functional space, is essential for coloni-
In addition to the aforementioned roles for the microbiota in zation. Factors that perturb the microbial community structure
maintaining homoeostasis, we will focus on an additional func- and function, such as antibiotics, allow for potential pathogens to
tion of the microbiota: the ability to influence susceptibility to and colonize, grow and persist. Growth and persistence of these micro-
outcomes of infectious diseases. The microbiota plays a key role in organisms provides an opportunity for them to come into close con-
colonization resistance, which is the prevention of growth, persis- tact with the host through direct contact with the epithelium or via
tence and subsequent infection by non-native microorganisms9. secreted products.
Classically, the study of infectious diseases has focused primarily on Community ecology principles can be applied to the micro-
non-indigenous microorganisms, commonly referred to as ‘patho- biota to better understand how the community protects the host
gens’, as central to the aetiopathogenesis of infectious diseases10. from invading microorganisms16. Three factors can be attributed
Under this schema for infectious diseases as originally postulated to the growth rate and ultimate survival of an invading species in
by Koch, infection occurs in a linear progression; a non-indigenous an established community: the availability of resources, presence of
microorganism enters the host, colonizes and causes disease10. For natural enemies and physical environment17. Persistence of invad-
over a century, research has focused on the mechanisms by which ing microorganisms is dependent on resource availability, or niche
a pathogen can overcome host defences and establish infection11. In opportunity. This concept was characterized in a study that assessed
this Review Article, we will expand from a focus on the host–patho- invasion ecology of an indigenous bacterial species of the human
gen interaction and discuss how the indigenous microbiota is an intestinal tract18. The authors administered live bacteria—the pro-
additional element that plays a critical role in determining suscepti- biotic Bifidobacterium longum strain AH1206—to participants, and
bility to, and outcomes of, infectious diseases. found that long-term establishment, or persistence, of AH1206
was directly dependent on under-representation of an indigenous
Interactions among host, microbiota and pathogen B. longum species and functional genes related to carbohydrate uti-
Health and disease reflects the overall balance between host lization, resulting in higher resource availability, or a niche opportu-
responses, the indigenous microbiota and potential pathogens (see nity for AH1206. Consequently, B. longum was able to persist in the
Box 1 for a definition of ‘indigenous microorganism’)12. This bal- gut due to an available niche.
ance is maintained through mechanisms of colonization resistance, One prominent example of the importance of niche availability
which can be both directly and indirectly mediated by the microbi- in the pathogenesis of infectious disease is Clostridium difficile.
ota13. The microbiota can indirectly mediate colonization resistance C. difficile—a Gram-positive anaerobic spore-forming bacterium
by stimulating host mucosal immune defences to prevent inva- that can cause C. difficile infection (CDI)—is able to exploit host
sion of non-indigenous microorganisms and subsequent infection. nutrient availability to establish colonization in individuals that
Normal development and function of the mucosal immune system have been administered antibiotics. A prevailing hypothesis for
and its responses are influenced by the presence of the indigenous the cause of CDI is that antibiotic therapy disrupts the indigenous
Department of Internal Medicine, Infectious Diseases Division, University of Michigan Medical School, Ann Arbor, MI, USA. 2Department of Microbiology
1
and Immunology, University of Michigan Medical School, Ann Arbor, MI, USA. *e-mail: youngvi@med.umich.edu
Nature Microbiology | VOL 4 | JANUARY 2019 | 35–45 | www.nature.com/naturemicrobiology 35
Review Article NATuRe MicRoBiology
Box 1 | Glossary
Indigenous microorganism. A microorganism that resides with- Homoeostasis. For the purposes of this Review Article, this
in or on a host. refers to a stable state between host immune responses and the
Colonization resistance. The ability of the host and the indigenous microbiota.
indigenous microbiota to prevent growth and persistence of Infection. A disruption of homoeostasis that results in lower
foreign microorganisms. colonization resistance from either an indigenous or non-
Microbiome. A community of microorganisms (bacteria, archaea, indigenous microorganism(s).
microeukaryotes and viruses), and the environment (including Community structure. The composition of the microbiota, which
the specific environmental conditions) that they occupy. For encompasses both the range of unique species and their relative
example, the vaginal microbiome would include not only the abundance.
microorganisms that occupy that site, but also all aspects of the
Community function. The sum of the total activity of the
host, including (but not limited to) vaginal epithelial cells, mucus,
microbiota (for example, production of metabolites or metabolism
immune cells and immune cytokines. This is consistent with
of environmental compounds) at a given time and in a specific
the earliest uses of the term and the root word ‘biome’, meaning
environment.
environment161.
Prebiotic. Non-digestible complex polysaccharide food
Microbiota. A community of microorganisms that occupy a
compounds meant to stimulate the growth and/or activity of one
specific site or habitat. Often, the terms microbiota and microbiome
or more taxonomic groups of bacteria to provide a benefit to the
are used interchangeably. Here, we use microbiota when referring
health of the host.
only to the microorganisms, and reserve microbiome for when we
bring in all elements of a given microbial environment. Probiotic. Live bacteria in the form of supplements or within a
Metagenome. The collective genomes of a microbial community food product, which when ingested in adequate amounts, provide
in a given community or sample. health benefits to the host.
Metabolome. The collection of metabolites produced by a Synbiotic. A product that contains both prebiotics and probiotics.
community of microorganisms. For a given environment or site, FMT. The delivery of a faecal suspension from a healthy donor to a
this would include the metabolites produced by the community of recipient, administered to modulate the structure and/or function
microorganisms present, but also those produced from the host. of the microbiota with therapeutic intent.
gut microbiota, rendering the community susceptible to the veg- plays an essential role in excluding pathogenic expansion through
etative growth of C. difficile spores19. Murine models and human modulation of host responses to maintain homoeostasis (see Fig. 1
studies show that antibiotic administration can alter the com- for examples of how the microbiota modulates host responses).
position of the gut microbiota by diminishing a large portion of Indigenous and invading non-indigenous microorganisms are
bacterial taxa, predisposing individuals to CDI20,21 as a result of physically separated from epithelial cells by an overlying layer of
vacant nutrient niches, which was highlighted in a recent study22. mucus, which forms the outermost physical barrier of mucosal sur-
Using a murine model, different classes of antibiotics were admin- faces. The major components of the mucus layer are glycoproteins
istered via drinking water, or in the case of clindamycin given called mucins, which are differentially expressed within the gastro-
by intraperitoneal injection, to disrupt the caecal microbiome to intestinal tract, respiratory tract and female reproductive tract27–30.
evaluate C. difficile gene expression and metabolic profile. The Mucins are secreted from the apical side of the epithelium into the
authors found that C. difficile is a bacterial generalist—a bacte- lumen, with expression being either constitutive or regulated31.
rial species that is able to adapt to a variety of nutrient niches and The importance of mucus in creating a physical barrier for muco-
hosts, making it well suited to expand into niches cleared by a sal defence is clear in mice deficient in the major intestinal mucin,
range of antibiotics. Mathematical modelling predicted that indig- muc2. These muc2−/− animals have a diminished mucus layer, allow-
enous Lachnospiraceae are required for colonization resistance, ing the microbiota to come into close contact with the epithelium,
and murine models have shown a reduction of these bacteria leading to inflammation and the onset of colitis32.
following antibiotic treatment23. Mucin production is influenced by the presence and composi-
Antibiotics also aid the creation of a niche by altering bile acid tion of the indigenous microbiota, as germ-free mice show a reduc-
metabolism. C. difficile is transmitted as a spore, which requires tion in MUC2 production and the mucous layer is protected by
specific bile acid signals for maximum germination into active species belonging to the genera Bifidobacterium in SPF (specific-
vegetative cells. Studies have shown that antibiotics cause a pathogen-free) mice33. This notion is supported by recent research
decrease in microorganisms that have 7α-dehydroxylase activity, that used human intestinal organoids (HIOs) as a model system to
which in turn reduces secondary bile acids such as deoxycholate. understand the relationship between colonization of Escherichia coli
This reduction in deoxycholate causes an increase in the pri- (another early colonizer of the gut) and intestinal development34.
