You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
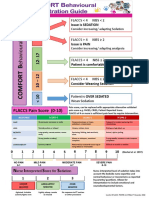
- FLACCS Pain Score (0-10) : N I S SDocument2 pagesFLACCS Pain Score (0-10) : N I S SareviamdNo ratings yet
- Intimate Partner Violence, Depression, and Child Growth and DevelopmentDocument12 pagesIntimate Partner Violence, Depression, and Child Growth and DevelopmentareviamdNo ratings yet
- Prpanolol PTSDDocument7 pagesPrpanolol PTSDareviamdNo ratings yet
- What Is Scored?: 2 Minute ObservationDocument16 pagesWhat Is Scored?: 2 Minute ObservationareviamdNo ratings yet
- Community-Acquired Pneumonia Among Children: The Latest Evidence For An Updated ManagementDocument10 pagesCommunity-Acquired Pneumonia Among Children: The Latest Evidence For An Updated ManagementareviamdNo ratings yet
- Nutrients: Ffects of Lactobacillus Plantarum PS128 OnDocument16 pagesNutrients: Ffects of Lactobacillus Plantarum PS128 OnareviamdNo ratings yet
- Efek Telp SmsDocument8 pagesEfek Telp SmsareviamdNo ratings yet
- Prpanolol PTSDDocument7 pagesPrpanolol PTSDareviamdNo ratings yet
- Telaah Kritis Artikel Review SistematikDocument4 pagesTelaah Kritis Artikel Review SistematikNorbertus MacekaNo ratings yet
- Agustini Utari - CAH in Limited Resources AreaDocument28 pagesAgustini Utari - CAH in Limited Resources AreaEnny AndrianiNo ratings yet
- PedsQL-3.0-Satisfaction For HO - AU3.0 - eng-USoriDocument4 pagesPedsQL-3.0-Satisfaction For HO - AU3.0 - eng-USoriareviamdNo ratings yet
- Achmad Rafli - Increasing Immunization Coverage PDFDocument40 pagesAchmad Rafli - Increasing Immunization Coverage PDFKaze GifNo ratings yet
- Sand PlayDocument12 pagesSand PlayareviamdNo ratings yet
- Sand PlayDocument12 pagesSand PlayareviamdNo ratings yet
- IKM Research PDFDocument119 pagesIKM Research PDFAlbertnego AndrowmedhasitepuNo ratings yet
- HW5Document4 pagesHW5Karthik GanesuniNo ratings yet
- Kualitatif-Blok 3.1-2014-Sesi Analisis data-AUDocument22 pagesKualitatif-Blok 3.1-2014-Sesi Analisis data-AUareviamdNo ratings yet
- Journal Nefro 5 PDFDocument13 pagesJournal Nefro 5 PDFAndhika Aryandhie DwiputraNo ratings yet
- Vit D Nephrotic SyndromDocument11 pagesVit D Nephrotic SyndromareviamdNo ratings yet
- OR RR DLL PDFDocument5 pagesOR RR DLL PDFYoga YudhistiraNo ratings yet
- Abeyagunawardena 2017Document6 pagesAbeyagunawardena 2017Rolando AgustianNo ratings yet
- Banerjee 2017Document8 pagesBanerjee 2017srildaNo ratings yet
- Lerch 2018Document10 pagesLerch 2018areviamdNo ratings yet
- Cohen 2017Document19 pagesCohen 2017areviamdNo ratings yet
- Efficacy Rituximab Vs Tacrolimus NSDocument8 pagesEfficacy Rituximab Vs Tacrolimus NSareviamdNo ratings yet
- Evaluasi DengueDocument9 pagesEvaluasi DengueareviamdNo ratings yet
- Vit D Nephrotic SyndromDocument11 pagesVit D Nephrotic SyndromareviamdNo ratings yet
- Kompilasi Materi Pembicara 1-4 Webinar iLA-PERDICI - v2Document208 pagesKompilasi Materi Pembicara 1-4 Webinar iLA-PERDICI - v2areviamdNo ratings yet
- Assesmen Nyeri PAPDocument3 pagesAssesmen Nyeri PAPareviamdNo ratings yet
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Data Pasien TB JuliDocument42 pagesData Pasien TB JuliTsubbatun NajahNo ratings yet
- 11 10 2014Document14 pages11 10 2014Alaa DarwishNo ratings yet
- Functional Food DevelopmentDocument11 pagesFunctional Food Developmentlaura restrepoNo ratings yet
- Problems of Elder AbuseDocument13 pagesProblems of Elder AbuseNeha Jayaraman100% (3)
