You might also like
- A Simple Guide to Facial Palsy, Diagnosis, Treatment, and Related ConditionsFrom EverandA Simple Guide to Facial Palsy, Diagnosis, Treatment, and Related ConditionsNo ratings yet
- Drooping Eyelid, (Ptosis) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandDrooping Eyelid, (Ptosis) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Bell's Palsy Treatment RecoveryDocument5 pagesBell's Palsy Treatment RecoverymelatiNo ratings yet
- Bell's Palsy Drooling Excessive Tearing: Common CausesDocument3 pagesBell's Palsy Drooling Excessive Tearing: Common CausessmilingforeverNo ratings yet
- Pareza FacialaDocument1 pagePareza FacialaStefanNo ratings yet
- Facial InjuriesDocument6 pagesFacial Injuriesmicheal1960No ratings yet
- SeizureDocument4 pagesSeizureremjith rajendranNo ratings yet
- Bell'S Palsy: Villanueva, Relyssa Ashley L. BSNDocument6 pagesBell'S Palsy: Villanueva, Relyssa Ashley L. BSNAshley VillanuevaNo ratings yet
- Bell' Palsy - PPT Report - PPT FINALDocument21 pagesBell' Palsy - PPT Report - PPT FINALCarshena Cuares100% (1)
- Jps R 07111519Document3 pagesJps R 07111519Riuin23No ratings yet
- Neurophysiology: CASE 4-1Document17 pagesNeurophysiology: CASE 4-1shestrelmay l umingaNo ratings yet
- Tata Laksana Bells PalsyDocument4 pagesTata Laksana Bells PalsyYoan ChouNo ratings yet
- Differentiate between facial palsy and Bell's palsyDocument19 pagesDifferentiate between facial palsy and Bell's palsyAya AmerNo ratings yet
- Bell Palsy: Clinical Examination and Management: ReviewDocument8 pagesBell Palsy: Clinical Examination and Management: ReviewCitraNo ratings yet
- Bell - S PalsyDocument17 pagesBell - S PalsyRickzen Hawkins NikecholantNo ratings yet
- Bell's Palsy Facial Paralysis GuideDocument6 pagesBell's Palsy Facial Paralysis GuidelauNo ratings yet
- Bell's Palsy Treatment and ManagementDocument15 pagesBell's Palsy Treatment and ManagementDavid MharkNo ratings yet
- Bell's Palsy - Johns Hopkins MedicineDocument5 pagesBell's Palsy - Johns Hopkins MedicineRoxan PacsayNo ratings yet
- Bell S Palsy Case StudyDocument4 pagesBell S Palsy Case StudyJAN ACCEL PAGADUANNo ratings yet
- Bell's Palsy: Causes, Signs, Symptoms and TreatmentDocument10 pagesBell's Palsy: Causes, Signs, Symptoms and Treatmentjennifer helligerNo ratings yet
- Bell's Palsy Guide: Causes, Symptoms, Diagnosis and TreatmentDocument22 pagesBell's Palsy Guide: Causes, Symptoms, Diagnosis and TreatmentRizky AmaLia Ar-RosyidNo ratings yet
- Bell's Palsy: Submitted By: Twinkle Singh & Kinjalika VarmaDocument34 pagesBell's Palsy: Submitted By: Twinkle Singh & Kinjalika Varmatwinklestar1396No ratings yet
- Bell's PalsyDocument46 pagesBell's PalsySanjeet SahNo ratings yet
- Causes of PtosisDocument3 pagesCauses of PtosisHenry Jonathan BadongenNo ratings yet
- Inner Ear Balance ProblemsDocument6 pagesInner Ear Balance ProblemsaleiyoNo ratings yet
- Treatment of Bell's PalsyDocument5 pagesTreatment of Bell's Palsymaryrose_jordanNo ratings yet
- Presenting Complaint: Patient's ResponseDocument5 pagesPresenting Complaint: Patient's ResponseGabriella PatriciaNo ratings yet
- Facial MusclesDocument26 pagesFacial MusclesAdel Yousef JaffalNo ratings yet
- Facial Nerve Paralysis 2Document44 pagesFacial Nerve Paralysis 2Omowole GbengaNo ratings yet
- Bell'sDocument2 pagesBell'sEden RamosNo ratings yet
- TLC Noah HeerDocument3 pagesTLC Noah HeerAlain SalsaMan BazilNo ratings yet