mary bile acid taurocholate. This disruption is important because The research showed that E. coli promotes the production of intes-
deoxycholate can inhibit the growth of C. difficile, whereas tauro- tinal epithelial mucins. In addition to indigenous microbiota influ-
cholate promotes the germination of spores. Therefore, antibiot- encing mucin production, pathogens can alter the presence and
ics that alter the concentration of deoxycholate prevent C. difficile composition of the mucous layer. MUC2 production is reduced
from germinating19,24–26. when C. difficile is injected into HIOs, and patients with CDI have
The mucosal immune system, which includes the physical and decreased MUC2 production35. Altering the composition of the
chemical barrier of the gut epithelium, secreted antimicrobial pep- microbiota (for example, through modifying dietary components)
tides (AMPs) and dynamic and adaptive production of targeted can exacerbate mucin degradation during infection. For example,
immunoglobulins, forms a robust system for regulating the compo- in mice that are deprived of dietary fibre during Citrobacter roden-
sition of the indigenous microbiota and responding to pathogenic tium infection, the composition of the microbiota is enriched with
challenges. When these mechanisms are deficient, the host is more bacterial species that can degrade host mucins, resulting in greater
susceptible to infection. However, the indigenous microbiota itself epithelial access and, in this case, lethal colitis36. Thus, mucin
36 Nature Microbiology | VOL 4 | JANUARY 2019 | 35–45 | www.nature.com/naturemicrobiology
NATuRe MicRoBiology Review Article
Invading non-indigenous
microorganisms
Inhibition Infection
SCFAs
Dietary fibre
Antibiotics High-fat diet
Salmonella C. difficile
AMPs
E. coli GPR43 IgA Paracellular permeability ?
Bifidobacterium Mucin
production
IL-22
B cells
DC and
macrophages
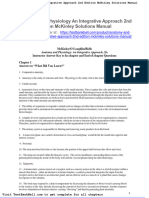
Fig. 1 | Disruptions to the microbiota alter mechanisms of colonization resistance and affect infection outcomes. Dietary fibre can alter the community
structure of the microbiota and subsequent function via the production of SCFAs, such as acetate, propionate and butyrate62. SCFAs can bind to the
G-protein-coupled receptor GPR43 and can stimulate AMPs, including REGIIIγ and β-defensins55. SCFAs can inhibit the growth of Salmonella, as it can
diffuse through the membrane, acidify the cytoplasm and inhibit growth58. Microorganisms, such as E. coli, can influence the production of mucins, thereby
limiting the access of indigenous and non-indigenous microorganisms to the epithelium33. Alterations to the microbiota (for example, as a result of
antibiotic treatment) can result in lowered B-cell-modulated production of IgA68, and a high-fat diet may result in increased paracellular permeability as
this dietary alteration results in claudin switching in murine models47, both of which can result in susceptibility to infection. DC, dendritic cell.
production is regulated by interactions between the indigenous tight junctions of the pulmonary alveolus, resulting in an influx of
microbiota, pathogens and host. fluid into the lung44. Disruption is associated with the loss of a tight
The passage of dietary antigens, ions and microbial products junction protein called claudin-4. Thus, careful regulation of epi-
from the lumen into the laminal propria is controlled by epithelial thelial barrier permeability in the presence of invading microorgan-
cells and can occur via transcellular or paracellular pathways37. The isms is essential for the maintenance of homoeostasis and inhibition
paracellular pathway is controlled by tight–junction–protein com- of infection.
plexes that connect adjacent epithelial cells at their apical border. Alterations to the microbiota resulting from dietary composi-
These are composed of occludin proteins, claudins and junctional tion (for example, a high-fat diet) could also affect paracellular
adhesion molecules, where occludin and claudins interact with permeability, and thus infection susceptibility. In mice, a high-fat
zonulae occludentes that link to the actin cytoskeleton to control diet is associated with changes to the microbiota45,46 and reduced
paracellular permeability and maintain cellular polarity38. The expression of tight junction proteins, resulting in impaired bar-
assembly/disassembly of tight junctions is a dynamic process, so rier function46. More recent studies have demonstrated that mice
that when this process or its components are impaired, paracellular fed a high-fat diet exhibit remodelling and claudin switching
permeability is altered and this can result in inflammation—a com- affecting paracellular permeability47. Given the established rela-
mon occurrence in inflammatory bowel disease39. tionship between microbiota composition and diet, and new evi-
Tight junctions are an important component of host defences dence that points to barrier function abnormalities resulting from
used to mitigate infections. In vitro studies have documented how dietary composition, this may be an under-appreciated mecha-
certain bacteria can alter the function of tight junctions40. For exam- nism driven by the microbiota, which contributes to increased
ple, C. difficile is able to disrupt tight junctions via the expression of infection susceptibility.
toxins41. The C. difficile toxins TcdA and TcdB are able to increase AMPs are essential components of innate immune defences,
paracellular permeability by disrupting the link between zonula and work to limit pathogen interaction with the epithelium. They
occludens-1 and the actin cytoskeleton. More recently, the disrup- are produced by host epithelial cells, neutrophils, paneth cells,
tion of tight junctions via C. difficile toxins has also been shown mast cells and adipocytes. These molecules can either be cationic
using a HIO system42. This has been observed for other pathogens, or anionic, due to a high concentration of either hydrophobic or
such as Yersina enterocolitica, which can disrupt the assembly of hydrophilic amino acids, and work by binding to negatively or
tight junction proteins to impair barrier function43. Barrier damage positively charged bacterial membranes to disrupt bacterial mem-
by pathogens is not restricted to the gut, nor are bacteria the only brane integrity48–50. AMPs are secreted at all mucosal surfaces
pathogen able to cause epithelial damage. Influenza A can disrupt and their expression can be enhanced by the presence of specific
Nature Microbiology | VOL 4 | JANUARY 2019 | 35–45 | www.nature.com/naturemicrobiology 37
Review Article NATuRe MicRoBiology
Table 1 | Examples of microbiota associated with altered mucosal immunity and increased infectious disease susceptibility
Site Infectious disease/condition Community structure Immune component References
Gastrointestinal tract Entamoeba histolytica, ↑ Prevotellaceae Augmented Th17-mediated 150–155
Giardia, ↑ Prevotella copri response
Cryptosporidium, ↑ Proteobacteria ↑IL-23, IL-1, IL-6, IL-8
Blastocystis hominis ↓ Firmicutes
Simian immunodeficiency virus ↑ Pasteurellaceae, Aggregatibacter, ↓Expression of TLR4, TLR8
Actinobacillus, Mycoplasma
HIV ↑ Proteobacteria, Prevotella ↑Activated T cells and
↓ Firmicutes myeloid dendritic cells
Respiratory tract Fungal or viral pneumonia ↑ Prevotella, Veillonella ↑ Th17 cells, IL-1α, IL-1β, IL-7 114, 156,157
Female reproductive tract Bacterial vaginosis ↑ Diversity ↑ IL-1β, IL-12p70 158–160
(clinical condition associated with ↓ Lactobacillus ↓IP-10, elafin
susceptibility to infection) ↑ Gardnerella vaginalis, A. vaginae,
HIV ↑ Diversity ↑Activated CD4+ T cells,
↓ Lactobacillus IL-23, IL-1β, IL-17
↑ Gardnerella vaginalis, A. vaginae,
Prevotella bivia
microorganisms and the composition of the microbiota51,52. shaping the community structure63–65. In mice, segmented fila-
Within the gut, Bacteroides thetaiotaomicron and Bifidobacterium mentous bacteria closely associated with the intestinal epithelium
breve upregulate the expression of the peptidoglycan-binding can enhance B-cell production of IgA, and interleukin-17 (IL-17)-
C-type lectin regenerating islet-derived protein IIIγ (REGIIIγ), producing CD4+ T cells, to promote barrier function66. The muco-
which is known to target and inhibit Gram-positive bacteria53. sal immune system keeps the expansion of segmented filamentous
Short-chain fatty acids (SCFAs) are products of bacterial fer- bacteria in check through neutrophil recruitment to the ileum via
mentation from non-digestible carbohydrates that act as an energy the production of IL-17A, and chemokine (C–X–C motif) ligands 1
source for colonocytes, and have been shown to alter the produc- and 2 (ref. 67). Microbiota-mediated IgA production is associated
tion of AMPs. The most abundant SCFAs in the colon are acetate, with reduced infection risk, since antimicrobial treatment results in
propionate and butyrate54, and the composition of the indigenous deficient pulmonary IgA production and, consequently, a greater
microbiota alters their production. Recently, it has been shown that risk of Pseudomonas aeruginosa pneumonia in intensive care unit
SCFAs can induce intestinal epithelial cell production of AMPs patients and murine models68.
by binding to the G-protein-coupled receptor GPR43 to stimulate
REGIIIγ and β-defensins55. Additionally, the production of SCFAs Relationship between microbial community structure, altered
in the colon can reduce the fitness of pathogens. For example, immune responses and infection susceptibility. In chronic
Salmonella can use propionate as a carbon source at low concen- inflammatory diseases, such as inflammatory bowel disease, celiac
trations, but high concentrations inhibit its growth56,57. A suggested disease and metabolic disorders, alterations to the microbiota have
mechanism by which propionate can limit the growth of Salmonella been associated with an altered immune response69–71. Before clini-
typhimurium is through disruption of intracellular pH homoeosta- cal presentation of these diseases, alterations to the microbiota may
sis58. Propionate diffuses across the membrane of Gram-negative result in host immune changes and subsequent chronic low-grade
bacteria, including S. typhimurium, and dissociates into a proton inflammation72,73. Recent clinical data have shown that there are
and propionate anion that acidifies the cytoplasm, resulting in a associations between chronic low-grade inflammation and suscep-
prolonged lag phase and reduced growth rate58,59. Propionate lev- tibility to certain infections. This was highlighted by a 2016 study
els are influenced by the composition of the indigenous microbiota that investigated the relationship between C-reactive protein (CRP)
(for example, species belonging to the genus Bacteroides), again and the risk of infection74. CRP is an acute-phase protein that plays
providing evidence of how the indigenous microbiota can limit a key role in the amplification of both local and systemic inflamma-
the growth, colonization and persistence of pathogens. Moreover, tion. The synthesis of this molecule is regulated by the proinflam-
Salmonella expression of virulence genes can also be regulated via matory cytokines IL-1 and IL-6 secreted at the site of inflammation
butyrate and propionate60,61. For example, HilD—a transcriptional or infection, and it is used as a marker of active inflammation in
regulator found within Salmonella pathogenicity island 1 (essen- Crohn’s disease and many other inflammatory conditions. Chronic
tial for invasion of Salmonella into the intestinal epithelium)—is low-level increases in CRP are associated with an increase in Gram-
post-translationally modified by propionyl-CoA—a product of negative bacterial infections, such as Gram-negative pneumonia.
propionate metabolism60. Other pathogens, such as C. difficile, are More recent data demonstrate that the indigenous microbiota
also limited by the production of SCFAs, as diets that encourage may play a role in altering host responses to produce low levels of
the development of propionate and butyrate are associated with inflammation, resulting in greater risk for infection. Table 1 shows
decreased bacterial fitness, resulting in a reduction of C. difficile- examples of infectious diseases that are associated with low-grade
mediated inflammation in murine models62. inflammation and specific microbiota community structure.
