You might also like
- Compendium 2008 29 4 1-8Document8 pagesCompendium 2008 29 4 1-8brookortontiaNo ratings yet
- Corticotomy For Orthodontic Tooth MovementDocument8 pagesCorticotomy For Orthodontic Tooth MovementGissellePantojaNo ratings yet
- Orthodontically Driven Corticotomy: Tissue Engineering to Enhance Orthodontic and Multidisciplinary TreatmentFrom EverandOrthodontically Driven Corticotomy: Tissue Engineering to Enhance Orthodontic and Multidisciplinary TreatmentFederico BrugnamiNo ratings yet
- Wilko Don TicsDocument7 pagesWilko Don TicsMonika SonawaneNo ratings yet
- Wil CK Odon TicsDocument5 pagesWil CK Odon TicsRambabu SatipedakalaNo ratings yet
- Long-Term Effects of Vertical Bone Augmentation: A Systematic ReviewDocument15 pagesLong-Term Effects of Vertical Bone Augmentation: A Systematic ReviewShafira Nur Amalia ZulvaNo ratings yet
- Corticotomy-Assisted OrthodonticsDocument6 pagesCorticotomy-Assisted Orthodonticsyui cherryNo ratings yet
- Corticotomy Assisted Orthodontic TreatmentDocument6 pagesCorticotomy Assisted Orthodontic TreatmentAniket PotnisNo ratings yet
- Accelerated OrthodonticsDocument5 pagesAccelerated OrthodonticsMiguel Soni CasillasNo ratings yet
- Temporary Anchorage Devices in Orthodontics: A Paradigm ShiftDocument7 pagesTemporary Anchorage Devices in Orthodontics: A Paradigm ShiftsmritiNo ratings yet
- TE SIO Critical Commentary 7-8-12Document27 pagesTE SIO Critical Commentary 7-8-12misapopovNo ratings yet
- DR 3Document6 pagesDR 3ANGELA AMAYANo ratings yet
- Dental Research Journal: The Effect of Buccal Corticotomy On Accelerating Orthodontic Tooth Movement of Maxillary CanineDocument6 pagesDental Research Journal: The Effect of Buccal Corticotomy On Accelerating Orthodontic Tooth Movement of Maxillary CaninezaidNo ratings yet
- Surgical Assistance For Rapid Orthodontic Treatment and Temporary Skeletal Anchorage - 2014 - Oral and Maxillofacial Surgery Clinics of North AmericaDocument12 pagesSurgical Assistance For Rapid Orthodontic Treatment and Temporary Skeletal Anchorage - 2014 - Oral and Maxillofacial Surgery Clinics of North AmericaGabriela Lizbeth ArmentaNo ratings yet
- 2010 - Efficacy of Horizontal and Vertical Bone Augmentation ProceduresDocument24 pages2010 - Efficacy of Horizontal and Vertical Bone Augmentation ProceduresLenny GrauNo ratings yet
- ALVEOLAR DISTRACTION OSTEOGENESIS AND IMPLANTOLOGYDocument4 pagesALVEOLAR DISTRACTION OSTEOGENESIS AND IMPLANTOLOGYIJAR JOURNALNo ratings yet
- 3-3-40-485-3Document4 pages3-3-40-485-3Teresa Domingo JiménezNo ratings yet
- Biology of Tooth MovementDocument16 pagesBiology of Tooth MovementLanaNo ratings yet
- Biology of Orthodontic Tooth MovementDocument16 pagesBiology of Orthodontic Tooth MovementGowri ShankarNo ratings yet
- Distraction Osteogenesis of The Maxillofacial Skeleton: Clinical and Radiological EvaluationDocument27 pagesDistraction Osteogenesis of The Maxillofacial Skeleton: Clinical and Radiological EvaluationDevata RaviNo ratings yet
- 11 Durga Raju MachaDocument7 pages11 Durga Raju MachaKrupali JainNo ratings yet
