You might also like
- Sialic Acids and Sialoglycoconjugates in the Biology of Life, Health and DiseaseFrom EverandSialic Acids and Sialoglycoconjugates in the Biology of Life, Health and DiseaseNo ratings yet
- Pneumonia: Past and Present: Dr. Pushpa Raj Sharma Professor of Child Health Institute of MedicineDocument41 pagesPneumonia: Past and Present: Dr. Pushpa Raj Sharma Professor of Child Health Institute of MedicineKartika RezkyNo ratings yet
- A Placebo-Controlled Trial of Silymarin in Patients With Nonalcoholic Fatty Liver DiseaseDocument6 pagesA Placebo-Controlled Trial of Silymarin in Patients With Nonalcoholic Fatty Liver Diseasesnn123456No ratings yet
- Royal College of Obstetricians and Gynaecologists: Peer Review DraftDocument11 pagesRoyal College of Obstetricians and Gynaecologists: Peer Review DraftaliNo ratings yet
- Phototherapyand Combinationtherapies ForvitiligoDocument22 pagesPhototherapyand Combinationtherapies ForvitiligoAro MandaNo ratings yet
- Liver EnzymesDocument6 pagesLiver EnzymesWande AyodeleNo ratings yet
- Oestrogen, Progesterone, AndrogensDocument58 pagesOestrogen, Progesterone, AndrogensTandin SonamNo ratings yet
- STD Treatment Guideline HCPDocument72 pagesSTD Treatment Guideline HCPKomang Adhi AmertajayaNo ratings yet
- Adrenocortical HyperfunctionDocument132 pagesAdrenocortical Hyperfunctionshobharamkrishna100% (2)
- Review: Epidemiology, Mechanisms, and Management of Diabetic GastroparesisDocument8 pagesReview: Epidemiology, Mechanisms, and Management of Diabetic GastroparesisIrma KurniawatiNo ratings yet
- TABLE 77-1: Differential Diagnosis and Management of Dermal MelanocytosisDocument29 pagesTABLE 77-1: Differential Diagnosis and Management of Dermal MelanocytosisHellenPertiwiWulandariNo ratings yet
- Graves' Disease & PregnancyDocument19 pagesGraves' Disease & Pregnancyrajan kumar100% (1)
- Graves' Hyperthyroidism Treatment OptionsDocument10 pagesGraves' Hyperthyroidism Treatment OptionsFideVegaNo ratings yet
- Citric Acid 10 Days CureDocument1 pageCitric Acid 10 Days Curelarry HNo ratings yet
- Bacteriotherapy Faqs PDFDocument17 pagesBacteriotherapy Faqs PDFpavaroti37No ratings yet
- Chronic Fatigue Syndrome: An Overview of Diagnosis and TreatmentDocument65 pagesChronic Fatigue Syndrome: An Overview of Diagnosis and TreatmentDavid_Waltos_2571No ratings yet
- Jeffrey Barratt, MDDocument27 pagesJeffrey Barratt, MDEmily EresumaNo ratings yet
- Vitamin B12 Deficiency and A Patient Case StudyDocument36 pagesVitamin B12 Deficiency and A Patient Case Studynherm6425100% (1)
- Anti-Diabetic Medication - Wikipedia, The Free EncyclopediaDocument12 pagesAnti-Diabetic Medication - Wikipedia, The Free Encyclopediaumesh123patilNo ratings yet
- CandidiasisDocument27 pagesCandidiasisBhavesh SippyNo ratings yet
- Urinary Tract Infection, Complicated (UTI) - Johns Hopkins ABX GuideDocument5 pagesUrinary Tract Infection, Complicated (UTI) - Johns Hopkins ABX GuideLaoMed plusNo ratings yet
- Clinical Review of Hereditary HaemochromatosisDocument6 pagesClinical Review of Hereditary HaemochromatosisVijeyachandhar DorairajNo ratings yet
- Bacterial Vaginosis Guide: Causes, Symptoms & TreatmentDocument7 pagesBacterial Vaginosis Guide: Causes, Symptoms & TreatmentgracegozaliNo ratings yet
- Adjuvant breast cancer therapy agentsDocument3 pagesAdjuvant breast cancer therapy agentsGem BulaongNo ratings yet
- Alcoholic Liver DiseaseDocument22 pagesAlcoholic Liver DiseaseVikramjeet SinghNo ratings yet
- CNW - Nov13-2007 - Health Canada Approves Health Claim For HMS 90 - ImmunocalDocument1 pageCNW - Nov13-2007 - Health Canada Approves Health Claim For HMS 90 - Immunocalapi-3714923No ratings yet
- 14.human GeneticsDocument18 pages14.human GeneticsRenjith Moorikkaran MNo ratings yet