Another host factor influenced by the composition of the micro- An example of the relationship between the resident micro-
biota, immunoglobulin A (IgA), is constitutively secreted at muco- bial community and altered host immune responses that result in
sal surfaces to contain the indigenous microbiota but also to defend altered infectious disease susceptibility can be seen in the vaginal
the host from invading microorganisms. Studies in germ-free mice microbiota (described in Fig. 2). The community structure of the
demonstrate that secretion of IgA in the intestine is dependent vaginal microbiota can be described as either having low diver-
on the presence of the indigenous microbiota and plays a role in sity, consisting of mostly Lactobacillus species, or high diversity
38 Nature Microbiology | VOL 4 | JANUARY 2019 | 35–45 | www.nature.com/naturemicrobiology
NATuRe MicRoBiology Review Article
Non-inflamed Inflamed
HIV
Lactic acid
O
AMPs H3C Decreased
O– AMPs
OH
Low Lactobacillus
High-diversity community
Lactobacillus
Low-diversity community
Dendritic cell
DC
CD4+ T cell Macrophage
IL-6, TNF, IL-8
IL-1RA IL-6, TNF, IL-8 IL-1RA
Fig. 2 | Example of how the indigenous microbiota influences infectious disease susceptibility in the female genital tract. Vaginal microbiota with high
diversity and low Lactobacillus species prevalence are associated with inflammation and increased HIV-1 infection82,85,158,159. In the absence of Lactobacillus
species, there is decreased production of the AMP α-defensin97, which can bind to the gp120 receptor on HIV and stop entry into CD4+ T cells98.
Protonated lactic acid produced by Lactobacillus species results in decreased inflammatory mediators, including IL-6, IL-8 and TNFα99. TNFα exacerbates
epithelial damage, which can result in greater access of HIV to the host mucosal immune system92. Anti-inflammatory cytokines and responses, including
IL-1RA, are reduced in the presence of a high-diversity vaginal microbiota92.
(diversity being defined as species richness and evenness)75–79. This and Gardnerella vaginalis. In comparison, low inflammation was
has been shown to be highly associated with ethnicity80–82. The associated with a high abundance of Lactobacillus species, includ-
high-diversity vaginal microbiota subset is defined by a reduction ing Lactobacillus iners and Lactobacillus crispatus, and this is consis-
of Lactobacillus species and an increase in strict anaerobes, includ- tent with previous work where Lactobacillus was found to decrease
ing taxa belonging to the genera Prevotella, Dialister, Atopobium, the risk of acquiring HIV95. In another recent study, women who
Gardnerella, Megasphaera and Sneathia75,83–89. This high-diversity acquired HIV displayed greater vaginal microbiota diversity and
subset is associated with the clinical condition bacterial vagino- an increased risk of acquiring HIV if Parvimonas species types I
sis, and increased risk of acquiring sexually transmitted infections and II, Gemella asaccharolytica, Mycoplasma hominis, Leptotrichia,
such as human immunodeficiency virus, Neisseria gonorrhoeae, Eggerthella and Megasphaera were present96.
Chlamydia trachomatis and human papilloma virus85. The specific It is hypothesized that the diminished abundance of Lactobacillus
association between bacterial vaginosis and the acquisition of HIV species contributes to an increased risk of acquiring HIV because
is poorly understood. Previously, it has been reported that bacterial many defence mechanisms are repressed (Fig. 2). For example, a
vaginosis is associated with female genital tract inflammation90,91. decrease in Lactobacillus species results in decreased production
Secretion of an inflammatory cytokine profile consisting of IL-1β of the AMP α-defensin97. α-Defensins bind to the gp120 receptor
and IL-12p70 has been linked to a particular microbial composition on HIV and stop entry into CD4+ T cells98. This means that in an
(specifically, microbial communities with Prevotella, Atopobium environment where Lactobacillus species are reduced and HIV is
vaginae, Fusobacterium and Gardnerella) that is postulated to present, HIV may have greater access to CD4+ T cells. Additionally,
place women at higher risk of acquiring HIV. Anti-inflammatory Lactobacillus species are able to produce lactic acid. A recent study
cytokines and responses, including interleukin-1 receptor agonist has shown that protonated lactic acid results in decreased inflam-
(IL-1RA), are reduced in the presence of a high-diversity vaginal matory mediators, including IL-6, IL-8 and tumour necrosis factor
microbiota92. In a 2018 study, Lennard and colleagues were able to α (TNFα)99. TNFαexacerbates epithelial damage, so in the absence
identify microbial taxa that were associated with persistent bacterial of lactic acid, the increase in TNFαcan result in greater access of
vaginosis and a high inflammatory profile93. The use of a bead-based HIV to the host mucosal immune system92.
multiplex assay—a system able to profile the concentrations of host The relationship between microbiota structure and altered
cytokines, chemokines and growth factors—enabled the identifi- immune response has also been seen in the lung. Our understand-
cation of two distinct profiles: high and low inflammation94. The ing of the relationship between the structure and function of the
high inflammatory profile was associated with taxa that have been lung microbiota and health is in its infancy, partly due to the fact
classically associated with bacterial vaginosis, such as Megashaera that until relatively recently the lower respiratory tract (LRT) was
Nature Microbiology | VOL 4 | JANUARY 2019 | 35–45 | www.nature.com/naturemicrobiology 39
Review Article NATuRe MicRoBiology
considered to be sterile in healthy individuals100. Culture protocols Prebiotics. Prebiotics can result in a decrease in the use of antibiot-
within the clinical microbiology laboratory were developed to iden- ics required for infectious episodes and a decrease in infection rates
tify specific bacterial species that cause acute respiratory infections in the paediatric population118,119. There are multiple mechanisms
using selective media101, rather than as a means to survey the lung by which prebiotics may work to inhibit infectious diseases. In vitro
microbiota, which requires an extensive suite of culture condi- studies show that prebiotics work to promote the growth of some
tions102. The invasive nature of sampling the LRT via bronchoalveo- members of the indigenous microbiota by acting as a substrate for
lar lavage103 also meant that samples were not readily available. As a fermentation120–123, and many indigenous Bifidobacterium species
result, the Human Microbiome Project did not include the lungs in are able to breakdown galactooligosaccharide and fructooligosac-
its original surveys of the human microbiome104. chardie linkage bonds124. In the clinical setting, prebiotics may result
In many healthy individuals, the structure of the lung microbial in the expansion of targeted species within the community, and work
community comprises microorganisms that are found in the oro- to inhibit the growth of the pathogen through niche exclusion. The
pharyngeal community105–109. In 2015, Bassis and colleagues char- major fermentation products of prebiotics are SCFAs125. Therefore,
acterized the oral, nasal, lung and gastric communities, and found prebiotics may also work by restoring either bacterial metabolism
that membership was significantly shared between the lungs and (for example, butyrate), their secondary by-products (bile acid/
oral cavity109, including Prevotella, Streptococcus, Pasteurellaceae, salt metabolism) or immune responses regulated by SCFAs126,127,
Fusobacterium and Streptococcus. From this analysis, they postu- or through limiting the growth of pathogens58,62. In vivo, dietary
lated that the oral community seeds the LRT. Other studies have supplementation in healthy adults with resistant starch shows an
supported this hypothesis and identified the mechanism as sub- overall increase in butyrate production, but with high inter-indi-
clinical microaspiration in healthy individuals110. Dickson and col- vidual variation128. Prebiotics may also work by reducing adherence
leagues propose that their findings support the notion of the adapted of the pathogen to the host epithelium by mimicking ligands for
island model, where the distal lung bacterial community displays host-cell receptor sites129. This has been shown in an in vitro tissue
reduced richness and evenness, and reduced taxa similarity to the model in which pretreatment of cells with galactooligosaccharides
upper respiratory tract106,111. In healthy individuals, the lung micro- before exposure to enteropathogenic E. coli reduced the adherence
biome can be viewed as a balance between microbial immigration of enteropathogenic E. coli by as much as 70%130.
due to microaspiration and the elimination of bacteria (coughing
and mucocilliary clearance)112. Probiotics. Probiotics are hypothesized to prevent or treat infec-
There is evidence to suggest that high microbial diversity of tions by competing with pathogens for nutritional and functional
the lung microbiota is associated with infection113. Particularly, resources. Mouse models have shown that non-toxigenic C. difficile
enrichment of microbial community members within the lung, spores can prevent the colonization of toxigenic C. difficile131 and
seeded from the oral community and including anaerobes such can greatly reduce recurrent infection132. In addition to occupying a
as Prevotella and Veillonella, is associated with a distinct meta- vacant niche, probiotics may also modulate the microbiota by pre-
bolic and inflammatory profile. In a 2016 study, the authors found venting the growth of pathogens through the production of antimi-
that enrichment of Prevotella and Veillonella was associated with crobial substances such as bacteriocins133,134. In vitro studies have
increased numbers of Th17 cells and secretion of Th17 chemoat- also suggested that probiotics may block the adhesion of pathogenic
tractant cytokines (for example, IL-1αand IL-1β)114. This elevated bacteria to epithelial cells through direct interaction via lectin-like
inflammatory state may allow for increased infection suscepti- adhesion components135.
