You might also like
- 23 Ifteni Tit Rápida 1 Acta - Psychiatrica - Scandinavica - 2014 - 130 - (1) - 25Document5 pages23 Ifteni Tit Rápida 1 Acta - Psychiatrica - Scandinavica - 2014 - 130 - (1) - 25observacionfray23No ratings yet
- Fludrocortisona - editorial.JACC .2016Document3 pagesFludrocortisona - editorial.JACC .2016jonasscopelNo ratings yet
- A Guideline and Checklist For Initiating and Managing Clozapine Treatment in Patients With Treatment-Resistant SchizophreniaDocument21 pagesA Guideline and Checklist For Initiating and Managing Clozapine Treatment in Patients With Treatment-Resistant SchizophreniaDian GbligNo ratings yet
- Journal Pone 0059672Document8 pagesJournal Pone 0059672mcgilicuttyNo ratings yet
- Geographic and Clinical Variation in Clozapine Use in The United StatesDocument7 pagesGeographic and Clinical Variation in Clozapine Use in The United StatesEvaG2012No ratings yet
- Lobos JA Et Al 2010Document191 pagesLobos JA Et Al 2010Evi LoNo ratings yet
- Effect OF Chlorpromazine AND Haloperidol Combination ON Lipid Profile IN Nigeria Schizophrenic PatientsDocument10 pagesEffect OF Chlorpromazine AND Haloperidol Combination ON Lipid Profile IN Nigeria Schizophrenic PatientstrianaamaliaNo ratings yet
- Norepinephrine Kinetics and Dynamics in Septic Shock and Trauma PatientsDocument7 pagesNorepinephrine Kinetics and Dynamics in Septic Shock and Trauma PatientsMoh SuriyawalNo ratings yet
- Clozapine and Haloperidol in ModeratelyDocument8 pagesClozapine and Haloperidol in Moderatelyrinaldiapt08No ratings yet
- Markovitz2002 Risp+Probenecid RCTDocument9 pagesMarkovitz2002 Risp+Probenecid RCTIulia CiocotisanNo ratings yet
- Management of Clozapine-Resistant Schizophrenia: Rob W. Kerwin & Anusha BolonnaDocument6 pagesManagement of Clozapine-Resistant Schizophrenia: Rob W. Kerwin & Anusha Bolonnaatika ichaNo ratings yet
- Clozapine Augementation in CRSDocument12 pagesClozapine Augementation in CRSMarius PaţaNo ratings yet
- Clotiapine - Another Forgotten Treassure in PsychiatryDocument1 pageClotiapine - Another Forgotten Treassure in PsychiatryJuan IgnacioNo ratings yet
- Oral Lichen PlanusDocument7 pagesOral Lichen Planusdrgurpal74100% (1)
- Clozapine: SchizophrenicDocument8 pagesClozapine: SchizophrenicVictoria FellowsNo ratings yet
- Suzuki 2011Document4 pagesSuzuki 2011Hesbon MomanyiNo ratings yet
- Use of Very-High-Dose Olanzapine in Treatment-Resistant SchizophreniaDocument4 pagesUse of Very-High-Dose Olanzapine in Treatment-Resistant SchizophreniaPutu Agus GrantikaNo ratings yet
- M34 16Document2 pagesM34 16Ana Tomas PetrovicNo ratings yet
- Cuma Abstraknya Aja: TTG Risperidone: Stroke Therapy TreatmentsDocument6 pagesCuma Abstraknya Aja: TTG Risperidone: Stroke Therapy TreatmentsChandz ChanDra ErryandariNo ratings yet
- Clozapine Use in A CohortDocument6 pagesClozapine Use in A CohortcaturNo ratings yet
- Clozapina 2Document12 pagesClozapina 2Robert MovileanuNo ratings yet
- Eria 2Document11 pagesEria 2ruth angelinaNo ratings yet
- A Novel, Highly Sensitive and Specific Biomarker For Niemann-Pick Type C1 DiseaseDocument8 pagesA Novel, Highly Sensitive and Specific Biomarker For Niemann-Pick Type C1 DiseaseTheodora TeddyNo ratings yet