- Department of Labor: OWCP-915Document2 pagesDepartment of Labor: OWCP-915USA_DepartmentOfLaborNo ratings yet
- Activity 6 - SummarizingDocument6 pagesActivity 6 - SummarizingAntolin AguirreNo ratings yet
- Human Services Homeless PPT FinalDocument26 pagesHuman Services Homeless PPT Finalal_crespoNo ratings yet
- Compliance and Therapy Report 01312023 114720 PDFDocument2 pagesCompliance and Therapy Report 01312023 114720 PDFCristinaLucanNo ratings yet
- Nandini PDFDocument7 pagesNandini PDFJustine LopezNo ratings yet
- MEDI7241 How To Write A Research Protocol TutorialDocument7 pagesMEDI7241 How To Write A Research Protocol TutorialJazradelNo ratings yet
- ILOILO DOCTORS’ COLLEGE COLLEGE OF NURSING Ferrous SulfateDocument2 pagesILOILO DOCTORS’ COLLEGE COLLEGE OF NURSING Ferrous SulfatePauline AnesNo ratings yet
- Intensive Care UnitDocument26 pagesIntensive Care Unitpdamodar2007No ratings yet
- Annex To The European Commission Guideline On Excipients in The Labelling and Package Leaflet of Medicinal Products For Human Use' (2019)Document21 pagesAnnex To The European Commission Guideline On Excipients in The Labelling and Package Leaflet of Medicinal Products For Human Use' (2019)janoscribdNo ratings yet
- ICH Good Clinical Practice GuidelinesDocument4 pagesICH Good Clinical Practice GuidelinesJagadish BabuNo ratings yet
- Seamless Care - DR SH LeungDocument38 pagesSeamless Care - DR SH Leungmalaysianhospicecouncil6240No ratings yet
- Wound Healing Rate of Buddha Belly Leaf ThesisDocument25 pagesWound Healing Rate of Buddha Belly Leaf ThesisJoyce Lee100% (2)
- VetMed Week Souvenir Program February 18-22, 2013Document20 pagesVetMed Week Souvenir Program February 18-22, 2013baruruydNo ratings yet
- Prevent and Reduce Neck Stiffness Caused by RTDocument9 pagesPrevent and Reduce Neck Stiffness Caused by RTaurika sinambelaNo ratings yet
- Understanding Kundalini Energy and its Role in Spiritual EvolutionDocument190 pagesUnderstanding Kundalini Energy and its Role in Spiritual Evolutionnityanandroy100% (1)
- The Nursing Assessment of Peptic UlcerDocument14 pagesThe Nursing Assessment of Peptic UlcerVelia suwandiNo ratings yet
- Kinds of Diseases: Name: Rebekha Noveria NPM: 18.11.124 PSIK 3.1Document12 pagesKinds of Diseases: Name: Rebekha Noveria NPM: 18.11.124 PSIK 3.1Rebekha Noveria SitumorangNo ratings yet
- Dikamali (Gardenia Resinifera Roth.) : G. Latifolia G. Resinifera G. TurgidaDocument6 pagesDikamali (Gardenia Resinifera Roth.) : G. Latifolia G. Resinifera G. TurgidaPrajakta RaneNo ratings yet
- AnnouncementDocument2 pagesAnnouncementArianne Katrina CoballesNo ratings yet
- Data Obat Terjual Jan-Des 2018Document62 pagesData Obat Terjual Jan-Des 2018HanNo ratings yet
- The Scholar Class v1.0.1 FREEDocument7 pagesThe Scholar Class v1.0.1 FREEBreno SouzaNo ratings yet
- Symposium Topic: Current Update in Diagnosis & Management of Emergency MedicineDocument2 pagesSymposium Topic: Current Update in Diagnosis & Management of Emergency MedicineAfriza AnggriniNo ratings yet
- MTF Surgery KitDocument33 pagesMTF Surgery KitCarolyn Samuels75% (4)
- 06-Otter (623-636)Document14 pages06-Otter (623-636)ronie redsNo ratings yet
- CSSD Forums Sop 20120716 enDocument73 pagesCSSD Forums Sop 20120716 enNeil Osborne100% (1)
- Uganda Universities and Courses For Student Loan SupportDocument5 pagesUganda Universities and Courses For Student Loan SupportThe Campus TimesNo ratings yet