bility resulting from an altered immune response. Although the Synbiotics—substances containing both prebiotics and probiot-
Th17 response is associated with pathogen clearance, in some ics—have shown some recent success. Sepsis is a life-threatening
cases, there is also evidence to suggest that this response is associ- condition initiated by an infection that causes systemic inflam-
ated with impaired pathogen clearance. Aspergillus fumigatus is a mation, and is a major cause of morbidity and mortality in the
fungal pathogen that can result in pneumonia in immunocompro- neonatal population in the developing world136. For infants in the
mised patients. In an IL-17-deficient mouse model, clearance of developing world, death by sepsis occurs independent of antibi-
A. fumigatus conidia was enhanced, while the presence of IL-17 otic treatment, with no prevention method currently available136,137.
was associated with driving a T-helper 2 (Th2)-mediated inflamma- A recent randomized, double-blind, placebo-controlled trial tested
tory response characterized by eosinophilia115. the efficacy of an oral synbiotic (containing Lactobacillus plantarum
Alterations to microbiota community structure change the and a fructooligosaccharide) in the prevention of sepsis and sub-
overall dynamics between the microbiota and host to result in sequent death in neonates from India138. The results showed a sig-
altered infection susceptibility. Additionally, the composition of nificant reduction of sepsis and death in infants that received the
the microbiota may cause some individuals to be at a greater risk synbiotic. This synbiotic is currently the most cost-effective inter-
of acquiring infection. These examples suggest that there may vention for neonatal sepsis, costing US$1 for one week of treat-
be other pathogens that interact with the host and microbiota to ment, so there is great potential for this intervention given the
generate low levels of inflammation, which leads to reduced colo- efficacy and the low cost.
nization resistance. By understanding the relationships between
the microbiota, host responses and non-native microorganisms, FMT. FMT is the delivery of a faecal suspension from a healthy
we can propose treatments that act to prevent the invasion of donor to a recipient, with the intention of modulating the micro-
pathogenic microorganisms. biota in an attempt to resolve infection or, in some cases, disease
(either through structural or functional changes to the micro-
Therapies targeted to modulate the microbiota biota). FMT has gained significant attention over the past decade
Therapies that target the modulation of the microbiota aim to pre- as it has proven to be a highly effective treatment for recurrent or
vent colonization by pathogens or promote the clearance of patho- refractory CDI139,140. It has also shown some success in intestinal
gens. These therapies include prebiotics, probiotics and faecal decolonization of multidrug-resistant organisms to resolve disease,
microbiota transplantation (FMT; refer to Box 1 for definitions of including vancomycin-resistant enterococci, multidrug-resistant
these therapies)116,117. Although these therapies have shown success Staphylococcus aureus, and extended-spectrum β-lactamase- and
in the clinical setting, the mechanisms of action are varied and, in carbapenemase-producing Enterobacteriaceae141.
many cases, unclear. In this section, we discuss the proposed mech- The mechanism by which FMT works is currently unknown,
anisms underlying these therapies (outlined in Fig. 3). but evidence suggests multiple possible mechanisms. One possible
40 Nature Microbiology | VOL 4 | JANUARY 2019 | 35–45 | www.nature.com/naturemicrobiology
NATuRe MicRoBiology Review Article
a Prebiotic and probiotics
Prebiotics Probiotics SCFAs Invading non-indigenous microorganism
2
Indigenous 3
microbiota
1
b Faecal microbiota transplantation
FMT 2 Metabolite
production
3 Bacteriophage
1 Engraftment
Indigenous
microbiota
Fig. 3 | Hypothesized mechanisms for therapies preventing the colonization or clearance of pathogens. Prebiotics and probiotics can be used as
separate therapies or as a joint therapy (synbiotic) to prevent the colonization of pathogens, whereas FMT is used to clear the pathogen. a, Prebiotics are
hypothesized to work by facilitating the expansion of indigenous community members that are able to digest non-soluble fibre sources (1)120–123. These
members of the community may also increase SCFA production, which has been shown to regulate virulence expression in some pathogens (2)60,61.
Prebiotics may also inhibit pathogen binding to epithelial receptors via competition (3)130. Probiotics are hypothesized to work by filling a vacant niche
(either nutritional or functional)132. Depending on the strain of probiotics, SCFA production may increase as well (2). Using these therapies together
may give the live bacterial strain a better opportunity to occupy an available niche. b, It is unclear how FMT works, but it may be through restoration of
community structure and function via engraftment (1), or through restoration of the metabolome (2). Bacteriophages may also be transferred through
FMT (3), which may result in treatment success149.
mechanism is transplantation or engraftment of donor species to evaluated before FMT, and disease was associated with high abun-
the recipient microbiome, resulting in the replacement of missing dance of Caudovirales bacteriophages and low Caudovirales diver-
function142. Engraftment is possible in the case of C. difficile as anti- sity (richness and evenness) compared with healthy controls149.
biotic use results in the creation of nutritional niches. Many studies Positive clinical outcomes following FMT were associated with
have shown a shift in the recipient’s microbiota following success- alterations to the enteric virome and bacterial microbiota, and those
ful FMT143,144, although an increase in diversity does not necessar- who received donor faeces had a higher richness of Caudovirales
ily occur145. In a recent study, bacterial engraftment from donor to and greater treatment success.
host was determined using a machine-learning technique to pre-
dict the presence of operational taxonomic units following FMT Summary and conclusions
from metagenomics data146. However, actual engraftment of the Advances in surveying the complex, dynamic and diverse com-
entire faecal community may not be necessary for treatment suc- munities of microorganisms, both through culture-dependent and
cess. Staley and colleagues have shown that engraftment does not culture-independent techniques, have allowed us to understand
determine successful FMT in the treatment of recurrent or refrac- how our microbiota plays an important role in homoeostasis and
tory CDI147. Even more compelling evidence is provided from stud- infectious disease susceptibility. Altering the structure of a micro-
ies that have used filtrates from donor stools (called faecal filtrate bial community can affect function, and is associated with infec-
transfer) to treat patients with chronic-relapsing CDI to resolve dis- tious disease susceptibility and outcomes. Major strides have been
ease148. The success of faecal filtrate transfer suggests that engraft- taken towards understanding the mechanistic relationship between
ment or competition between bacteria may not have any influence the microbiota and infectious diseases, but many unanswered ques-
on success, but rather the transfer of bacterial components, metabo- tions remain. For infectious diseases that have been associated
lites and/or bacteriophages may mediate the observed beneficial with alterations of the microbiota (for example, bacterial vaginosis
effects of FMT. In a recent study, the virome of CDI patients was and increased risk of acquiring HIV), are these alterations to the
Nature Microbiology | VOL 4 | JANUARY 2019 | 35–45 | www.nature.com/naturemicrobiology 41
Review Article NATuRe MicRoBiology
microbiota causative? If so, what are the potential mechanisms? 23. Fleming-Davies, A. et al. In Women in Mathematical Biology (eds Layton,
Most of what we know about the microbiota and its relationship to A. & Miller, L.) 137–161 (Springer, New York, 2017).
24. Theriot, C. M. & Young, V. B. Interactions between the gastrointestinal
infectious diseases comes from studies that have focused on cata- microbiome and Clostridium difficile. Annu. Rev. Microbiol. 69,
loguing and measuring structure (taxonomy and diversity, respec- 445–461 (2015).
tively). Since structure can dictate function, how do alterations of in 25. Theriot, C. M., Bowman, A. A. & Young, V. B. Antibiotic-induced
situ function affect disease outcomes? To date, indigenous bacterial alterations of the gut microbiota alter secondary bile acid production and
communities have received the most attention. What do viruses and allow for Clostridium difficile spore germination and outgrowth in the large
intestine. mSphere 1, e00045-15 (2016).
fungi contribute to infectious disease susceptibility? We now know 26. Thanissery, R., Winston, J. A. & Theriot, C. M. Inhibition of spore
that infectious diseases are not a singular microorganism problem, germination, growth, and toxin activity of clinically relevant C. difficile
and as research shifts from a reductionist approach to understand- strains by gut microbiota derived secondary bile acids. Anaerobe 45,
ing the complex dynamics between the microbial community and 86–100 (2017).
the host, we will gain a greater understanding of the human micro- 27. Kato, K., Lillehoj, E. P., Lu, W. & Kim, K. C. MUC1: the first respiratory
mucin with an anti-inflammatory function. J. Clin. Med. 6, 110 (2017).
biota, learn how infectious diseases can be prevented, refine treat- 28. Andersch-Bjorkman, Y., Thomsson, K. A., Holmen Larsson, J. M.,
ments and create novel therapeutics. Ekerhovd, E. & Hansson, G. C. Large scale identification of proteins,
mucins, and their O-glycosylation in the endocervical mucus during the
Received: 14 March 2017; Accepted: 28 September 2018; menstrual cycle. Mol. Cell. Proteomics 6, 708–716 (2007).
29. Kim, K. C. Role of epithelial mucins during airway infection. Pulm.
Published online: 13 December 2018
Pharmacol. Ther. 25, 415–419 (2012).