- The Pharmacodynamics and Pharmacokinetics of Mivacurium in ChildrenDocument7 pagesThe Pharmacodynamics and Pharmacokinetics of Mivacurium in ChildrenluyawinNo ratings yet
- Kane1988 PDFDocument8 pagesKane1988 PDFRavi KumarNo ratings yet
- Screenshot 2023-10-04 at 21.11.14Document1 pageScreenshot 2023-10-04 at 21.11.14Joe DrumNo ratings yet
- Pharmacokinetics of Clozapine and Its Metabolites in Psychiatric Patients: Plasma Protein Binding and Renal ClearanceDocument7 pagesPharmacokinetics of Clozapine and Its Metabolites in Psychiatric Patients: Plasma Protein Binding and Renal ClearancegowaryNo ratings yet
- Levamisole Therapy in Children With Frequently Relapsing and Steroid-Dependent Nephrotic Syndrome - A Single-Center ExperienceDocument5 pagesLevamisole Therapy in Children With Frequently Relapsing and Steroid-Dependent Nephrotic Syndrome - A Single-Center ExperienceGading AuroraNo ratings yet
- HhhhhhfanDocument10 pagesHhhhhhfanVandhy P. Andi LoloNo ratings yet
- Oxberry, 2011Document7 pagesOxberry, 2011Maoi28No ratings yet
- Efficacy of Oral Lycopene in The Treatment of Oral LeukoplakiaDocument6 pagesEfficacy of Oral Lycopene in The Treatment of Oral Leukoplakia2211801733No ratings yet
- P Primary Open-Angle PatofisDocument2 pagesP Primary Open-Angle Patofisleonblizzara696No ratings yet
- Ten Common Mistakes in The Management of Lupus Nephritis. 2014Document10 pagesTen Common Mistakes in The Management of Lupus Nephritis. 2014Alejandro Rivera IbarraNo ratings yet
- Clozapine and Olanzapine Are Associated With Food.14Document5 pagesClozapine and Olanzapine Are Associated With Food.14jacopo pruccoliNo ratings yet
- Population Pharmacokinetics of Cyclosporine in Chinese Cardiac Transplant RecipientsDocument8 pagesPopulation Pharmacokinetics of Cyclosporine in Chinese Cardiac Transplant RecipientsGifari Muhammad SyabaNo ratings yet
- Diagnostic Journal 3Document9 pagesDiagnostic Journal 3dr.yogaNo ratings yet
- Cadeddu Et Al J Med Case Reports 2015Document6 pagesCadeddu Et Al J Med Case Reports 2015Sheila UlinaNo ratings yet
- Bauch-Atrial Natriuretic Peptide As A MarDocument6 pagesBauch-Atrial Natriuretic Peptide As A MarSzendeNo ratings yet
- Jurnal LisinoprilDocument7 pagesJurnal LisinoprildidiisafitriNo ratings yet
- Smelson Et Al 2002 Risperidone Decreases Craving and Relapses in Individuals With Schizophrenia and Cocaine DependenceDocument5 pagesSmelson Et Al 2002 Risperidone Decreases Craving and Relapses in Individuals With Schizophrenia and Cocaine Dependence20WH1A0557 KASHETTY DEEKSHITHANo ratings yet
- Vavuranakis 2022Document7 pagesVavuranakis 2022Amro MahmoudNo ratings yet
- Effectiveness of Treatment For Sudden Sensorineural Hearing LossDocument4 pagesEffectiveness of Treatment For Sudden Sensorineural Hearing Lossronaldyohanesf87No ratings yet
- The Effects of Intravenous Aminophylline On Level of Consciousness in Acute Intentional Benzodiazepines Poisoning in Comparison To FlumazenilDocument6 pagesThe Effects of Intravenous Aminophylline On Level of Consciousness in Acute Intentional Benzodiazepines Poisoning in Comparison To FlumazenilMarco Antonio Rosales GuerreroNo ratings yet
- Journal of Antimicrobial Chemotherapy Volume Issue 2016Document7 pagesJournal of Antimicrobial Chemotherapy Volume Issue 2016Ulima Mazaya GhaisaniNo ratings yet
