You might also like
- LV36 Ignition SystemsDocument67 pagesLV36 Ignition SystemsĐức HòangNo ratings yet
- Fairview Terminal PhaseII Expansion Project Report - Oct2012Document436 pagesFairview Terminal PhaseII Expansion Project Report - Oct2012NewsroomNo ratings yet
- The Evolution of The Byzantine Liturgy - Juan MateosDocument29 pagesThe Evolution of The Byzantine Liturgy - Juan MateosȘtefan NuicăNo ratings yet
- Overview of The DSM 5Document68 pagesOverview of The DSM 5khalpopoNo ratings yet
- Anatomy and Physiology Chapter 1 Practice TestDocument13 pagesAnatomy and Physiology Chapter 1 Practice TestDani AnyikaNo ratings yet
- Flashover ReportDocument9 pagesFlashover ReportMahmoud A. SalemNo ratings yet
- Cloud Native Applications in A Telco WorldDocument22 pagesCloud Native Applications in A Telco WorldmarimcuriNo ratings yet
- DLL - Science 8 - Q2Document17 pagesDLL - Science 8 - Q2Nazer M. Lacabo100% (2)
- MCT385 PDFDocument21 pagesMCT385 PDFOleksandr YakubetsNo ratings yet
- Yle Movers PostersDocument2 pagesYle Movers PostersVictoria100% (2)
- Performance of Digital Morphology Analyzer Vision Pro On White Blood Cell DifferentialsDocument8 pagesPerformance of Digital Morphology Analyzer Vision Pro On White Blood Cell DifferentialsYojan Leo Irakurri PuenteNo ratings yet
- Clinical Biochemistry: E. Schapkaitz, S. RaburabuDocument7 pagesClinical Biochemistry: E. Schapkaitz, S. RaburabuMunawwar SaukaniNo ratings yet
- Semiquantitative, Fully Automated Urine Test Strip AnalysisDocument7 pagesSemiquantitative, Fully Automated Urine Test Strip AnalysisDewi PradnyaNo ratings yet
- Ok 2Document7 pagesOk 2cydolusNo ratings yet
- Size and Concentration Analyses of Extracellular Vesicles by NanoparticleDocument11 pagesSize and Concentration Analyses of Extracellular Vesicles by NanoparticleGuy EntractNo ratings yet
- Safely Reducing Manual Urine Microscopy Analyses by Combining Urine Flow Cytometer and Strip ResultsDocument7 pagesSafely Reducing Manual Urine Microscopy Analyses by Combining Urine Flow Cytometer and Strip ResultsFearless AngelNo ratings yet
- Diagnosis of Tuberculous Pleurisy With Combination.9Document7 pagesDiagnosis of Tuberculous Pleurisy With Combination.9sukiyantoNo ratings yet
- 10.1515 - Labmed 2023 0064Document9 pages10.1515 - Labmed 2023 0064Arturo Eduardo Huarcaya OntiverosNo ratings yet
- Bruegel 2015Document15 pagesBruegel 2015my accountNo ratings yet
- P77 Blood Screening For in Vitro Mechanical.205Document1 pageP77 Blood Screening For in Vitro Mechanical.205savasNo ratings yet
- Evaluation of The Performance of Sysmex XN-3100 Automated Hematology Analyzer Regarding The Sysmex XE-2100 and Microscopic ExaminationDocument9 pagesEvaluation of The Performance of Sysmex XN-3100 Automated Hematology Analyzer Regarding The Sysmex XE-2100 and Microscopic ExaminationbalkisNo ratings yet
- 02 Abstrak - Ebm Kedkel Kel 2Document2 pages02 Abstrak - Ebm Kedkel Kel 2Fathia ZahraNo ratings yet
- Ondas de Shoque SindromeDocument4 pagesOndas de Shoque SindromeJoha HerreñoNo ratings yet
- Managing Preanalytical HaematDocument8 pagesManaging Preanalytical HaematARIF AHAMMED PNo ratings yet
- Cellprep PaperDocument8 pagesCellprep PapermuratcavasNo ratings yet
- Quantitative LC Analysis of Cyclosporine A in OculDocument6 pagesQuantitative LC Analysis of Cyclosporine A in OculHammam HafidzurahmanNo ratings yet
- Butyrylcholinesterase in OsccDocument4 pagesButyrylcholinesterase in OsccKanad ChaudhuriNo ratings yet
