You might also like
- Congenital Heart DiseaseDocument38 pagesCongenital Heart DiseaseSnIP StandredNo ratings yet
- Congenital Heart DiseasesDocument6 pagesCongenital Heart Diseasestheglobalnursing100% (2)
- Pediatric Nursing Reviewer CardiovascularDocument4 pagesPediatric Nursing Reviewer CardiovascularJemy Lorane TemporalNo ratings yet
- Peds Exam 3Document25 pagesPeds Exam 3Yu Yu ChenNo ratings yet
- Cardio Vascular DisordersDocument62 pagesCardio Vascular DisordersUday Kumar100% (1)
- Tiki Taka Notes Final PDFDocument104 pagesTiki Taka Notes Final PDFAditiSahak62No ratings yet
- Cardiovascular System: by DR - Nuha Abdel GhaffarDocument41 pagesCardiovascular System: by DR - Nuha Abdel GhaffarMohammed Alaa EldeanNo ratings yet
- Valvular Heart Disease Nursing Care and DiagnosisDocument41 pagesValvular Heart Disease Nursing Care and DiagnosisVirendra Shekhawat100% (1)
- Congenital Heart Disease GuideDocument77 pagesCongenital Heart Disease GuideMalueth Angui100% (1)
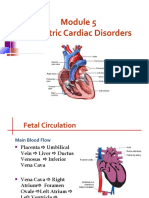
- Pediatric Cardiac Disorders: Fetal Circulation and Congestive Heart FailureDocument62 pagesPediatric Cardiac Disorders: Fetal Circulation and Congestive Heart FailureMarie Queenly Pagaran100% (1)
- Wk7 PLP Cardiovascular Disorder Part 1,2,3,4Document210 pagesWk7 PLP Cardiovascular Disorder Part 1,2,3,4claire yowsNo ratings yet
- MITRAL STENOSIS AND AORTIC STENOSIS CAUSES, SYMPTOMS AND TREATMENTDocument6 pagesMITRAL STENOSIS AND AORTIC STENOSIS CAUSES, SYMPTOMS AND TREATMENTKobby AmoahNo ratings yet
- Congenital Heart Disease - Cynotic AcynoticDocument34 pagesCongenital Heart Disease - Cynotic Acynoticvruttika parmarNo ratings yet
- Angelina A Joho MSC in Critical Care and TraumaDocument50 pagesAngelina A Joho MSC in Critical Care and TraumaZabron LuhendeNo ratings yet
- Congenital Heart Diseases: TopicsDocument19 pagesCongenital Heart Diseases: TopicsMaheen SyedNo ratings yet
- Cardiovascular Disorders: Prepared By: Wad-Ey, Rosie Glae, RNDocument49 pagesCardiovascular Disorders: Prepared By: Wad-Ey, Rosie Glae, RNrosieglaeNo ratings yet
- PericarditisDocument52 pagesPericarditissanjivdasNo ratings yet
- Heart FailureDocument39 pagesHeart FailureMuhammad AsifNo ratings yet
- PedsnotesDocument18 pagesPedsnoteskp13oyNo ratings yet
- Lesson No 3 Cardiac TamponadeDocument6 pagesLesson No 3 Cardiac TamponadeMary Grace GestiadaNo ratings yet
- 515Document972 pages515solecitodelmarazul100% (6)
- Cardiovascular DisorderDocument21 pagesCardiovascular Disorderdanica cordovaNo ratings yet
- Congenital Heart Disease: PathophysiologyDocument21 pagesCongenital Heart Disease: PathophysiologyChin Chan100% (1)
- Total Anomalous Venous ReturnDocument4 pagesTotal Anomalous Venous ReturnJohn Bernard Ting TizonNo ratings yet
- Cor PulmonaleDocument33 pagesCor PulmonaleSanda AnaNo ratings yet
- Quiz Blessings #5Document3 pagesQuiz Blessings #5Rachel LiuNo ratings yet
- Module No. Date: Topic:: Cues/Questions/ Keywords Notes Congenital Heart DisordersDocument28 pagesModule No. Date: Topic:: Cues/Questions/ Keywords Notes Congenital Heart Disordersanon ymousNo ratings yet
- Congestive Heart Failure and Asthma Case StudiesDocument21 pagesCongestive Heart Failure and Asthma Case Studiesangelica dizonNo ratings yet
- PAEDs - CVS-1Document44 pagesPAEDs - CVS-1Priscah bhokeNo ratings yet