- Cancer Prevention - The Causes and Prevention of Cancer Volume 1 (Cancer Prevention-Cancer Causes) (PDFDrive) PDFDocument338 pagesCancer Prevention - The Causes and Prevention of Cancer Volume 1 (Cancer Prevention-Cancer Causes) (PDFDrive) PDFtheresaNo ratings yet
- Evaluation and Treatment of Patients with Autism and Mitochondrial DiseaseDocument15 pagesEvaluation and Treatment of Patients with Autism and Mitochondrial DiseaseverdantlawNo ratings yet
- Ambiguous Genitalia 3Document4 pagesAmbiguous Genitalia 3syarifah salmaNo ratings yet
- Cushings Addisons and Acromegaly EdDocument45 pagesCushings Addisons and Acromegaly Edsamehseef100% (1)
- Fight Cancer with Nutritious Foods & DrinksDocument6 pagesFight Cancer with Nutritious Foods & DrinksTushar Varshney100% (1)
- Botulism 08.16.2013Document12 pagesBotulism 08.16.2013Emily EresumaNo ratings yet
- Pathogenesis of Hashimoto's Thyroiditis (Chronic Autoimmune Thyroiditis) - UpToDateDocument22 pagesPathogenesis of Hashimoto's Thyroiditis (Chronic Autoimmune Thyroiditis) - UpToDaterazvanNo ratings yet
- Varian Cysts: The Lebanese Society of Obstetrics and GynecologyDocument4 pagesVarian Cysts: The Lebanese Society of Obstetrics and GynecologyAde Gustina SiahaanNo ratings yet
- Neurobiologia Molecular Del Síndrome de Fatiga CrónicaDocument12 pagesNeurobiologia Molecular Del Síndrome de Fatiga CrónicaRicardo Jose De LeonNo ratings yet
- Mucosal Immunity I Imm2011Document38 pagesMucosal Immunity I Imm2011Lisa KangNo ratings yet
- GFCF Diet and Bio Medical Protocol for Autism RecoveryDocument7 pagesGFCF Diet and Bio Medical Protocol for Autism RecoveryScience NerdNo ratings yet
- Sleep Disorders in Children and Adolescents: Understanding Causes and Treatment OptionsDocument50 pagesSleep Disorders in Children and Adolescents: Understanding Causes and Treatment OptionsCitra Sukri Sugesti100% (1)
- Mixed Adrenergic Agonist DrugsDocument27 pagesMixed Adrenergic Agonist DrugsqbNo ratings yet
- Hepatobiliary Disease With AudioDocument46 pagesHepatobiliary Disease With Audioapi-195799092No ratings yet
- The Skin in commonly encountered systemic diseasesDocument42 pagesThe Skin in commonly encountered systemic diseasesrainmaker77771121No ratings yet
- Introduction and Overview of Community Health Nursing: Mary Ann Rosa MSN, RN, CS, GNPDocument66 pagesIntroduction and Overview of Community Health Nursing: Mary Ann Rosa MSN, RN, CS, GNPphoenix18075% (4)
- Morning Report: Laura Lascurain MD PGY 3 May 1, 2015Document19 pagesMorning Report: Laura Lascurain MD PGY 3 May 1, 2015Emily EresumaNo ratings yet
- Uveitis and IritisDocument5 pagesUveitis and IritisHester Marie SimpiaNo ratings yet
- Types of Insulin for Diabetes TreatmentDocument4 pagesTypes of Insulin for Diabetes TreatmentRaul Fernando Vasquez WoddensonNo ratings yet
- Cushing DiseaseDocument70 pagesCushing Diseaseاحمد المصرىNo ratings yet
- Telomere PDFDocument2 pagesTelomere PDFsoumita100% (1)
- The Psychological Impact of AusterityDocument16 pagesThe Psychological Impact of AusterityThe Centre for Welfare Reform100% (2)
- The Role of Zinc in Antiviral ImmunityDocument15 pagesThe Role of Zinc in Antiviral ImmunityKhalifatul Aulia AsyuriyahNo ratings yet
- More Than A Sore ThroatDocument17 pagesMore Than A Sore ThroatEmily EresumaNo ratings yet
- Pediatric Urology Topics Relating To Infants & Toddlers: Danielle Brady, Pgy-2Document35 pagesPediatric Urology Topics Relating To Infants & Toddlers: Danielle Brady, Pgy-2Emily EresumaNo ratings yet
- Classification of AnemiaDocument4 pagesClassification of AnemiaEna PaparićNo ratings yet
- Liver Flukes1Document50 pagesLiver Flukes1asmaa rashad100% (1)
