You might also like
- Exercise and Bariatric SurgeryDocument9 pagesExercise and Bariatric SurgeryDusan OrescaninNo ratings yet
- The Dresden Protocol For Multidimensional Walking Assessment (DMWA) in Clinical PracticeDocument15 pagesThe Dresden Protocol For Multidimensional Walking Assessment (DMWA) in Clinical PracticeMari PaoNo ratings yet
- Does Gait Speed Contribute To Sarcopenia Case-Finding in A PostacuteDocument18 pagesDoes Gait Speed Contribute To Sarcopenia Case-Finding in A PostacuteMari PaoNo ratings yet
- Early MobilizationDocument8 pagesEarly MobilizationMari PaoNo ratings yet
- Exercise and Bariatric SurgeryDocument9 pagesExercise and Bariatric SurgeryDusan OrescaninNo ratings yet
- An Electromyographic Analysis of Commercial and CoDocument15 pagesAn Electromyographic Analysis of Commercial and CoMari PaoNo ratings yet
- Effects of Integrative Core Stability Training OnDocument15 pagesEffects of Integrative Core Stability Training OnMari PaoNo ratings yet
- Associations Between Functional Fitness and Walking Speed in Older AdultsDocument5 pagesAssociations Between Functional Fitness and Walking Speed in Older AdultsMari PaoNo ratings yet
- 2018JAGSJung Et Al-2018-Journal of The American Geriatrics SocietyDocument5 pages2018JAGSJung Et Al-2018-Journal of The American Geriatrics SocietyMari PaoNo ratings yet
- Bajar de Peso Hit Vrs Continuo AnalisisDocument1 pageBajar de Peso Hit Vrs Continuo AnalisisMari PaoNo ratings yet
- Assessing The Walking Speed ofDocument6 pagesAssessing The Walking Speed ofMari PaoNo ratings yet
- 6th Vital Sign AppDocument25 pages6th Vital Sign AppMari PaoNo ratings yet
- A Global Clinical Measure of Fitness and FrailtyDocument7 pagesA Global Clinical Measure of Fitness and FrailtyMari PaoNo ratings yet
- The Role of Exercise-Induced Myokines in Regulating MetabolismDocument16 pagesThe Role of Exercise-Induced Myokines in Regulating MetabolismMari PaoNo ratings yet
- Effects of Different Exercise Interventions On Risk of Falls, Gait Ability, andDocument11 pagesEffects of Different Exercise Interventions On Risk of Falls, Gait Ability, andMari PaoNo ratings yet
- Oa Puede El Ejercicio RpevenirDocument2 pagesOa Puede El Ejercicio RpevenirMari PaoNo ratings yet
- Writing More Specific Exercise PrescriptionsDocument2 pagesWriting More Specific Exercise PrescriptionsMari PaoNo ratings yet
- 1 s2.0 S2352873717300252 MainDocument10 pages1 s2.0 S2352873717300252 MainMari PaoNo ratings yet
- Exercise Timing and Circadian RhythmsDocument6 pagesExercise Timing and Circadian RhythmsMari PaoNo ratings yet
- Crosstalk Between Adipokines and Myokines in FatDocument20 pagesCrosstalk Between Adipokines and Myokines in FatMari PaoNo ratings yet
- Sedentary Behavior, Exercise, and Cardiovascular Health: ReviewDocument17 pagesSedentary Behavior, Exercise, and Cardiovascular Health: ReviewMari PaoNo ratings yet
- Effects of A 4-Week Multicomponent Exercise ProgramDocument8 pagesEffects of A 4-Week Multicomponent Exercise ProgramMari PaoNo ratings yet
- Inactivity and Skeletal Muscle Metabolism: A Vicious Cycle in Old AgeDocument21 pagesInactivity and Skeletal Muscle Metabolism: A Vicious Cycle in Old AgeMari PaoNo ratings yet
- Recovery After ExerciseDocument10 pagesRecovery After ExerciseMari PaoNo ratings yet
- An Evidence Based Approach ForDocument15 pagesAn Evidence Based Approach ForDanilo Andres Silva EsparzaNo ratings yet
- The Scientific Basis For Recovery Training Practices in SportDocument63 pagesThe Scientific Basis For Recovery Training Practices in SportMari PaoNo ratings yet
- MSSE-Central Peripheral Fatigue InteractionDocument7 pagesMSSE-Central Peripheral Fatigue InteractionMari PaoNo ratings yet
- Efficacy of A Land-Based Home Exercise programME For PDFDocument6 pagesEfficacy of A Land-Based Home Exercise programME For PDFMari PaoNo ratings yet