- Congenital Heart DeseasesDocument54 pagesCongenital Heart DeseasesAntony100% (1)
- Tof and PdaDocument47 pagesTof and PdaskerstinNo ratings yet
- Quiz 2 Sa PediaDocument6 pagesQuiz 2 Sa Pediaqweyo yhuNo ratings yet
- Pediatric Cardiac DisordersDocument55 pagesPediatric Cardiac DisordersgraciaNo ratings yet
- (I..) KMU Peads CardicDocument88 pages(I..) KMU Peads CardicMuhammadNo ratings yet
- Pulmonary Thromboembolism: DR Olubunmi Ogunlade Consultant PulmonologistDocument34 pagesPulmonary Thromboembolism: DR Olubunmi Ogunlade Consultant PulmonologistEmeka Chinedu Precious PetrousNo ratings yet
- Tetralogy of Fallot Cyanotic Lesion GuideDocument12 pagesTetralogy of Fallot Cyanotic Lesion Guideputri nadNo ratings yet
- Heart Failure in ChildrenDocument44 pagesHeart Failure in ChildrenRisna Ariani100% (2)
- Approach To Cyanotic Heart Disease Christopher Cheung Santokh Dhillon PDFDocument13 pagesApproach To Cyanotic Heart Disease Christopher Cheung Santokh Dhillon PDFsuckeydluffyNo ratings yet
- Aortic StenosisDocument3 pagesAortic StenosisKhalid Mahmud Arifin100% (1)
- Congenital Heart DiseaseDocument43 pagesCongenital Heart DiseaseSanjanaNo ratings yet
- LME SelfDocument5 pagesLME SelfJM Mizraime Gallo Dela-peñaNo ratings yet
- Cardiac TamponadeDocument10 pagesCardiac Tamponadetitusrop10No ratings yet
- Medicine in Brief: Name the Disease in Haiku, Tanka and ArtFrom EverandMedicine in Brief: Name the Disease in Haiku, Tanka and ArtRating: 5 out of 5 stars5/5 (1)
- CHD Final 1Document9 pagesCHD Final 1danica grace gubaNo ratings yet
- Conginital Heart DiseaseDocument19 pagesConginital Heart DiseaseSanthosh.S.UNo ratings yet
- CHFSP 2005Document36 pagesCHFSP 2005Andy F MonroeNo ratings yet
- ucu-CHDs_240114_230618 (2)Document68 pagesucu-CHDs_240114_230618 (2)BrianNo ratings yet
- PDA and COA Nursing CareDocument18 pagesPDA and COA Nursing CareDenise EspinosaNo ratings yet
- Types & Treatments of Acyanotic Heart Disease ObstructionsDocument4 pagesTypes & Treatments of Acyanotic Heart Disease ObstructionsJessica Carmela CasugaNo ratings yet
- Cardiac Tamponade and ManagementDocument42 pagesCardiac Tamponade and Managementأم حمدNo ratings yet
- Pathophysiology Congenital Heart Disease-1Document54 pagesPathophysiology Congenital Heart Disease-1single_ladyNo ratings yet
- Case Study PPT Patho NLNGDocument36 pagesCase Study PPT Patho NLNGKate ChavezNo ratings yet
- Fetal Perfusion/Congenital Heart DefectsDocument13 pagesFetal Perfusion/Congenital Heart DefectsMatthew RyanNo ratings yet
- Congenital Heart DefectDocument12 pagesCongenital Heart Defectsangkularosmina837No ratings yet
- Cardiovascular System Dr. Eman Badr 2020Document182 pagesCardiovascular System Dr. Eman Badr 2020Amina DinarNo ratings yet
- Congenital Heart DiseasesDocument21 pagesCongenital Heart DiseasesfahmiNo ratings yet
- Cardiac Tamponade (P)Document16 pagesCardiac Tamponade (P)CloudySkyNo ratings yet
- Congenital Heart Diseases: DR - Ankita Patel MPT (Cardio-Pulmonary)Document41 pagesCongenital Heart Diseases: DR - Ankita Patel MPT (Cardio-Pulmonary)heena solankiNo ratings yet
- Aortic RegurgitationDocument3 pagesAortic RegurgitationKhalid Mahmud Arifin100% (1)
- 3 World Literature HOMERDocument2 pages3 World Literature HOMERAngel Joy CatalanNo ratings yet