- Facial Palsy v7Document6 pagesFacial Palsy v7Link FosterNo ratings yet
- Bell's Palsy Is A Type of Facial Paralysis That Results in An Inability ToDocument2 pagesBell's Palsy Is A Type of Facial Paralysis That Results in An Inability Touvwevewvwvevwve ossasNo ratings yet
- The Anaphylactic ShockDocument8 pagesThe Anaphylactic ShockRooby JeanpierreNo ratings yet
- Palsy: What Is Bel's Palsy?Document3 pagesPalsy: What Is Bel's Palsy?sbb anbwNo ratings yet
- Siti Nur Haliza - Farmasi 1B - Task 1Document6 pagesSiti Nur Haliza - Farmasi 1B - Task 1Gio ArgyandraNo ratings yet
- Bell's palsy facial paralysis causesDocument30 pagesBell's palsy facial paralysis causesApril Grace Loredo0% (1)
- Presentation Cranial Nerve DisordersDocument30 pagesPresentation Cranial Nerve DisordersSania SaeedNo ratings yet
- Mouth Breathing, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandMouth Breathing, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsRating: 4 out of 5 stars4/5 (1)
- Bell PalsyDocument1 pageBell PalsyMarcus PiroteNo ratings yet
- Research Paper On Bells PalsyDocument5 pagesResearch Paper On Bells Palsyklbndecnd100% (1)
- Anaphy 2Document2 pagesAnaphy 2Chan ChanNo ratings yet
- Adult Glasgow Coma Scale: Traumatic Brain InjuryDocument5 pagesAdult Glasgow Coma Scale: Traumatic Brain InjuryJessica AdhykaNo ratings yet
- Thesis On Facial PalsyDocument8 pagesThesis On Facial Palsymelissalongmanchester100% (2)
- Drooling, (Sialorrhea) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandDrooling, (Sialorrhea) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Cervoni2017 4Document5 pagesCervoni2017 4ekanovicaNo ratings yet
- Ted PDFDocument3 pagesTed PDFxuexueNo ratings yet
- Bell's PalsyDocument37 pagesBell's PalsyobligatraftelNo ratings yet
- PrintDocument32 pagesPrintnewtonNo ratings yet
- Nine Effective Home Remedies For EaracheDocument1 pageNine Effective Home Remedies For EarachekaralyntNo ratings yet
- Meeting Special Needs: A practical guide to support children with EpilepsyFrom EverandMeeting Special Needs: A practical guide to support children with EpilepsyNo ratings yet
- Breath Holding SpellDocument3 pagesBreath Holding SpellDimas Alphiano100% (1)
- Seizure DisorderDocument8 pagesSeizure Disorderapi-397871513No ratings yet
- Head Injuries FAST CheckDocument20 pagesHead Injuries FAST CheckCasper ScholesNo ratings yet
- Bell's Palsy Fact Sheet - National Institute of Neurological Disorders and StrokeDocument5 pagesBell's Palsy Fact Sheet - National Institute of Neurological Disorders and StrokeRoxan PacsayNo ratings yet
- Nursing Care Plan For GlaucomaDocument2 pagesNursing Care Plan For GlaucomaEmiey Rara100% (1)
- Bells PalsyDocument32 pagesBells PalsymallikmcNo ratings yet
- Bells PalsyDocument2 pagesBells PalsyJhevilin RMNo ratings yet
- Bells palsy facial paralysis treatment and prognosisDocument19 pagesBells palsy facial paralysis treatment and prognosishessty100% (1)
- Alzheimer, AloisDocument11 pagesAlzheimer, AloisInternational Brain Research OrganizationNo ratings yet
- LSEBN Caring For Your Burn at Home CWDocument36 pagesLSEBN Caring For Your Burn at Home CWjeundeuki kimNo ratings yet
- Wound Dressing GuideDocument2 pagesWound Dressing Guidekitsil100% (7)
- Salbutamol Therapy For Food Impaction In.34Document1 pageSalbutamol Therapy For Food Impaction In.34Ana Clara ReisNo ratings yet