- Basal Implants in The Mandibular Esthetic Zone A Case SeriesDocument6 pagesBasal Implants in The Mandibular Esthetic Zone A Case SeriesInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Retrospective Study: Lateral Ridge Augmentation Using Autogenous Dentin: Tooth-Shell Technique vs. Bone-Shell TechniqueDocument12 pagesRetrospective Study: Lateral Ridge Augmentation Using Autogenous Dentin: Tooth-Shell Technique vs. Bone-Shell TechniqueNarissaporn ChaiprakitNo ratings yet
- Biology of Tooth MovementDocument22 pagesBiology of Tooth MovementsakshiNo ratings yet
- Osteogenesis InglesDocument4 pagesOsteogenesis InglesJulio TorresNo ratings yet
- ImplantDocument46 pagesImplantMosica VladNo ratings yet
- Histologic Comparison of Biologic Width Around Teeth Versus Implants: The Effect On Bone PreservationDocument5 pagesHistologic Comparison of Biologic Width Around Teeth Versus Implants: The Effect On Bone PreservationPaul CerdaNo ratings yet
- Stem Cells in OrthodonticsDocument4 pagesStem Cells in OrthodonticsInternational Journal of Innovative Science and Research Technology100% (1)
- Ams 5 108Document4 pagesAms 5 108Alice EmailsNo ratings yet
- The Platform Switching Concept-A Myth or Fact: A Literature ReviewDocument5 pagesThe Platform Switching Concept-A Myth or Fact: A Literature ReviewChifa MusrataNo ratings yet
- Ι Mplant-Supported Overdentures: Clinical Review: · September 2017Document10 pagesΙ Mplant-Supported Overdentures: Clinical Review: · September 2017ankitaNo ratings yet
- The Osteoperiosteal Flap: A Simplified Approach to Alveolar Bone ReconstructionFrom EverandThe Osteoperiosteal Flap: A Simplified Approach to Alveolar Bone ReconstructionRating: 4 out of 5 stars4/5 (1)
- 6 Merheb 2014 Critical Buccal Bone DimensionsDocument9 pages6 Merheb 2014 Critical Buccal Bone DimensionsCarlos SilvaNo ratings yet
- Submerged Root TechniqueDocument5 pagesSubmerged Root TechniqueFrederick Alexander TrisnaNo ratings yet
- Chapterpdf Download635476105037 4Document20 pagesChapterpdf Download635476105037 4Abhishek JhaNo ratings yet
- Alveolar Ridge Preservation After Tooth Extraction Using Different Bone Graft Materials and Autologous Platelet ConcentratesDocument15 pagesAlveolar Ridge Preservation After Tooth Extraction Using Different Bone Graft Materials and Autologous Platelet ConcentratesnicolesigoloNo ratings yet
- Bone Grafts SatyaDocument153 pagesBone Grafts SatyaArchanaNo ratings yet
- Comparison of Alveolar Bone Loss Around Incisors in Normal Occlusion Samples and Surgical Skeletal Class III PatientsDocument8 pagesComparison of Alveolar Bone Loss Around Incisors in Normal Occlusion Samples and Surgical Skeletal Class III PatientsCindy Cendekiawati AnizarNo ratings yet
- Materiales P Vs RDocument11 pagesMateriales P Vs RJuliana RodriguezNo ratings yet
- Journal of The World Federation of OrthodontistsDocument7 pagesJournal of The World Federation of Orthodontistsvighanesh kadamNo ratings yet
- Speed Up Orthodontic Treatment With Corticotomy Facilitated TechniquesDocument27 pagesSpeed Up Orthodontic Treatment With Corticotomy Facilitated TechniquesSaravanan Kanagavel100% (1)
- Basic Knowledge of Bone Grafting: March 2012Document29 pagesBasic Knowledge of Bone Grafting: March 2012Nadira NurinNo ratings yet
- 3Document12 pages3kris.halim1997No ratings yet
- Review Cirugía Preprotésica. ArtículoDocument9 pagesReview Cirugía Preprotésica. ArtículoAnita Estela Batz MatulNo ratings yet
- Corticotomy AssisstedDocument12 pagesCorticotomy AssisstedRohini TondaNo ratings yet