30. Lesuffleur, T., Zweibaum, A. & Real, F. X. Mucins in normal and neoplastic
References human gastrointestinal tissues. Crit. Rev. Oncol. Hematol. 17, 153–180 (1994).
1. Aagaard, K. et al. The placenta harbors a unique microbiome. Sci. Transl. 31. Specian, R. D. & Neutra, M. R. Regulation of intestinal goblet cell secretion.
Med. 6, 237ra265 (2014). I. Role of parasympathetic stimulation. Am. J. Physiol. 242,
2. Wampach, L. et al. Colonization and succession within the human gut G370–G379 (1982).
microbiome by archaea, bacteria, and microeukaryotes during the first year 32. Van der Sluis, M. et al. Muc2-deficient mice spontaneously develop colitis,
of life. Front. Microbiol. 8, 738 (2017). indicating that MUC2 is critical for colonic protection. Gastroenterology
3. Nkamga, V. D., Henrissat, B. & Drancourt, M. Archaea: essential inhabitants 131, 117–129 (2006).
of the human digestive microbiota. Hum. Microbiome J. 3, 1–8 (2017). 33. Schroeder, B. O. et al. Bifidobacteria or fiber protects against diet-induced
4. Parfrey, L. W., Walters, W. A. & Knight, R. Microbial eukaryotes in the microbiota-mediated colonic mucus feterioration. Cell Host Microbe 23,
human microbiome: ecology, evolution, and future directions. Front. 27–40 (2018).
Microbiol. 2, 153 (2011). 34. Hill, D. R. et al. Bacterial colonization stimulates a complex physiological
5. Reynolds, L. A. & Finlay, B. B. Early life factors that affect allergy response in the immature human intestinal epithelium. eLife 6,
development. Nat. Rev. Immunol. 17, 518–528 (2017). e29132 (2017).
6. Jandhyala, S. M. et al. Role of the normal gut microbiota. World J. 35. Engevik, M. A. et al. Human Clostridium difficile infection: altered mucus
Gastroenterol. 21, 8787–8803 (2015). production and composition. Am. J. Physiol. Gastrointest. Liver Physiol. 308,
7. Su, C. et al. Helminth-induced alterations of the gut microbiota exacerbate G510–G524 (2015).
bacterial colitis. Mucosal Immunol. 11, 144–157 (2018). 36. Desai, M. S. et al. A dietary fiber-deprived gut microbiota degrades the
8. Lozupone, C. A., Stombaugh, J. I., Gordon, J. I., Jansson, J. K. & Knight, R. colonic mucus barrier and enhances pathogen susceptibility. Cell 167,
Diversity, stability and resilience of the human gut microbiota. Nature 489, 1339–1353.e1321 (2016).
220–230 (2012). 37. Ménard, S., Cerf-Bensussan, N. & Heyman, M. Multiple facets of intestinal
9. Lawley, T. D. & Walker, A. W. Intestinal colonization resistance. permeability and epithelial handling of dietary antigens. Mucosal Immunol.
Immunology 138, 1–11 (2013). 3, 247–259 (2010).
10. Koch, R. Die Ätiologie der milzbrand-krankheit, begründet auf die 38. König, J. et al. Human intestinal barrier function in health and disease.
entwicklungsgeschichte des Bacillus anthracis. Cohns Beitr. Biol. Pflanzen 2, Clin. Transl. Gastroenterol. 7, e196 (2016).
277–310 (1876). 39. Zeissig, S. et al. Changes in expression and distribution of claudin 2, 5 and
11. Falkow, S. Molecular Koch’s postulates applied to bacterial pathogenicity—a 8 lead to discontinuous tight junctions and barrier dysfunction in active
personal recollection 15 years later. Nat. Rev. Microbiol. 2, 67–72 (2004). Crohn’s disease. Gut 56, 61–72 (2007).
12. Young, V. B. The role of the microbiome in human health and disease: an 40. Fasano, A. et al. Vibrio cholerae produces a second enterotoxin, which
introduction for clinicians. Br. Med. J. 356, j831 (2017). affects intestinal tight junctions. Proc. Natl Acad. Sci. USA 88,
13. Buffie, C. G. & Pamer, E. G. Microbiota-mediated colonization resistance 5242–5246 (1991).
against intestinal pathogens. Nat. Rev. Immunol. 13, 790–801 (2013). 41. Nusrat, A. et al. Clostridium difficile toxins disrupt epithelial barrier
14. Round, J. L. & Mazmanian, S. K. The gut microbiota shapes intestinal function by altering membrane microdomain localization of tight junction
immune responses during health and disease. Nat. Rev. Immunol. 9, proteins. Infect. Immun. 69, 1329–1336 (2001).
313–323 (2009). 42. Leslie, J. L. et al. Persistence and toxin production by Clostridium difficile
15. Walter, J., Maldonado-Gómez, M. X. & Martínez, I. To engraft or not to within human intestinal organoids result in disruption of epithelial
engraft: an ecological framework for gut microbiome modulation with live paracellular barrier function. Infect. Immun. 83, 138–145 (2015).
microbes. Curr. Opin. Biotechnol. 49, 129–139 (2018). 43. Hering, N. A. et al. Yersinia enterocolitica induces epithelial barrier
16. Costello, E. K., Stagaman, K., Dethlefsen, L., Bohannan, B. J. M. & dysfunction through regional tight junction changes in colonic HT-29/B6
Relman, D. A. The application of ecological theory toward an cell monolayers. Lab. Invest. 91, 310–324 (2010).
understanding of the human microbiome. Science 336, 1255–1262 (2012). 44. Short, K. R. et al. Influenza virus damages the alveolar barrier by disrupting
17. Shea, K. & Chesson, P. Community ecology theory as a framework for epithelial cell tight junctions. Eur. Respir. J. 47, 954–966 (2016).
biological invasions. Trends Ecol. Evol. 17, 170–176 (2002). 45. De La Serre, C. B. et al. Propensity to high-fat diet-induced obesity in rats
18. Maldonado-Gomez, M. X. et al. Stable engraftment of Bifidobacterium is associated with changes in the gut microbiota and gut inflammation. Am.
longum AH1206 in the human gut depends on individualized features of J. Physiol. Gastrointest. Liver Physiol. 299, G440–G448 (2010).
the resident microbiome. Cell Host Microbe 20, 515–526 (2016). 46. Cani, P. D. et al. Selective increases of bifidobacteria in gut microflora
19. Theriot, C. M. et al. Antibiotic-induced shifts in the mouse gut microbiome improve high-fat-diet-induced diabetes in mice through a mechanism
and metabolome increase susceptibility to Clostridium difficile infection. associated with endotoxaemia. Diabetologia 50, 2374–2383 (2007).
Nat. Commun. 5, 3114 (2014). 47. Ahmad, R., Rah, B., Bastola, D., Dhawan, P. & Singh, A. B. Obesity-induces
20. Jernberg, C., Lofmark, S., Edlund, C. & Jansson, J. K. Long-term ecological organ and tissue specific tight junction restructuring and barrier
impacts of antibiotic administration on the human intestinal microbiota. deregulation by claudin switching. Sci. Rep. 7, 5125 (2017).
ISME J. 1, 56–66 (2007). 48. Zhang, L. J. & Gallo, R. L. Antimicrobial peptides. Curr. Biol. 26,
21. Buffie, C. G. et al. Profound alterations of intestinal microbiota following a R14–R19 (2016).
single dose of clindamycin results in sustained susceptibility to Clostridium 49. Jiang, Z. et al. Effects of net charge and the number of positively charged
difficile-induced colitis. Infect. Immun. 80, 62–73 (2012). residues on the biological activity of amphipathic α-helical cationic
22. Jenior, M. L., Leslie, J. L., Young, V. B. & Schloss, P. D. Clostridium difficile antimicrobial peptides. Biopolymers 90, 369–383 (2008).
colonizes alternative nutrient niches during infection across distinct murine 50. Wang, Z. & Wang, G. APD: the antimicrobial peptide database. Nucleic
gut microbiomes. mSystems 2, e00063-17 (2017). Acids Res. 32, D590–D592 (2004).
42 Nature Microbiology | VOL 4 | JANUARY 2019 | 35–45 | www.nature.com/naturemicrobiology
NATuRe MicRoBiology Review Article
51. Muytjens, C. M. J., Yu, Y. & Diamandis, E. P. Discovery of antimicrobial 78. Van de Wijgert, J. H. H. M. et al. The vaginal microbiota: what have we
peptides in cervical-vaginal fluid from healthy nonpregnant women via learned after a decade of molecular characterization? PLoS ONE 9,
an integrated proteome and peptidome analysis. Proteomics 17, e105998 (2014).
1600461 (2017). 79. MacIntyre, D. A. et al. The vaginal microbiome during pregnancy and the
52. Hiemstra, P. S., Amatngalim, G. D., van der Does, A. M. & Taube, C. postpartum period in a European population. Sci. Rep. 5, 8988 (2015).
Antimicrobial peptides and innate lung defenses: role in infectious and 80. Borgdorff, H. et al. The association between ethnicity and vaginal
noninfectious lung diseases and therapeutic applications. Chest 149, microbiota composition in Amsterdam, the Netherlands. PLoS ONE 12,
545–551 (2016). e0181135 (2017).
53. Natividad, J. M. et al. Differential induction of antimicrobial REGIII by the 81. Fettweis, J. M. et al. Differences in vaginal microbiome in African
intestinal microbiota and Bifidobacterium breve NCC2950. Appl. Environ. American women versus women of European ancestry. Microbiology 160,
Microbiol. 79, 7745–7754 (2013). 2272–2282 (2014).