- A Placebo-Controlled Trial of Oral Fingolimod in Relapsing Multiple SclerosisDocument15 pagesA Placebo-Controlled Trial of Oral Fingolimod in Relapsing Multiple SclerosisNidia BracamonteNo ratings yet
- Clinical Course of Steroid Sensitive Nephrotic Syndrome in Children: Outcome and OutlookDocument11 pagesClinical Course of Steroid Sensitive Nephrotic Syndrome in Children: Outcome and OutlookIkhbar FalahNo ratings yet
- LupusDocument8 pagesLupusFerdinand YuzonNo ratings yet
- Limited Reduction in Uremic Solute Concentrations With Increased Dialysis Frequency and Time in The Frequent Hemodialysis Network Daily TrialDocument7 pagesLimited Reduction in Uremic Solute Concentrations With Increased Dialysis Frequency and Time in The Frequent Hemodialysis Network Daily TrialyosefNo ratings yet
- Clozapine in Treatment of Schizophrenia: V. Burtea P. Ifteni A Teodorescu L. RogozeaDocument6 pagesClozapine in Treatment of Schizophrenia: V. Burtea P. Ifteni A Teodorescu L. RogozeaReza Badruun Syahrul HakimNo ratings yet
- Laprosy Research Paper (Ahmed Tanjimul Islam)Document7 pagesLaprosy Research Paper (Ahmed Tanjimul Islam)AHMED TANJIMUL ISLAMNo ratings yet
- Neurology 2016 Dhall S13 24Document13 pagesNeurology 2016 Dhall S13 24EstefaniSabrinaSandovalNo ratings yet
- Complementary and Alternative Medical Lab Testing Part 8: UrologyFrom EverandComplementary and Alternative Medical Lab Testing Part 8: UrologyRating: 3 out of 5 stars3/5 (1)
- Rhonda Byrne - El SecretoDocument8 pagesRhonda Byrne - El SecretoAlzeniraNo ratings yet
- ClozapineDocument5 pagesClozapineFebelina IdjieNo ratings yet
- Efficacy and Safety of Cyclosporine A For Patients With Steroid-Resistant Nephrotic Syndrome - A Meta-AnalysisDocument8 pagesEfficacy and Safety of Cyclosporine A For Patients With Steroid-Resistant Nephrotic Syndrome - A Meta-AnalysisIndah SolehaNo ratings yet
- Cerebrospinal Fluid Levels of Neopterin Are Elevated in Delirium After Hip FractureDocument9 pagesCerebrospinal Fluid Levels of Neopterin Are Elevated in Delirium After Hip Fractureyeremias setyawanNo ratings yet
- Biomedicines: Reduced Pro-Inflammatory Cytokines After Eight Weeks of Low-Dose Naltrexone For FibromyalgiaDocument9 pagesBiomedicines: Reduced Pro-Inflammatory Cytokines After Eight Weeks of Low-Dose Naltrexone For FibromyalgiaHima RamanNo ratings yet
- Neurology2018881847 PDFDocument9 pagesNeurology2018881847 PDFFelipe MNo ratings yet
- Lally 2015Document11 pagesLally 2015Mariana PestanaNo ratings yet
- Complementary and Alternative Medical Lab Testing Part 17: OncologyFrom EverandComplementary and Alternative Medical Lab Testing Part 17: OncologyNo ratings yet
- Changing: PsychiatryDocument30 pagesChanging: PsychiatrycaturNo ratings yet
- Diagnosis and Management For UrosepsisDocument8 pagesDiagnosis and Management For UrosepsisFitrianiMappasereNo ratings yet
- Pemeriksaaan Lab: Pemeriksaan 1 2 3Document1 pagePemeriksaaan Lab: Pemeriksaan 1 2 3caturNo ratings yet
- Guias Aspen 2016Document53 pagesGuias Aspen 2016Antonieta Latorre GardilcicNo ratings yet
- Jurnal LiteraturDocument6 pagesJurnal LiteraturpptpptNo ratings yet
- Ijms 20 01475 PDFDocument28 pagesIjms 20 01475 PDFFernanda GLNo ratings yet
- Jurnal ReddingDocument8 pagesJurnal Reddingirvan halimNo ratings yet
- 5 Clozapine-Resistant SchizophreniaDocument7 pages5 Clozapine-Resistant SchizophreniacaturNo ratings yet