- Clinical Evaluation of Baccalaureate Nursing Students Using SBAR Format: Faculty Versus Self EvaluationDocument5 pagesClinical Evaluation of Baccalaureate Nursing Students Using SBAR Format: Faculty Versus Self EvaluationAngel Joy CatalanNo ratings yet
- Chronic Obstructive Pulmonary Disease (COPD) and Bronchial AsthmaDocument16 pagesChronic Obstructive Pulmonary Disease (COPD) and Bronchial AsthmaAngel Joy CatalanNo ratings yet
- 1 Overview of Literature and Its CharacteristicsDocument20 pages1 Overview of Literature and Its CharacteristicsAngel Joy CatalanNo ratings yet
- Introduction To World Literature: by Katrina Melissa CruzDocument3 pagesIntroduction To World Literature: by Katrina Melissa CruzElmar Dela TorreNo ratings yet
- 4 6 Risk Factors For CHDDocument12 pages4 6 Risk Factors For CHDHazel LopezNo ratings yet
- Chap 3 Paper - Theoretical Frameworks and Nursing ResearchDocument9 pagesChap 3 Paper - Theoretical Frameworks and Nursing ResearchEtty EriyantiNo ratings yet
- Integumentary Changes of The Aging AdultDocument7 pagesIntegumentary Changes of The Aging AdultAngel Joy CatalanNo ratings yet
- Theories of DevelopmentDocument17 pagesTheories of DevelopmentAngel Joy CatalanNo ratings yet
- Common Respiratory InterventionsDocument10 pagesCommon Respiratory InterventionsAngel Joy CatalanNo ratings yet
- Impact of Aging Family Members on CaregiversDocument5 pagesImpact of Aging Family Members on CaregiversAngel Joy CatalanNo ratings yet
- Cardiovascular DisordersDocument10 pagesCardiovascular DisordersAngel Joy CatalanNo ratings yet
- Nursing ManagementDocument6 pagesNursing ManagementkenNo ratings yet
- Impact of The Ageing Member To The FamilyDocument5 pagesImpact of The Ageing Member To The FamilyAngel Joy CatalanNo ratings yet
- IntroductionDocument2 pagesIntroductionAngel Joy CatalanNo ratings yet
- Diagnostic Studies and TherapiesDocument11 pagesDiagnostic Studies and TherapiesAngel Joy CatalanNo ratings yet
- 38139172Document58 pages38139172Paulo CesarNo ratings yet
- Theories of DevelopmentDocument17 pagesTheories of DevelopmentAngel Joy CatalanNo ratings yet
- Impact of The Ageing Member To The FamilyDocument5 pagesImpact of The Ageing Member To The FamilyAngel Joy CatalanNo ratings yet
- Module 1 Concepts in Caring for Older AdultsDocument33 pagesModule 1 Concepts in Caring for Older AdultsAngel Joy Catalan100% (1)
- Respiratory Disorders IIDocument24 pagesRespiratory Disorders IIAngel Joy CatalanNo ratings yet
- Diagnostic Studies and TherapiesDocument11 pagesDiagnostic Studies and TherapiesAngel Joy CatalanNo ratings yet
- Common Respiratory InterventionsDocument10 pagesCommon Respiratory InterventionsAngel Joy CatalanNo ratings yet
- Attachment PDFDocument5 pagesAttachment PDFsiska marlianaNo ratings yet
- Respiratory DisordersDocument10 pagesRespiratory DisordersAngel Joy CatalanNo ratings yet
- Perspectives of AgingDocument34 pagesPerspectives of AgingAngel Joy CatalanNo ratings yet
- Overview of Anatomy and Physiology of The Respiratory SystemDocument6 pagesOverview of Anatomy and Physiology of The Respiratory SystemAngel Joy CatalanNo ratings yet
- Community Health Nursing Concepts and PrinciplesDocument7 pagesCommunity Health Nursing Concepts and PrinciplesAngel Joy CatalanNo ratings yet