54. Wong, J. M., de Souza, R., Kendall, C. W., Emam, A. & Jenkins, D. J. 82. Łaniewski, P. et al. Linking cervicovaginal immune signatures, HPV and
Colonic health: fermentation and short chain fatty acids. J. Clin. microbiota composition in cervical carcinogenesis in non-Hispanic and
Gastroenterol. 40, 235–243 (2006). Hispanic women. Sci. Rep. 8, 7593 (2018).
55. Zhao, Y. et al. GPR43 mediates microbiota metabolite SCFA regulation of 83. Redondo-Lopez, V., Cook, R. L. & Sobel, J. D. Emerging role of lactobacilli
antimicrobial peptide expression in intestinal epithelial cells via activation in the control and maintenance of the vaginal bacterial microflora. Rev.
of mTOR and STAT3. Mucosal Immunol. 11, 752–762 (2018). Infect. Dis. 12, 856–872 (1990).
56. McHan, F. & Shotts, E. B. Effect of short-chain fatty acids on the growth 84. Hillier, S. L., Krohn, M. A., Rabe, L. K., Klebanoff, S. J. & Eschenbach, D.
of Salmonella typhimurium in an in vitro system. Avian Dis. 37, A. The normal vaginal flora, H 2O2-producing lactobacilli, and bacterial
396–398 (1993). vaginosis in pregnant women. Clin. Infect. Dis. 16, S273–S281 (1993).
57. Horswill, A. R., Dudding, A. R. & Escalante-Semerena, J. C. Studies of 85. Sewankambo, N. et al. HIV-1 infection associated with abnormal vaginal
propionate toxicity in Salmonella enterica identify 2-methylcitrate as a flora morphology and bacterial vaginosis. Lancet 350, 546–550 (1997).
potent inhibitor of cell growth. J. Biol. Chem. 276, 19094–19101 (2001). 86. Gupta, K. et al. Inverse association of H2O2-producing lactobacilli and
58. Jacobson, A. et al. A gut commensal-produced metabolite mediates vaginal Escherichia coli colonization in women with recurrent urinary tract
colonization resistance to Salmonella infection. Cell Host Microbe 24, infections. J. Infect. Dis. 178, 446–450 (1998).
296–307 (2018). 87. Wiesenfeld, H. C., Hillier, S. L., Krohn, M. A., Landers, D. V. & Sweet, R. L.
59. Ricke, S. C. Perspectives on the use of organic acids and short chain fatty Bacterial vaginosis is a strong predictor of Neisseria gonorrhoeae and
acids as antimicrobials. Poult. Sci. 82, 632–639 (2003). Chlamydia trachomatis infection. Clin. Infect. Dis. 36, 663–668 (2003).
60. Hung, C. C. et al. The intestinal fatty acid propionate inhibits Salmonella 88. Lai, S. K. et al. Human immunodeficiency virus type 1 is trapped by acidic
invasion through the post-translational control of HilD. Mol. Microbiol. 87, but not by neutralized human cervicovaginal mucus. J. Virol. 83,
1045–1060 (2013). 11196–11200 (2009).
61. Gantois, I. et al. Butyrate specifically down-regulates Salmonella 89. Di Paola, M. et al. Characterization of cervico-vaginal microbiota in women
pathogenicity island 1 gene expression. Appl. Environ. Microbiol. 72, developing persistent high-risk human papillomavirus infection. Sci. Rep. 7,
946–949 (2006). 10200 (2017).
62. Hryckowian, A. J. et al. Microbiota-accessible carbohydrates suppress 90. Anahtar, M. N. et al. Cervicovaginal bacteria are a major modulator of
Clostridium difficile infection in a murine model. Nat. Microbiol. 3, host inflammatory responses in the female genital tract. Immunity 42,
662–669 (2018). 965–976 (2015).
63. Benveniste, J., Lespinats, G. & Salomon, J. Serum and secretory IgA in 91. Keller, M. J. et al. Longitudinal assessment of systemic and genital tract
axenic and holoxenic mice. J. Immunol. 107, 1656–1662 (1971). inflammatory markers and endogenous genital tract E. coli inhibitory
64. Kawamoto, S. et al. The inhibitory receptor PD-1 regulates IgA selection activity in HIV-infected and uninfected women. Am. J. Reprod. Immunol.
and bacterial composition in the gut. Science 336, 485–489 (2012). 75, 631–642 (2016).
65. Kubinak, J. L. et al. MyD88 signaling in T cells directs IgA-mediated 92. Doerflinger, S. Y., Throop, A. L. & Herbst-Kralovetz, M. M. Bacteria in the
control of the microbiota to promote health. Cell Host Microbe 17, vaginal microbiome alter the innate immune response and barrier
153–163 (2015). properties of the human vaginal epithelia in a species-specific manner.
66. Lecuyer, E. et al. Segmented filamentous bacterium uses secondary and J. Infect. Dis. 209, 1989–1999 (2014).
tertiary lymphoid tissues to induce gut IgA and specific T helper 17 cell 93. Lennard, K. et al. Microbial composition predicts genital tract inflammation
responses. Immunity 40, 608–620 (2014). and persistent bacterial vaginosis in South African adolescent females.
67. Flannigan, K. L. et al. IL-17A-mediated neutrophil recruitment limits Infect. Immun. 86, e00410–17 (2018).
expansion of segmented filamentous bacteria. Mucosal Immunol. 10, 94. Masson, L. et al. Defining genital tract cytokine signatures of sexually
673–684 (2016). transmitted infections and bacterial vaginosis in women at high risk of HIV
68. Robak, O. H. et al. Antibiotic treatment-induced secondary IgA deficiency infection: a cross-sectional study. Sex. Transm. Infect. 90, 580–587 (2014).
enhances susceptibility to Pseudomonas aeruginosa pneumonia. J. Clin. 95. Martin, H. L. et al. Vaginal lactobacilli, microbial flora, and risk of human
Invest. 128, 3535–3545 (2018). immunodeficiency virus type 1 and sexually transmitted disease acquisition.
69. Blander, J. M., Longman, R. S., Iliev, I. D., Sonnenberg, G. F. & Artis, D. J. Infect. Dis. 180, 1863–1868 (1999).
Regulation of inflammation by microbiota interactions with the host. 96. McClelland, R. S. et al. Evaluation of the association between the
Nat. Immunol. 18, 851–860 (2017). concentrations of key vaginal bacteria and the increased risk of HIV
70. Sonnenburg, J. L. & Backhed, F. Diet–microbiota interactions as moderators acquisition in African women from five cohorts: a nested case-control
of human metabolism. Nature 535, 56–64 (2016). study. Lancet Infect. Dis. 18, 554–564 (2018).
71. Verdu, E. F., Galipeau, H. J. & Jabri, B. Novel players in coeliac disease 97. Furci, L., Sironi, F., Tolazzi, M., Vassena, L. & Lusso, P. α-defensins block
pathogenesis: role of the gut microbiota. Nat. Rev. Gastroenterol. Hepatol. the early steps of HIV-1 infection: interference with the binding of gp120 to
12, 497–506 (2015). CD4. Blood 109, 2928–2935 (2007).
72. Bercik, P., Verdu, E. F. & Collins, S. M. Is irritable bowel syndrome a 98. Pace, B. T., Lackner, A. A., Porter, E. & Pahar, B. The role of defensins in
low-grade inflammatory bowel disease? Gastroenterol. Clin. North Am. 34, HIV pathogenesis. Mediators Inflamm. 2017, 5186904 (2017).
235–245 (2005). 99. Hearps, A. C. et al. Vaginal lactic acid elicits an anti-inflammatory response
73. Martin, R. et al. Faecalibacterium prausnitzii prevents physiological damages from human cervicovaginal epithelial cells and inhibits production of
in a chronic low-grade inflammation murine model. BMC Microbiol. 15, pro-inflammatory mediators associated with HIV acquisition. Mucosal
67 (2015). Immunol. 10, 1480–1490 (2017).
74. Zacho, J., Benfield, T., Tybjaerg-Hansen, A. & Nordestgaard, B. G. Increased 100. Pecora, D. V. A comparison of transtracheal aspiration with other methods
baseline C-reactive protein concentrations are associated with increased risk of determining the bacterial flora of the lower respiratory tract. N. Eng. J.
of infections: results from 2 large Danish population cohorts. Clin. Chem. Med. 269, 664–666 (1963).
62, 335–342 (2016). 101. Dickson, R. P. et al. Analysis of culture-dependent versus culture-
75. Ravel, J. et al. Vaginal microbiome of reproductive-age women. Proc. Natl independent techniques for identification of bacteria in clinically obtained
Acad. Sci. USA 108, 4680–4687 (2011). bronchoalveolar lavage fluid. J. Clin. Microbiol. 52, 3605–3613 (2014).
76. Wessels, J. M. et al. Association of high-risk sexual behaviour with diversity 102. Sibley, C. D. et al. Culture enriched molecular profiling of the cystic fibrosis
of the vaginal microbiota and abundance of Lactobacillus. PLoS ONE 12, airway microbiome. PLoS ONE 6, e22702 (2011).
e0187612 (2017). 103. Collins, A. M. et al. Bronchoalveolar lavage (BAL) for research; obtaining
77. Borgdorff, H. et al. Lactobacillus-dominated cervicovaginal microbiota adequate sample yield. J. Vis. Exp. 85, e4345 (2014).
associated with reduced HIV/STI prevalence and genital HIV viral load in 104. Human Microbiome Project Consortium. Structure, function and diversity
African women. ISME J. 8, 1781–1793 (2014). of the healthy human microbiome. Nature 486, 207–214 (2012).