- Alveolar Bone Resorption Under Complete DenturesDocument10 pagesAlveolar Bone Resorption Under Complete DenturesAbdelKhalek BouararaNo ratings yet
- Alloplastic Bone GraftsDocument62 pagesAlloplastic Bone GraftsMaysaa mahdiNo ratings yet
- Effect of Flapless Osteoperforation-Assisted Tooth Movement On Atrophic Alveolar Ridge: Histomorphometric and Gene-Enrichment AnalysisDocument9 pagesEffect of Flapless Osteoperforation-Assisted Tooth Movement On Atrophic Alveolar Ridge: Histomorphometric and Gene-Enrichment AnalysisThien LuNo ratings yet
- Changes in the Form and Structure of Residual Ridges OverviewDocument13 pagesChanges in the Form and Structure of Residual Ridges OverviewHeng SiekhongNo ratings yet
- Lingual Orthodontics ExplainedDocument36 pagesLingual Orthodontics ExplainedRajshekhar BanerjeeNo ratings yet
- 1 s2.0 S1883195817300889 Main PDFDocument10 pages1 s2.0 S1883195817300889 Main PDFridwan hardiNo ratings yet
- Distraction Osteogenesis SeminarDocument126 pagesDistraction Osteogenesis SeminarkeerthanNo ratings yet
- Aaid Joi D 17 00053Document11 pagesAaid Joi D 17 00053Yun De LinNo ratings yet
- Maxillary Sinus Bone GraftingDocument181 pagesMaxillary Sinus Bone GraftingTuấn Hành TrầnNo ratings yet
- Biologic Width - The No Encroachment Zone: I J D ADocument8 pagesBiologic Width - The No Encroachment Zone: I J D AJinny ShawNo ratings yet
- Bonegraftingforimplant Surgery: Ladi Doonquah,, Pierre-John Holmes,, Laxman Kumar Ranganathan,, Hughette RobertsonDocument19 pagesBonegraftingforimplant Surgery: Ladi Doonquah,, Pierre-John Holmes,, Laxman Kumar Ranganathan,, Hughette RobertsonJason LeeNo ratings yet
- Dental ArticulatorsDocument10 pagesDental ArticulatorsOmar Al-FatyanNo ratings yet
- Biology of The Alveolar Bone - Orthodontic Tissue Regeneration (OTR) PDFDocument5 pagesBiology of The Alveolar Bone - Orthodontic Tissue Regeneration (OTR) PDFDonald FlorezNo ratings yet
- 1 s2.0 S1607551X17307647 Main PDFDocument8 pages1 s2.0 S1607551X17307647 Main PDFindrayaniNo ratings yet
- Bone Grafts in Periodontal Surgery - A Review: July 2014Document4 pagesBone Grafts in Periodontal Surgery - A Review: July 2014Fajri AliNo ratings yet
- Corticotomy-Assisted OrthodonticsDocument6 pagesCorticotomy-Assisted Orthodonticsyui cherryNo ratings yet
- Periodontal Accelerated Osteogenic Orthodontics ADocument8 pagesPeriodontal Accelerated Osteogenic Orthodontics Ayui cherryNo ratings yet
- Suturing TechniquesDocument6 pagesSuturing TechniquesAldo TanNo ratings yet
- Diagnosis and Management of TemporomandibularDocument3 pagesDiagnosis and Management of Temporomandibularyui cherryNo ratings yet
- Suturing and Closure Techniques ExplainedDocument26 pagesSuturing and Closure Techniques Explainedyui cherryNo ratings yet
- Imf Single WireDocument7 pagesImf Single WireFirn Firth FirchNo ratings yet
- Mechanical and optical properties of glass-ionomer cementsDocument10 pagesMechanical and optical properties of glass-ionomer cementsyui cherryNo ratings yet
- Physical ExaminationDocument117 pagesPhysical Examinationsasmita nayakNo ratings yet
- TeethDocument17 pagesTeethSheryce Gwyneth GuadalupeNo ratings yet
- Ceballos, Mary Kate L. (BSN 1-Ya-18) - Week 7 - Laboratory Exercise - The Nervous System Cns and PnsDocument9 pagesCeballos, Mary Kate L. (BSN 1-Ya-18) - Week 7 - Laboratory Exercise - The Nervous System Cns and PnsKay ChoiNo ratings yet