- Olmos2019Document11 pagesOlmos2019caturNo ratings yet
- Diurnal Neurobiological Alterations After Exposure To Clozapine inDocument9 pagesDiurnal Neurobiological Alterations After Exposure To Clozapine incaturNo ratings yet
- Reduction of Pavlovian Bias in Schizophrenia: Enhanced Effects in Clozapine-Administered PatientsDocument23 pagesReduction of Pavlovian Bias in Schizophrenia: Enhanced Effects in Clozapine-Administered PatientscaturNo ratings yet
- The Tricyclic Antidepressant Clomipramine Inhibits Neuronal Autophagic FluxDocument9 pagesThe Tricyclic Antidepressant Clomipramine Inhibits Neuronal Autophagic FluxcaturNo ratings yet
- Clozapine Use in A CohortDocument6 pagesClozapine Use in A CohortcaturNo ratings yet
- Study On Antidepressant Drug To Cure Depression 2577 0543 1000121Document6 pagesStudy On Antidepressant Drug To Cure Depression 2577 0543 1000121caturNo ratings yet
- Ppok 1Document13 pagesPpok 1caturNo ratings yet
- The Tricyclic Antidepressant Clomipramine Inhibits Neuronal Autophagic FluxDocument9 pagesThe Tricyclic Antidepressant Clomipramine Inhibits Neuronal Autophagic FluxcaturNo ratings yet
- Depression Management Adult, Ambulatory Clinical Practice GuidelineDocument23 pagesDepression Management Adult, Ambulatory Clinical Practice GuidelinecaturNo ratings yet
- Ppok 1Document13 pagesPpok 1caturNo ratings yet
- Guia Apa TDMDocument152 pagesGuia Apa TDMpsicolauNo ratings yet
- GUIDLINE 15 - CPG - Diagnosis - DepressionDocument49 pagesGUIDLINE 15 - CPG - Diagnosis - DepressioncaturNo ratings yet
- CPG Asthma enDocument38 pagesCPG Asthma enSekar MutiaraNo ratings yet
- Study On Antidepressant Drug To Cure Depression 2577 0543 1000121Document6 pagesStudy On Antidepressant Drug To Cure Depression 2577 0543 1000121caturNo ratings yet
- GUIDLINE 15 - CPG - Diagnosis - DepressionDocument49 pagesGUIDLINE 15 - CPG - Diagnosis - DepressioncaturNo ratings yet
- Guia Apa TDMDocument152 pagesGuia Apa TDMpsicolauNo ratings yet
- Depression Management Adult, Ambulatory Clinical Practice GuidelineDocument23 pagesDepression Management Adult, Ambulatory Clinical Practice GuidelinecaturNo ratings yet
- CPG Asthma enDocument38 pagesCPG Asthma enSekar MutiaraNo ratings yet
- WfiDocument4 pagesWfiDevii RachmaaNo ratings yet
- Reology ItraconazolDocument10 pagesReology ItraconazolcaturNo ratings yet
- Bioequivalence of Two Pregabalin 300 MG Capsules (Neurexal and Lyrica) in Healthy Human VolunteersDocument5 pagesBioequivalence of Two Pregabalin 300 MG Capsules (Neurexal and Lyrica) in Healthy Human VolunteerscaturNo ratings yet
- Waiver FormDocument2 pagesWaiver Formapi-249429435No ratings yet
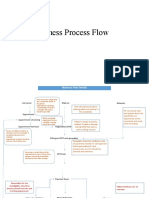
- Business Process FlowDocument12 pagesBusiness Process FlowKumar BalramNo ratings yet
- Prevalence of High Risk Pregnancy in Rural DharwadDocument4 pagesPrevalence of High Risk Pregnancy in Rural DharwadIOSRjournalNo ratings yet
- Chapter 2 Fire Fighter SafetyDocument2 pagesChapter 2 Fire Fighter SafetyMuhammad Alshikh100% (1)
- Three Biological Humors (The Tridoshas-Vata, Pitta and Kapha) and Their Role in Human SystemDocument45 pagesThree Biological Humors (The Tridoshas-Vata, Pitta and Kapha) and Their Role in Human SystemPrashanthNo ratings yet