Nature Microbiology | VOL 4 | JANUARY 2019 | 35–45 | www.nature.com/naturemicrobiology 43
Review Article NATuRe MicRoBiology
105. Segal, L. N. et al. Enrichment of lung microbiome with supraglottic taxa 132. Gerding, D. N. et al. Administration of spores of nontoxigenic Clostridium
is associated with increased pulmonary inflammation. Microbiome 1, difficile strain M3 for prevention of recurrent C. difficile infection: a
19 (2013). randomized clinical trial. JAMA 313, 1719–1727 (2015).
106. Dickson, R. P. et al. Spatial variation in the healthy human lung 133. Cotter, P. D., Hill, C. & Ross, R. P. Bacteriocins: developing innate
microbiome and the adapted island model of lung biogeography. Ann. Am. immunity for food. Nat. Rev. Microbiol. 3, 777–788 (2005).
Thorac. Soc. 12, 821–830 (2015). 134. Servin, A. L. Antagonistic activities of lactobacilli and bifidobacteria against
107. Hilty, M. et al. Disordered microbial communities in asthmatic airways. microbial pathogens. FEMS Microbiol. Rev. 28, 405–440 (2004).
PLoS ONE 5, e8578 (2010). 135. Mukai, T., Kaneko, S., Matsumoto, M. & Ohori, H. Binding of
108. Charlson, E. S. et al. Assessing bacterial populations in the lung by replicate Bifidobacterium bifidum and Lactobacillus reuteri to the carbohydrate
analysis of samples from the upper and lower respiratory tracts. PLoS ONE moieties of intestinal glycolipids recognized by peanut agglutinin. Int. J.
7, e42786 (2012). Food Microbiol. 90, 357–362 (2004).
109. Bassis, C. M. et al. Analysis of the upper respiratory tract microbiotas as 136. Liu, L. et al. Global, regional, and national causes of child mortality in
the source of the lung and gastric microbiotas in healthy individuals. mBio 2000–13, with projections to inform post-2015 priorities: an updated
6, e00037 (2015). systematic analysis. Lancet 385, 430–440 (2015).
110. Dickson, R. P. et al. Bacterial topography of the healthy human lower 137. Thaver, D. & Zaidi, A. K. Burden of neonatal infections in developing
respiratory tract. mBio https://doi.org/10.1128/mBio.02287-16 (2017). countries: a review of evidence from community-based studies. Pediatr.
111. Dickson, R. P. & Huffnagle, G. B. The lung microbiome: new principles Infect. Dis. J. 28, S3–S9 (2009).
for respiratory bacteriology in health and disease. PLoS Pathog. 11, 138. Panigrahi, P. et al. A randomized synbiotic trial to prevent sepsis among
e1004923 (2015). infants in rural India. Nature 548, 407–412 (2017).
112. Dickson, R. P., Erb-Downward, J. R. & Huffnagle, G. B. Homeostasis and its 139. Kassam, Z., Lee, C. H., Yuan, Y. & Hunt, R. H. Fecal microbiota
disruption in the lung microbiome. Am. J. Physiol. Lung Cell. Mol. Physiol. transplantation for Clostridium difficile infection: systematic review and
309, L1047–L1055 (2015). meta-analysis. Am. J. Gastroenterol. 108, 500–508 (2013).
113. Shenoy, M. K. et al. Immune response and mortality risk relate to distinct 140. Van Nood, E. et al. Duodenal infusion of donor feces for recurrent
lung microbiomes in patients with HIV and pneumonia. Am. J. Respir. Crit. Clostridium difficile. N. Engl. J. Med. 368, 407–415 (2013).
Care Med. 195, 104–114 (2016). 141. Manges, A. R., Steiner, T. S. & Wright, A. J. Fecal microbiota
114. Segal, L. N. et al. Enrichment of the lung microbiome with oral taxa is transplantation for the intestinal decolonization of extensively
associated with lung inflammation of a Th17 phenotype. Nat. Microbiol. 1, antimicrobial-resistant opportunistic pathogens: a review. Infect. Dis. (Lond)
16031 (2016). 48, 587–592 (2016).
115. Murdock, B. J. et al. Interleukin-17 drives pulmonary eosinophilia following 142. Khoruts, A. & Sadowsky, M. J. Understanding the mechanisms of faecal
repeated exposure to Aspergillus fumigatus conidia. Infect. Immun. 80, microbiota transplantation. Nat. Rev. Gastroenterol. Hepatol. 13,
1424–1436 (2012). 508–516 (2016).
116. Thomas, D. W. et al. Probiotics and prebiotics in pediatrics. Pediatrics 126, 143. Weingarden, A. et al. Dynamic changes in short- and long-term bacterial
1217–1231 (2010). composition following fecal microbiota transplantation for recurrent
117. Hill, C. et al. Expert consensus document. The International Scientific Clostridium difficile infection. Microbiome 3, 10 (2015).
Association for Probiotics and Prebiotics consensus statement on the scope 144. Hamilton, M. J., Weingarden, A. R., Unno, T., Khoruts, A. & Sadowsky, M.
and appropriate use of the term probiotic. Nat. Rev. Gastroenterol. Hepatol. J. High-throughput DNA sequence analysis reveals stable engraftment of
11, 506–514 (2014). gut microbiota following transplantation of previously frozen fecal bacteria.
118. Luoto, R. et al. Prebiotic and probiotic supplementation prevents rhinovirus Gut Microbes 4, 125–135 (2013).
infections in preterm infants: a randomized, placebo-controlled trial. J. 145. Seekatz, A. M. et al. Recovery of the gut microbiome following fecal
Allergy Clin. Immunol. 133, 405–413 (2014). microbiota transplantation. mBio 5, e00893-14 (2014).
119. Lohner, S., Kullenberg, D., Antes, G., Decsi, T. & Meerpohl, J. J. Prebiotics 146. Smillie, C. S. et al. Strain tracking reveals the determinants of bacterial
in healthy infants and children for prevention of acute infectious engraftment in the human gut following fecal microbiota transplantation.
diseases: a systematic review and meta-analysis. Nutr. Rev. 72, Cell Host Microbe 23, 229–240.e5 (2018).
523–531 (2014). 147. Staley, C., Kelly, C. R., Brandt, L. J., Khoruts, A. & Sadowsky, M. J.
120. Rycroft, C. E., Jones, M. R., Gibson, G. R. & Rastall, R. A. A comparative in Complete microbiota engraftment is not essential for recovery from
vitro evaluation of the fermentation properties of prebiotic oligosaccharides. recurrent Clostridium difficile infection following fecal microbiota
J. Appl. Microbiol. 91, 878–887 (2001). transplantation. mBio 7, e01965-16 (2016).
121. Marx, S. P., Winkler, S. & Hartmeier, W. Metabolization of β-(2,6)-linked 148. Ott, S. J. et al. Efficacy of sterile fecal filtrate transfer for treating patients
fructose-oligosaccharides by different bifidobacteria. FEMS Microbiol. Lett. with Clostridium difficile infection. Gastroenterology 152, 799–811.e7 (2017).
182, 163–169 (2000). 149. Zuo, T. et al. Bacteriophage transfer during faecal microbiota
122. Guigoz, Y., Rochat, F., Perruisseau-Carrier, G., Rochat, I. & Schiffrin, E. J. transplantation in Clostridium difficile infection is associated with treatment
Effects of oligosaccharide on the faecal flora and non-specific immune outcome. Gut 67, 634–643 (2018).
system in elderly people. Nutr. Res. 22, 13–25 (2002). 150. Morton, E. R. et al. Variation in rural African gut microbiota is strongly
123. Koga, Y. et al. Age-associated effect of kestose on Faecalibacterium correlated with colonization by Entamoeba and subsistence. PLoS Genet. 11,
prausnitzii and symptoms in the atopic dermatitis infants. Pediatr. Res. 80, e1005658 (2015).
844–851 (2016). 151. Gilchrist, C. A. et al. Role of the gut microbiota of children in diarrhea due
124. Pokusaeva, K., Fitzgerald, G. F. & van Sinderen, D. Carbohydrate to the protozoan parasite Entamoeba histolytica. J. Infect. Dis. 213,
metabolism in Bifidobacteria. Genes Nutr. 6, 285–306 (2011). 1579–1585 (2016).
125. Pan, X.-D., Chen, F.-Q., Wu, T.-X., Tang, H.-G. & Zhao, Z.-Y. Prebiotic 152. Burgess, S. L., Gilchrist, C. A., Lynn, T. C. & Petri, W. A. Jr Parasitic
oligosaccharides change the concentrations of short-chain fatty acids and protozoa and interactions with the host intestinal microbiota. Infect.
the microbial population of mouse bowel. J. Zhejiang. Univ. Sci. B 10, Immun. 85, e00101–17 (2017).
258–263 (2009). 153. Sui, Y. et al. Influence of gut microbiome on mucosal immune activation
126. Correa-Oliveira, R., Fachi, J. L., Vieira, A., Sato, F. T. & Vinolo, M. A. and SHIV viral transmission in naive macaques. Mucosal Immunol. 11,
Regulation of immune cell function by short-chain fatty acids. Clin. Transl. 1219–1229 (2018).