- Thyroid Disease: Presentation By: Pimundu Vicent Audo Ritah Tutor: Dr. Fualal JaneDocument41 pagesThyroid Disease: Presentation By: Pimundu Vicent Audo Ritah Tutor: Dr. Fualal JaneEsther AumaNo ratings yet
- CrohnsDocument19 pagesCrohnsLauren LevyNo ratings yet
- Final Research Essay PcosDocument13 pagesFinal Research Essay Pcosapi-510714949No ratings yet
- Lysosomal Disorders - PedsDocument38 pagesLysosomal Disorders - PedsbencleeseNo ratings yet
- The Emerging Role of Serratiopeptidase in Oral Surgery: Literature UpdateDocument5 pagesThe Emerging Role of Serratiopeptidase in Oral Surgery: Literature UpdatejklhjNo ratings yet
- Vildagliptin + Metformin (Eucreas) PDFDocument19 pagesVildagliptin + Metformin (Eucreas) PDFddandan_2No ratings yet
- 11 Iron Deficiency AnaemiaDocument56 pages11 Iron Deficiency AnaemiaAbdul QuadirNo ratings yet
- Birth Injury Types and CausesDocument15 pagesBirth Injury Types and CausesBibäs AcharyaNo ratings yet
- Ari Whitten The Ultimate Guide To Red Light TherapyDocument41 pagesAri Whitten The Ultimate Guide To Red Light TherapyJulianne Bsc94% (35)
- Pharmacology Exams and NotesDocument17 pagesPharmacology Exams and NotesMrz AlzNo ratings yet
- ICD Dan Kategori Pengecualian DRAFTDocument132 pagesICD Dan Kategori Pengecualian DRAFTamita sindu kusuma100% (1)
- 152 409 1 PBDocument2 pages152 409 1 PBRendra Syani Ulya FitriNo ratings yet
- Identifying Chromosomes 12 and 14Document3 pagesIdentifying Chromosomes 12 and 14AstatinNo ratings yet
- Elderly HandbookDocument95 pagesElderly HandbookJojo ChuaNo ratings yet
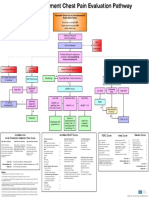
- Emergency Department Chest Pain Evaluation PathwayDocument2 pagesEmergency Department Chest Pain Evaluation Pathwaymuhammad sajidNo ratings yet
- Assignmen 1 AnswersDocument3 pagesAssignmen 1 AnswersAlasl BobyNo ratings yet
- MCNP Integrated Concepts NP 4Document11 pagesMCNP Integrated Concepts NP 4Karen Mae Santiago AlcantaraNo ratings yet
- Ibuprofen Drug StudyDocument3 pagesIbuprofen Drug StudySeann Loresco100% (2)
- Lesions of The Visual PathwayDocument2 pagesLesions of The Visual PathwayM StojanovskaNo ratings yet
- Output 1 Electrolytes - DraftDocument16 pagesOutput 1 Electrolytes - Draftallanrnmanaloto100% (1)
- Epinephrine DrugStudy WWW Rnpedia ComDocument4 pagesEpinephrine DrugStudy WWW Rnpedia ComIrish LigayaNo ratings yet
- Anthropometric Measurements and Nutritional AssessmentsDocument14 pagesAnthropometric Measurements and Nutritional AssessmentsSyeda Zainab AbbasNo ratings yet
- Poultry Diseases: Causes, Diagnosis and Treatment GuideDocument60 pagesPoultry Diseases: Causes, Diagnosis and Treatment GuideNarayan Yadav100% (1)
- Clinical MethodsDocument40 pagesClinical MethodsadniishariffNo ratings yet
- Bronchodilators Guide for Asthma and COPDDocument5 pagesBronchodilators Guide for Asthma and COPDdeepika kushwahNo ratings yet
- HSV Lesions and Recurrence RisksDocument24 pagesHSV Lesions and Recurrence RisksMichael Jansen SulaimanNo ratings yet
- CataractDocument38 pagesCataractruhulcoc1No ratings yet
- EEG For DummiesDocument10 pagesEEG For DummiesJosé GuevaraNo ratings yet
- Aiims Capsule AtfDocument252 pagesAiims Capsule Atfsimrankaur2003studNo ratings yet
- Pericardial Diseases: Acute PericarditisDocument26 pagesPericardial Diseases: Acute PericarditisamsirakNo ratings yet
- Sensory DisordersDocument5 pagesSensory DisordersMartin PersianNo ratings yet
- Kawasaki Disease: A Comprehensive Review: Kamleshun Ramphul, Stephanie Gonzalez MejiasDocument5 pagesKawasaki Disease: A Comprehensive Review: Kamleshun Ramphul, Stephanie Gonzalez MejiasAmarantoNo ratings yet
- Tla1 Midterm BSC100Document3 pagesTla1 Midterm BSC100AXCEL V. ANTOQUENo ratings yet
- University of Cebu-Banilad College of NursingDocument4 pagesUniversity of Cebu-Banilad College of NursingMauriceNo ratings yet