- Uu No. 16 Tahun 1992Document120 pagesUu No. 16 Tahun 1992Nanda Yusuf Dwi PNo ratings yet
- Valid RRR Application 2013 - 2017 PDFDocument22,467 pagesValid RRR Application 2013 - 2017 PDFAyub NaveedNo ratings yet
- PERDEV DLL Unit 1 - M3 (Developmental Stages Handout)Document4 pagesPERDEV DLL Unit 1 - M3 (Developmental Stages Handout)Leonila MirandaNo ratings yet
- Periodontal Accelerated Osteogenic OrthodonticsDocument6 pagesPeriodontal Accelerated Osteogenic Orthodonticsyui cherryNo ratings yet
- 216 Miracle Acupunture Points: ShavoshangDocument12 pages216 Miracle Acupunture Points: Shavoshangடைகர் தேவாNo ratings yet
- Isu Dan Etika Pada Perawatan Paliatif PDFDocument17 pagesIsu Dan Etika Pada Perawatan Paliatif PDFNatasya ChieCaem FunforeverNo ratings yet
- Norma Ashrae 62 1989Document3 pagesNorma Ashrae 62 1989Mittzi CallejasNo ratings yet
- Hemodynamic MonitoringDocument35 pagesHemodynamic MonitoringWiz SamNo ratings yet
- ABPEA Preparatory Guidelines After ECQDocument2 pagesABPEA Preparatory Guidelines After ECQAndre ApostolNo ratings yet
- Why Is Research Important - NHS GroupDocument8 pagesWhy Is Research Important - NHS GroupRoxan PacsayNo ratings yet
- Lecture 10 - Repeat BreedingDocument2 pagesLecture 10 - Repeat Breedingkushal NeupaneNo ratings yet
- Individuals Trained To The Awareness Level Are Personnel Who Are Likely To Witness An Incident and Have Been Trained To Initiate Emergency Response byDocument21 pagesIndividuals Trained To The Awareness Level Are Personnel Who Are Likely To Witness An Incident and Have Been Trained To Initiate Emergency Response byacastillojose100% (1)
- A03 - Mr. Pradeep Kumar Tripathi - FPSC George Town 18/1A, A.N. Jha Marg Georgetown, Allahabad, UpDocument6 pagesA03 - Mr. Pradeep Kumar Tripathi - FPSC George Town 18/1A, A.N. Jha Marg Georgetown, Allahabad, UpSanjay GuptaNo ratings yet
- Nursing Process: Franco L. Razon, Man, RN Divine Word College of Legazpi College of NursingDocument72 pagesNursing Process: Franco L. Razon, Man, RN Divine Word College of Legazpi College of NursingFranco RazonNo ratings yet
- Wa0011Document12 pagesWa0011Frengky AndikaNo ratings yet
- What Concentration Is The Best To Kill GermsDocument3 pagesWhat Concentration Is The Best To Kill GermsAncaja, Jameir 1CNo ratings yet
- DIY Mineral MakeupDocument1 pageDIY Mineral MakeupDirek JP NinalgaNo ratings yet
- Muhanga District Development Plan 2013-2018-1 01Document116 pagesMuhanga District Development Plan 2013-2018-1 01Joseph Tuseku Officiel100% (1)
- Zinc in Wound Healing Theoretical, ExperimentalDocument15 pagesZinc in Wound Healing Theoretical, ExperimentalRifky Budi TriyatnoNo ratings yet
- Tienchi Ginseng Panax Notoginseng San Qircljo PDFDocument4 pagesTienchi Ginseng Panax Notoginseng San Qircljo PDFTobiasenHolgersen89No ratings yet
- Eritro Papulo Skuamosa 2021Document47 pagesEritro Papulo Skuamosa 2021Yolanda Agnesia Purba0% (1)
- Contingency PlanDocument1 pageContingency PlanPramod Bodne100% (3)
- 61Document11 pages61Mohammed Issa SalehNo ratings yet
- Approval Romania 2008Document27 pagesApproval Romania 2008Andrés Domínguez RuizNo ratings yet
- Effect of Human Papilloma Virus in HIV Infected Person: A Mini ReviewDocument7 pagesEffect of Human Papilloma Virus in HIV Infected Person: A Mini ReviewKIH 20162017No ratings yet