Immunol. 5, e73 (2016). 154. Dillon, S. M. et al. An altered intestinal mucosal microbiome in HIV-1
127. Maslowski, K. M. et al. Regulation of inflammatory responses by gut infection is associated with mucosal and systemic immune activation and
microbiota and chemoattractant receptor GPR43. Nature 461, endotoxemia. Mucosal Immunol. 7, 983–994 (2014).
1282–1286 (2009). 155. Ichinohe, T. et al. Microbiota regulates immune defense against respiratory
128. Venkataraman, A. et al. Variable responses of human microbiomes to tract influenza A virus infection. Proc. Natl Acad. Sci. USA 108,
dietary supplementation with resistant starch. Microbiome 4, 33 (2016). 5354–5359 (2011).
129. Kunz, C., Rudloff, S., Baier, W., Klein, N. & Strobel, S. Oligosaccharides in 156. Rudner, X. L., Happel, K. I., Young, E. A. & Shellito, J. E. Interleukin-23
human milk: structural, functional, and metabolic aspects. Annu. Rev. Nutr. (IL-23)-IL-17 cytokine axis in murine Pneumocystis carinii infection. Infect.
20, 699–722 (2000). Immun. 75, 3055–3061 (2007).
130. Shoaf, K., Mulvey, G. L., Armstrong, G. D. & Hutkins, R. W. Prebiotic 157. Lukacs, N. W. et al. Respiratory virus-induced TLR7 activation controls
galactooligosaccharides reduce adherence of enteropathogenic Escherichia IL-17-associated increased mucus via IL-23 regulation. J. Immunol. 185,
coli to tissue culture cells. Infect. Immun. 74, 6920–6928 (2006). 2231–2239 (2010).
131. Zhang, K. et al. The non-toxigenic Clostridium difficile CD37 protects mice 158. Jespers, V. et al. A longitudinal analysis of the vaginal microbiota and
against infection with a BI/NAP1/027 type of C. difficile strain. Anaerobe vaginal immune mediators in women from sub-Saharan Africa. Sci. Rep. 7,
36, 49–52 (2015). 11974 (2017).
44 Nature Microbiology | VOL 4 | JANUARY 2019 | 35–45 | www.nature.com/naturemicrobiology
NATuRe MicRoBiology Review Article
159. Gosmann, C. et al. Lactobacillus-deficient cervicovaginal bacterial Author contributions
communities are associated with increased HIV acquisition in young South All authors contributed to the conceptualization, writing and preparation of this
African women. Immunity 46, 29–37 (2017). manuscript, as well as the creation of the figures.
160. Christensen-Quick, A. et al. Human Th17 cells lack HIV-inhibitory RNases
and are highly permissive to productive HIV infection. J. Virol. 90,
7833–7847 (2016). Competing interests
161. Prescott, S. L. History of medicine: origin of the term microbiome and why The authors declare no competing interests.
it matters. Hum. Microbiome J. 4, 24–25 (2017).
Additional information
Acknowledgements Reprints and permissions information is available at www.nature.com/reprints.
The authors thank D. R. Hill, K. Rao and C. M. Bassis for helpful feedback on earlier Correspondence should be addressed to V.B.Y.
versions of this manuscript, and D. R. Hill for many helpful conversations regarding
this manuscript. This work was supported by a grant awarded to V.B.Y. from the Publisher’s note: Springer Nature remains neutral with regard to jurisdictional claims in
National Institute of Allergy and Infectious Diseases at the National Institutes of Health published maps and institutional affiliations.
(U01-AI124255). © Springer Nature Limited 2018
Nature Microbiology | VOL 4 | JANUARY 2019 | 35–45 | www.nature.com/naturemicrobiology 45
You might also like
- Actividad 8 Artículo 4.Document7 pagesActividad 8 Artículo 4.byronNo ratings yet
- Actividad 6 Artículo 3Document32 pagesActividad 6 Artículo 3byronNo ratings yet
- Actividad 8 Artículo 4.Document7 pagesActividad 8 Artículo 4.byronNo ratings yet
- Articulo 7 YersineaDocument14 pagesArticulo 7 YersineabyronNo ratings yet
- Actividad 14 Artículo 6Document6 pagesActividad 14 Artículo 6byronNo ratings yet
- Actividad 4 Artículo 2Document11 pagesActividad 4 Artículo 2byronNo ratings yet
- Actividad 2 Artículo 1Document10 pagesActividad 2 Artículo 1byronNo ratings yet
- Actividad 14 Artículo 6Document6 pagesActividad 14 Artículo 6byronNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (120)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Nisani Et Al. 2007 RGENERAÇÃODocument5 pagesNisani Et Al. 2007 RGENERAÇÃOMarilia BorgesNo ratings yet
- TH THDocument12 pagesTH THchn pastranaNo ratings yet
- Sir David Cuthbertson Medal Lecture - Fluid, Electrolytes and Nutrition: Physiological and Clinical AspectsDocument15 pagesSir David Cuthbertson Medal Lecture - Fluid, Electrolytes and Nutrition: Physiological and Clinical AspectsThinh VinhNo ratings yet
- Icterus Neonatorum/ Jaundice: 07/12/2021 Rupinder DeolDocument83 pagesIcterus Neonatorum/ Jaundice: 07/12/2021 Rupinder DeolShivangi SharmaNo ratings yet
- Physiology of MenopauseDocument20 pagesPhysiology of Menopauseindriyani makmunNo ratings yet
- Filum Nematoda 2022Document45 pagesFilum Nematoda 2022RenjunNo ratings yet
- Biochemistry MCQsDocument18 pagesBiochemistry MCQsMUHAMMAD NAEEM IQBALNo ratings yet
- The Cerebrum - Lobes - Vasculature - TeachMeAnatomyDocument3 pagesThe Cerebrum - Lobes - Vasculature - TeachMeAnatomywzt2001No ratings yet
- Grade 12 General Biology I Quarter 2 Module 2 For StudentsDocument12 pagesGrade 12 General Biology I Quarter 2 Module 2 For StudentsStar DustNo ratings yet
- Phys 5.2 Resp Lung VolumesDocument9 pagesPhys 5.2 Resp Lung VolumesRama Devi DusiNo ratings yet
- 10th Name The Following BiologyDocument11 pages10th Name The Following BiologyManoj ThakurNo ratings yet
- ProteaseDocument18 pagesProteasePriyaNo ratings yet
- Anatomy and Physiology An Integrative Approach 2nd Edition Mckinley Solutions ManualDocument24 pagesAnatomy and Physiology An Integrative Approach 2nd Edition Mckinley Solutions ManualThomasSanderspfcq100% (43)
- Psychology in Practice - Environment PDFDocument252 pagesPsychology in Practice - Environment PDFThilluNo ratings yet
- Intra-Body Nano-Network - Brief Summary by Mik AndersenDocument24 pagesIntra-Body Nano-Network - Brief Summary by Mik AndersenGuilherme UnityNo ratings yet
- Extracorporeal Life Support For TraumaDocument12 pagesExtracorporeal Life Support For TraumaBruce Fredy Chino ChambillaNo ratings yet
- Introduction To SpeechDocument22 pagesIntroduction To SpeechJoe AjibadeNo ratings yet
- Markscheme: (209 Marks)Document24 pagesMarkscheme: (209 Marks)Michael WangNo ratings yet
- Embryology MCQDocument10 pagesEmbryology MCQTofik MohammedNo ratings yet
- Photosynthesis WorksheetDocument3 pagesPhotosynthesis WorksheetByambazaya E100% (2)
- Photosynthesiscombinedpogil 3Document9 pagesPhotosynthesiscombinedpogil 3Shaojie HeNo ratings yet
- Anaphylactic Death FinalDocument73 pagesAnaphylactic Death Finalkhaled eissaNo ratings yet
- Centurion University of Technology & Management Andhra Pradesh Examination CellDocument19 pagesCenturion University of Technology & Management Andhra Pradesh Examination Cell......No ratings yet
- Forward Head Posture Affects Your BrainDocument4 pagesForward Head Posture Affects Your Brainchandni saxenaNo ratings yet
- M 1 PPT-PDF XI Bio CH 7 Structural Organisation in AnimalsDocument39 pagesM 1 PPT-PDF XI Bio CH 7 Structural Organisation in Animalsamarendrar87No ratings yet
- NEB Biology Syllabus XI & XIIDocument26 pagesNEB Biology Syllabus XI & XIIBhanu AryalNo ratings yet
- National Cancer Institute 268/1 Rama 6 Road Thung Phaya Thai, Ratchathewi, Bangkok 10400 Tel. 02-202-6800, 02-202-6888Document2 pagesNational Cancer Institute 268/1 Rama 6 Road Thung Phaya Thai, Ratchathewi, Bangkok 10400 Tel. 02-202-6800, 02-202-6888Choo HokiertiNo ratings yet
- 7 Human Nutrition (Notes)Document20 pages7 Human Nutrition (Notes)Maya YazalNo ratings yet
- PT 1 QP Biology Grade 12Document5 pagesPT 1 QP Biology Grade 12Aniruddha KadamNo ratings yet
- Lesson 1 DepEd Guidelines On Instructional PlanningDocument9 pagesLesson 1 DepEd Guidelines On Instructional PlanningJeanmae Omalyao MakilingNo ratings yet