- Reference Value Evaluation of Urine Sediment in Indonesian Adult Population Using Automated Urine AnalyzerDocument7 pagesReference Value Evaluation of Urine Sediment in Indonesian Adult Population Using Automated Urine AnalyzerptfajarindahlestariNo ratings yet
- New QuantitiesDocument6 pagesNew Quantities20100117 Bùi Thùy VyNo ratings yet
- Pi Is 0022346818306432Document6 pagesPi Is 0022346818306432Melian AnitaNo ratings yet
- WBC Count, CSF, XN 5000, 2014Document8 pagesWBC Count, CSF, XN 5000, 2014balkisNo ratings yet
- 1 s2.0 S2352551723000227 MainDocument8 pages1 s2.0 S2352551723000227 MainTudor VataNo ratings yet
- 14 Diagnostic Value of HematologyDocument24 pages14 Diagnostic Value of HematologyPablo LópezNo ratings yet
- Nakul Aquaronne2003Document11 pagesNakul Aquaronne2003shaimae abd el fattahNo ratings yet
- Jurnal 1.3Document7 pagesJurnal 1.3Zha Zha Nurul ZahraNo ratings yet
- SILVER IndexDocument6 pagesSILVER IndexvistamaniacNo ratings yet
- Ekin 2018Document3 pagesEkin 2018barbaramcoelho7No ratings yet
- GM 10029Document5 pagesGM 10029pramiswariNo ratings yet
- PKI - AN - 2017 - NexION 2000 ICPMS Trace Elements in Blood+SerumDocument6 pagesPKI - AN - 2017 - NexION 2000 ICPMS Trace Elements in Blood+SerumAdelitza StrubingerNo ratings yet
- XN 3000 VS BeckmanDocument8 pagesXN 3000 VS BeckmanZied FehriNo ratings yet
- 10 1111@ijlh 12760Document6 pages10 1111@ijlh 12760Hedo HidayatNo ratings yet
- Platelet Estimation by Manual and AutomationDocument4 pagesPlatelet Estimation by Manual and AutomationKamran DawoodNo ratings yet
- Clinical Chemistry and Laboratory Medicine (CCLM) Comparison of Five A..Document10 pagesClinical Chemistry and Laboratory Medicine (CCLM) Comparison of Five A..Rafat ElshemiNo ratings yet
- Tropmed 82 412Document3 pagesTropmed 82 412OlpinNo ratings yet
- Performance Evaluation of The Sysmex XP-300 in An Oncology Setting: Evaluation and Comparison of Hematological Parameters With The Sysmex XN-3000Document7 pagesPerformance Evaluation of The Sysmex XP-300 in An Oncology Setting: Evaluation and Comparison of Hematological Parameters With The Sysmex XN-3000Yojan Leo Irakurri PuenteNo ratings yet
- Radiological Predictors of Shunt Response in The Diagnosis and Treatment of Idiopathic Normal Pressure Hydrocephalus - A Systematic Review and Meta AnalysisDocument51 pagesRadiological Predictors of Shunt Response in The Diagnosis and Treatment of Idiopathic Normal Pressure Hydrocephalus - A Systematic Review and Meta AnalysisSantiago FuentesNo ratings yet
- Utility - of - Scatterplot - Patterns - of - Automated - Hematology Analysers 2020Document6 pagesUtility - of - Scatterplot - Patterns - of - Automated - Hematology Analysers 2020tufis02No ratings yet
- 09 Platelet Count by Peripheral Smear and Automated Cell Counter PDFDocument4 pages09 Platelet Count by Peripheral Smear and Automated Cell Counter PDFanggaririnNo ratings yet
- Letter To The Editor: Comparison Between Automated and Microscopic Analysis in Body Fluids CytologyDocument3 pagesLetter To The Editor: Comparison Between Automated and Microscopic Analysis in Body Fluids CytologybalkisNo ratings yet
- Chibuike GiftDocument14 pagesChibuike GiftalexdorcastitilayomiNo ratings yet
- Using Computerized Cephalometrics To Analyze The Vertical Dimension of OcclusionDocument10 pagesUsing Computerized Cephalometrics To Analyze The Vertical Dimension of OcclusionKaren DanaNo ratings yet