- Radiology Report 2300985Document4 pagesRadiology Report 2300985JyotiNo ratings yet
- PDF Download Chapter 13 FullfrontalanatomycomDocument27 pagesPDF Download Chapter 13 FullfrontalanatomycomDr. Greg KingNo ratings yet
- Integumentary System Worksheet 1Document3 pagesIntegumentary System Worksheet 1Bea Lou SabadoNo ratings yet
- Ocular Complications With Dental Local Anaesthesia - A Systematic Review of Literature and Case ReportDocument4 pagesOcular Complications With Dental Local Anaesthesia - A Systematic Review of Literature and Case ReportNissaNo ratings yet
- IV. Choose the correct answer from between bracketsDocument15 pagesIV. Choose the correct answer from between bracketsMostafa ElsayedNo ratings yet
- Eyebrow Grooming Tips: How To Properly Tame Your BrowsDocument5 pagesEyebrow Grooming Tips: How To Properly Tame Your BrowsJeremiah ReardonNo ratings yet
- Understanding the Structure and Function of NeuronsDocument99 pagesUnderstanding the Structure and Function of Neurons[R2A] Khadijah AzlanNo ratings yet
- Geographic TongueDocument3 pagesGeographic TongueIrsalina SalmaNo ratings yet
- اسئلة تشريحDocument20 pagesاسئلة تشريحابراهيم فلاح حسنNo ratings yet
- Team Approach in Esthetic Dentistry.bDocument3 pagesTeam Approach in Esthetic Dentistry.bfloressam2000No ratings yet
- Arnett Combined Orthodontic and Surgical Open Bite CorrectionDocument12 pagesArnett Combined Orthodontic and Surgical Open Bite CorrectionAlex ReaNo ratings yet
- MCQ Final 2014Document19 pagesMCQ Final 2014JohnSon100% (1)
- Restorative Aspects of Periodontal Disease: An Update Part 2Document9 pagesRestorative Aspects of Periodontal Disease: An Update Part 2Dr Fahad and Associates Medical and dental clinicNo ratings yet
- Brainstem Medulla Pons MidbrainDocument3 pagesBrainstem Medulla Pons MidbrainAngela HabaradasNo ratings yet
- Neurology MCQ MixDocument53 pagesNeurology MCQ Mixezati pedramNo ratings yet
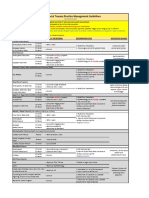
- VUMC Facial Trauma Practice Management GuidelinesDocument1 pageVUMC Facial Trauma Practice Management GuidelinesIndra D KristionoNo ratings yet
- EDT - Prosthodontics - Mid SummaryDocument17 pagesEDT - Prosthodontics - Mid SummaryneeNo ratings yet
- Anatomy of EarDocument3 pagesAnatomy of EarNitesh Kumar KarnaNo ratings yet
- AnatomyDocument11 pagesAnatomyKshitij Singh RajputNo ratings yet
- Endoscopic Anatomy of Nose and PNS FinalDocument98 pagesEndoscopic Anatomy of Nose and PNS FinalRahul Kurkure100% (2)
- LipflpbotoxDocument4 pagesLipflpbotoxAlexandra Luz StodieckNo ratings yet
- Organisation and Functions of The Nervous SystemDocument110 pagesOrganisation and Functions of The Nervous SystemBoemo BolaaneNo ratings yet
- Emotion, Personality, and The Frontal Lobe: Satoshi UmedaDocument15 pagesEmotion, Personality, and The Frontal Lobe: Satoshi UmedaCarmen Reyes RuizNo ratings yet
- Sensation and Perception Hand OutDocument4 pagesSensation and Perception Hand Outrosana f.rodriguezNo ratings yet
- Panoramic RadiographyDocument31 pagesPanoramic RadiographyMohammed abdalmenem100% (1)
- Dental 4Document13 pagesDental 4AHAMED SHIFAANNo ratings yet
- Skin Functions and LayersDocument30 pagesSkin Functions and LayersAswin Gumelar R.No ratings yet