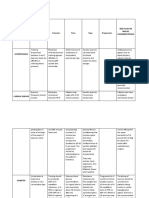
- Medical Conditions Frequency Intensity Time Type Progression Red Flags or Special ConsideratrionsDocument4 pagesMedical Conditions Frequency Intensity Time Type Progression Red Flags or Special ConsideratrionsClaire Madriaga GidoNo ratings yet
- Microbiology OSPE DocumentDocument12 pagesMicrobiology OSPE Documentj.l.sathwik7117No ratings yet
- NURSING CARE PLAN - Risk For Fluid Volume DeficitDocument2 pagesNURSING CARE PLAN - Risk For Fluid Volume DeficitDaniel Andre S. SomorayNo ratings yet
- General Surgery ReviewerDocument38 pagesGeneral Surgery ReviewerTabs NuñezNo ratings yet
- Nursing care plan for patient with meningiomaDocument3 pagesNursing care plan for patient with meningiomaShaira TillahNo ratings yet
- Impaired Physical MobilityDocument3 pagesImpaired Physical MobilityCalimlim Kim100% (1)
- Overview of Pediatrics Notes (Dr. Bongalo)Document3 pagesOverview of Pediatrics Notes (Dr. Bongalo)Angel BataNo ratings yet
- Newborn Screening TestDocument29 pagesNewborn Screening Testjinky_bsantos@yahoo.comNo ratings yet
- Beginning The Physical Examination: General Survey, Vital Signs, and PainDocument46 pagesBeginning The Physical Examination: General Survey, Vital Signs, and PainMoxie MacadoNo ratings yet
- Assessment Nursing Diagnosis Goals/ Expected Outcome S Nursing Intervention S Scientific Rationale Nursing Theory Core Values EvaluationDocument2 pagesAssessment Nursing Diagnosis Goals/ Expected Outcome S Nursing Intervention S Scientific Rationale Nursing Theory Core Values Evaluation8lueCzarcasmNo ratings yet
- Water Recreation and DiseaseDocument260 pagesWater Recreation and Diseasetuyetnam24No ratings yet
- Bukidnon State University College of Nursing Patient Monitoring SheetDocument6 pagesBukidnon State University College of Nursing Patient Monitoring SheetLucille Allen100% (7)
- Baus 2014Document5 pagesBaus 2014me13No ratings yet
- Anatomy of The BoneDocument12 pagesAnatomy of The BoneOpen Sea Ever CapturedNo ratings yet
- Research Secondary HypertensionDocument51 pagesResearch Secondary HypertensionDomeng TalksNo ratings yet
- Diagnosis Hfis DPP KlinikDocument8 pagesDiagnosis Hfis DPP KlinikFrans Aditiya TamaNo ratings yet
- Anestesia Embarazo y Mujer EmbarazadaDocument19 pagesAnestesia Embarazo y Mujer Embarazadanata0916No ratings yet
- UntitledDocument8 pagesUntitledapi-271638639No ratings yet
- Parmed X PDFDocument4 pagesParmed X PDFIoannis AmanatidisNo ratings yet
- A Screening Test For Obsessive-Compulsive DisorderDocument1 pageA Screening Test For Obsessive-Compulsive DisorderDebbie de GuzmanNo ratings yet
- CNH Construction Health DeclarationDocument1 pageCNH Construction Health DeclarationEna Ahmad PieNo ratings yet
- Cervical Spondylosis: Definition, Epidemiology, Clinical PresentationDocument14 pagesCervical Spondylosis: Definition, Epidemiology, Clinical PresentationJaspreet kaurNo ratings yet
- Prostate Cancer: Mr. Powers' CaseDocument13 pagesProstate Cancer: Mr. Powers' CaseTenth HokageNo ratings yet
- Giardia lamblia causes giardiasis in humansDocument13 pagesGiardia lamblia causes giardiasis in humansMirza Shaharyar BaigNo ratings yet
- JaundiceDocument30 pagesJaundiceNorakmal Andika YusriNo ratings yet
- Epigastric Lump: by Dr. S Tejaswi, Second Year PG Dept of General SurgeryDocument30 pagesEpigastric Lump: by Dr. S Tejaswi, Second Year PG Dept of General SurgerymahalakshmiNo ratings yet