- Jurnal Alin Poct Dipstk UrineDocument9 pagesJurnal Alin Poct Dipstk Urineherlina armarianiNo ratings yet
- Spleen Stiffness-Spleen Size-To-platelet Ratio RiskDocument6 pagesSpleen Stiffness-Spleen Size-To-platelet Ratio RiskValentina IorgaNo ratings yet
- Educat I Onalqual I Fi Cat I Ons: M. Pharm - Quali TyassuranceDocument2 pagesEducat I Onalqual I Fi Cat I Ons: M. Pharm - Quali TyassuranceCatcoNo ratings yet
- Ok 3Document11 pagesOk 3cydolusNo ratings yet
- Complicaiones de La Ventriculostomia Agosto 2011Document6 pagesComplicaiones de La Ventriculostomia Agosto 2011Felipe Anduquia GarayNo ratings yet
- 2021 Article 1883Document8 pages2021 Article 1883Nurul ShafaNo ratings yet
- Mortality Rate and Other Clinical Features.63Document6 pagesMortality Rate and Other Clinical Features.63ariyantodr1985No ratings yet
- Comparison of Urine Analysis Using Manual and Sedimentation MethodsDocument5 pagesComparison of Urine Analysis Using Manual and Sedimentation Methodsobakhit91No ratings yet
- Endoscopic Ultrasound Versus Magnetic Resonance Cholangiopancreatography in Suspected Choledocholithiasis: A Systematic ReviewDocument11 pagesEndoscopic Ultrasound Versus Magnetic Resonance Cholangiopancreatography in Suspected Choledocholithiasis: A Systematic ReviewAysha AljabriNo ratings yet
- Cytology of Bone Fine Needle Aspiration BiopsyDocument11 pagesCytology of Bone Fine Needle Aspiration BiopsyRavi MehrotraNo ratings yet
- Counting of RBC & WBC IN URINE SAMPLEDocument6 pagesCounting of RBC & WBC IN URINE SAMPLEengNo ratings yet
- 10.1515 - CCLM 2021 1320Document5 pages10.1515 - CCLM 2021 1320geo4maryNo ratings yet
- Role of Hematological Scoring System in Diagnosis of Neonatal SepsisDocument7 pagesRole of Hematological Scoring System in Diagnosis of Neonatal SepsisIJAR JOURNALNo ratings yet
- Differentiating Ischemic From Hemorrhagic Stroke Using Plasma Biomarkers: The S100B/RAGE PathwayDocument8 pagesDifferentiating Ischemic From Hemorrhagic Stroke Using Plasma Biomarkers: The S100B/RAGE PathwayMade SudarjanaNo ratings yet
- Organic Sensors 1Document158 pagesOrganic Sensors 1るよNo ratings yet
- Impact of Endoscopy System, High Definition, and Virtual Chromo-Endoscopy in Daily Routine Colonoscopy: A Randomized TrialDocument7 pagesImpact of Endoscopy System, High Definition, and Virtual Chromo-Endoscopy in Daily Routine Colonoscopy: A Randomized Trialm_manuela2002No ratings yet
- RetrieveDocument11 pagesRetrieveMICHAEL NUGROHONo ratings yet
- 10 1016@j Joen 2018 08 006Document6 pages10 1016@j Joen 2018 08 006Jorge OrbeNo ratings yet
- Case Report:: Jana K, Chakraborty T, Ghosh T K, Ghosh S, Pathak SDocument3 pagesCase Report:: Jana K, Chakraborty T, Ghosh T K, Ghosh S, Pathak SivanNo ratings yet
- Bacteriological Evaluation of Bladder Calculi: A Study: Original Research ArticleDocument4 pagesBacteriological Evaluation of Bladder Calculi: A Study: Original Research ArticleivanNo ratings yet
- Bone Marrow Evaluation of Patients Having Pancytopenia at Tertiary Care Center, M. Y. Hospital, Indore, India: One-Year StudyDocument4 pagesBone Marrow Evaluation of Patients Having Pancytopenia at Tertiary Care Center, M. Y. Hospital, Indore, India: One-Year StudyivanNo ratings yet
- Correlation of Blood Glucose Levels, Hba1C, Hemoglobin and Leukocytes With Outcome On Acute StrokeDocument5 pagesCorrelation of Blood Glucose Levels, Hba1C, Hemoglobin and Leukocytes With Outcome On Acute StrokeivanNo ratings yet