- Post-Exercise Recovery Strategies in Basketball: Practical Applications Based On Scientific EvidenceDocument17 pagesPost-Exercise Recovery Strategies in Basketball: Practical Applications Based On Scientific EvidenceMari PaoNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Teralight ProfileDocument12 pagesTeralight ProfileMohammed TariqNo ratings yet
- 1.functional Specification PTP With EDIDocument36 pages1.functional Specification PTP With EDIAnil Kumar100% (4)
- INTERNATIONAL BUSINESS DYNAMIC (Global Operation MGT)Document7 pagesINTERNATIONAL BUSINESS DYNAMIC (Global Operation MGT)Shashank DurgeNo ratings yet
- Ucbackup Faq - Commvault: GeneralDocument8 pagesUcbackup Faq - Commvault: GeneralhherNo ratings yet
- Planas V Comelec - FinalDocument2 pagesPlanas V Comelec - FinalEdwino Nudo Barbosa Jr.100% (1)
- QuestionDocument7 pagesQuestionNgọc LuânNo ratings yet
- Reading TPO 49 Used June 17 To 20 10am To 12pm Small Group Tutoring1Document27 pagesReading TPO 49 Used June 17 To 20 10am To 12pm Small Group Tutoring1shehla khanNo ratings yet
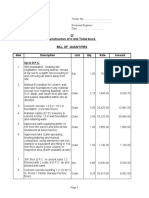
- Type BOQ For Construction of 4 Units Toilet Drawing No.04Document6 pagesType BOQ For Construction of 4 Units Toilet Drawing No.04Yashika Bhathiya JayasingheNo ratings yet
- R 18 Model B Installation of TC Auxiliary Lights and WingletsDocument29 pagesR 18 Model B Installation of TC Auxiliary Lights and WingletsAlejandro RodríguezNo ratings yet
- Perpetual InjunctionsDocument28 pagesPerpetual InjunctionsShubh MahalwarNo ratings yet
- 7933-Article Text-35363-1-10-20230724Document8 pages7933-Article Text-35363-1-10-20230724Ridho HidayatNo ratings yet
- ACC403 Week 10 Assignment Rebecca MillerDocument7 pagesACC403 Week 10 Assignment Rebecca MillerRebecca Miller HorneNo ratings yet
- Cencon Atm Security Lock Installation InstructionsDocument24 pagesCencon Atm Security Lock Installation InstructionsbiggusxNo ratings yet
- Omae2008 57495Document6 pagesOmae2008 57495Vinicius Cantarino CurcinoNo ratings yet
- TENDER DOSSIER - Odweyne Water PanDocument15 pagesTENDER DOSSIER - Odweyne Water PanMukhtar Case2022No ratings yet
- Fcode 54 en El SytucDocument2 pagesFcode 54 en El SytucAga MenonNo ratings yet
- Government of India Act 1858Document3 pagesGovernment of India Act 1858AlexitoNo ratings yet
- AdvertisingDocument2 pagesAdvertisingJelena ŽužaNo ratings yet
- Chapter 11 Walter Nicholson Microcenomic TheoryDocument15 pagesChapter 11 Walter Nicholson Microcenomic TheoryUmair QaziNo ratings yet
- Safety Inspection Checklist Project: Location: Inspector: DateDocument2 pagesSafety Inspection Checklist Project: Location: Inspector: Dateyono DaryonoNo ratings yet
- Mutual Fund Insight Nov 2022Document214 pagesMutual Fund Insight Nov 2022Sonic LabelsNo ratings yet
- Press Release - INTRODUCING THE NEW LAND ROVER DEFENDER PDFDocument6 pagesPress Release - INTRODUCING THE NEW LAND ROVER DEFENDER PDFJay ShahNo ratings yet
- Relay Interface ModulesDocument2 pagesRelay Interface Modulesmahdi aghamohamadiNo ratings yet
- Software Hackathon Problem StatementsDocument2 pagesSoftware Hackathon Problem StatementsLinusNelson100% (2)
- U2 - Week1 PDFDocument7 pagesU2 - Week1 PDFJUANITO MARINONo ratings yet
- Faida WTP - Control PhilosophyDocument19 pagesFaida WTP - Control PhilosophyDelshad DuhokiNo ratings yet
- Mix Cases UploadDocument4 pagesMix Cases UploadLu CasNo ratings yet
- Corporation Law Review Test Midterms 2019Document4 pagesCorporation Law Review Test Midterms 2019Van NessaNo ratings yet
- Gathering Package 2023Document2 pagesGathering Package 2023Sudiantara abasNo ratings yet
- Central Banking and Monetary PolicyDocument13 pagesCentral Banking and Monetary PolicyLuisaNo ratings yet