- COMMUNITY HEALTH NURSING (Continuation)Document18 pagesCOMMUNITY HEALTH NURSING (Continuation)Angel Joy Catalan100% (2)
- Cardiovascular Disorders: Types of DysrythmiasDocument3 pagesCardiovascular Disorders: Types of Dysrythmiasjamie carpioNo ratings yet
- 2.500548 Medilog Holter System PP en LQDocument8 pages2.500548 Medilog Holter System PP en LQIvan CvasniucNo ratings yet
- ECG EKG Examples and QuizDocument26 pagesECG EKG Examples and QuizBUBBUNo ratings yet
- Antianginal DrugsDocument47 pagesAntianginal Drugsmospala285No ratings yet
- Round 1 Round 2 Round 3: Rank Course Rank Course CourseDocument500 pagesRound 1 Round 2 Round 3: Rank Course Rank Course CourseSrinivas PingaliNo ratings yet
- King Abdulaziz University College of Pharmacy Clinical PharmacyDocument3 pagesKing Abdulaziz University College of Pharmacy Clinical PharmacyHusnain AhmadNo ratings yet
- 2013 ESC Stabilna Koronarna BolestDocument66 pages2013 ESC Stabilna Koronarna BolestМилан ЛабудовићNo ratings yet
- Pulmonary Hypertension (PDFDrive)Document264 pagesPulmonary Hypertension (PDFDrive)Anonymous oQtve4o100% (1)
- Emergency Cardiovascular CareDocument56 pagesEmergency Cardiovascular CareAdit PradaNaNo ratings yet
- VT CriteriaDocument8 pagesVT CriterianitipatNo ratings yet
- Cardiology MCQsDocument5 pagesCardiology MCQsTessa Neilson75% (4)
- National ECG Workshop AIMST MMA 2015Document217 pagesNational ECG Workshop AIMST MMA 2015Sara100% (1)
- List of Empanelled (South)Document14 pagesList of Empanelled (South)Ilam BaruthiNo ratings yet
- Rapid HFDocument9 pagesRapid HFDoc Tor StrangeNo ratings yet
- Share how the S8 Defibrillator Monitor provides a full range of life support functionsDocument4 pagesShare how the S8 Defibrillator Monitor provides a full range of life support functionsJuan Esteban F.No ratings yet
- Dharavi Slum InterventionDocument6 pagesDharavi Slum InterventionEdward DenbroughNo ratings yet
- Isosorbide DinitrateDocument1 pageIsosorbide Dinitrate202110439No ratings yet
- Basic Ecg InterpratationDocument71 pagesBasic Ecg Interpratationgunawan susantoNo ratings yet
- Basic Life Support (BLS) in AdultsDocument13 pagesBasic Life Support (BLS) in AdultsElena ChitoiuNo ratings yet
- Heart Defect PDFDocument6 pagesHeart Defect PDFRosemaryCastroNo ratings yet
- 3aatrialrhythms 110624075109 Phpapp02Document35 pages3aatrialrhythms 110624075109 Phpapp02Win Ichda AlfahleviNo ratings yet
- Risk of Arrhythmia and Sudden Death - M. Malik (BMJ, 2001) WWDocument429 pagesRisk of Arrhythmia and Sudden Death - M. Malik (BMJ, 2001) WWRohan Upadhyay UpadhyayNo ratings yet
- Rivaroxavan en Fa ValvularDocument5 pagesRivaroxavan en Fa Valvularcarlos pardoNo ratings yet
- Ccu Cad NCPDocument5 pagesCcu Cad NCPheyyymeeeNo ratings yet
- Cardiac EmergenciesDocument26 pagesCardiac Emergenciespreet kaurNo ratings yet
- David Montgomery MD PHD BioDocument2 pagesDavid Montgomery MD PHD Biolilsowell89No ratings yet
- MBBS Antiarrhythmics 2014 Class II (Antiarrhythmic Drugs)Document23 pagesMBBS Antiarrhythmics 2014 Class II (Antiarrhythmic Drugs)Dr.U.P.Rathnakar.MD.DIH.PGDHM100% (1)
- Newsletter 72010Document8 pagesNewsletter 72010Slusom WebNo ratings yet
- Unstable Angina PectorisDocument24 pagesUnstable Angina PectorisAkbar IskandarNo ratings yet
- Heart and PericardiumDocument26 pagesHeart and PericardiumpalNo ratings yet