- Secondary Hemophagocytic Lymphohistiocytosis: A Rare Case ReportDocument5 pagesSecondary Hemophagocytic Lymphohistiocytosis: A Rare Case ReportivanNo ratings yet
- Cobas® Taqman® HBV Test: Amplifying The PotentialDocument2 pagesCobas® Taqman® HBV Test: Amplifying The PotentialivanNo ratings yet
- 1242 5026 1 PBDocument5 pages1242 5026 1 PBivanNo ratings yet
- 4489 18254 1 PBDocument4 pages4489 18254 1 PBivanNo ratings yet
- Journal of Clinical Virology: Jihye Ha, Younhee Park, Hyon-Suk KimDocument4 pagesJournal of Clinical Virology: Jihye Ha, Younhee Park, Hyon-Suk KimivanNo ratings yet
- Prognostic Significance of Troponin T in Acute Myocardial InfarctionDocument6 pagesPrognostic Significance of Troponin T in Acute Myocardial InfarctionivanNo ratings yet
- With Robert Laurent and William ZorachDocument4 pagesWith Robert Laurent and William ZorachivanNo ratings yet
- (Laporan Kasus) : Scabies Management of Patient Children 5 Years OldDocument7 pages(Laporan Kasus) : Scabies Management of Patient Children 5 Years OldivanNo ratings yet
- Pengetahuan Hiv Dan Aids Pada Remaja Di Indonesia (Analisis Data Riskesdas 2010)Document10 pagesPengetahuan Hiv Dan Aids Pada Remaja Di Indonesia (Analisis Data Riskesdas 2010)ivanNo ratings yet
- 1 s2.0 S2590098621000130 MainDocument8 pages1 s2.0 S2590098621000130 MainEgo-free New-earthNo ratings yet
- Agriculture4 0-IEEETIIDocument13 pagesAgriculture4 0-IEEETIIAmanda FNo ratings yet
- Literature Review Benefits Outdoor PlayDocument7 pagesLiterature Review Benefits Outdoor Playfvg6kcwy100% (1)
- Java-Frequently Asked Interview QuestionsDocument2 pagesJava-Frequently Asked Interview QuestionsS.S. AmmarNo ratings yet
- Raghunathan 2015Document5 pagesRaghunathan 2015STOCK IKRAM GROUPNo ratings yet
- Aqa 83622 SMS PDFDocument14 pagesAqa 83622 SMS PDFT SolomonNo ratings yet
- Motives and Functions of A Business Chapter 1Document31 pagesMotives and Functions of A Business Chapter 1Zeeshan AfzalNo ratings yet
- List of Top Paid Keywords On Google AdsenseDocument4 pagesList of Top Paid Keywords On Google AdsenseRobert DurăNo ratings yet
- Twining 1Document16 pagesTwining 1juansespinosaNo ratings yet
- U-Bolts For PolesDocument11 pagesU-Bolts For PolesMosa Elnaid ElnaidNo ratings yet
- Arts 6 Module 1Document18 pagesArts 6 Module 1Elexthéo JoseNo ratings yet
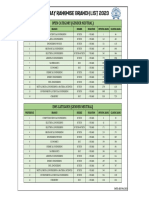
- Iit Bombay Rankwise Branch List 2023Document1 pageIit Bombay Rankwise Branch List 2023Ratan ChoudharyNo ratings yet
- TMF814 Network SimulatorDocument496 pagesTMF814 Network SimulatorNguyen Anh DucNo ratings yet
- 10 Multicast Zone Routing Protocol For Mobile Ad Hoc NetworksDocument6 pages10 Multicast Zone Routing Protocol For Mobile Ad Hoc NetworksakshusvgNo ratings yet
- Prla 2 Set 1 Story - Friends For LifeDocument4 pagesPrla 2 Set 1 Story - Friends For Lifehilmann.ariffinnNo ratings yet
- Ec Declaration of Conformity: QAS60 PDS 400 V 50 HZDocument6 pagesEc Declaration of Conformity: QAS60 PDS 400 V 50 HZFernando Morales PachonNo ratings yet
- Tcs Eis Case Study BPCLDocument4 pagesTcs Eis Case Study BPCLsumitkr_20181No ratings yet
- EpicsDocument5 pagesEpicsLynette JavaNo ratings yet
- Oxnard: Tsunami Evacuation MapsDocument2 pagesOxnard: Tsunami Evacuation MapsVentura County Star100% (1)
- LP Expert Detective Class 6Document5 pagesLP Expert Detective Class 6Abhishek SumanNo ratings yet