You might also like
- Financial Planning GodrejDocument199 pagesFinancial Planning GodrejriteshnaikNo ratings yet
- Retinal DetachmentDocument21 pagesRetinal Detachmentณัช เกษมNo ratings yet
- Senile Cataract (Age-Related Cataract) : Practice Essentials, Background, PathophysiologyDocument6 pagesSenile Cataract (Age-Related Cataract) : Practice Essentials, Background, PathophysiologyadliahghaisaniNo ratings yet
- Arsenic and Old LaceDocument180 pagesArsenic and Old LaceGlenn Calvin50% (2)
- Glaucoma and CataractDocument30 pagesGlaucoma and CataractJayselle ArvieNo ratings yet
- Childhood Cataracts and Other JadiDocument49 pagesChildhood Cataracts and Other JadiSania NadianisaNo ratings yet
- Cataract PTDocument9 pagesCataract PTPreeti SharmaNo ratings yet
- Congenital Cataract GuideDocument18 pagesCongenital Cataract GuideMohamad Hafyfy75% (4)
- Acid Base ImbalanceDocument50 pagesAcid Base ImbalanceDian Pratiwi BurnamaNo ratings yet
- 3rd Periodical Exam Math 9Document1 page3rd Periodical Exam Math 9DhangManongas-LlaboreVete100% (2)
- Construction Engineering and ManagementDocument3 pagesConstruction Engineering and ManagementMica XDNo ratings yet
- Proulx Et Al (Eds.) - The Wiley Handbook of What Works With Sexual Offenders. Contemporary Perspectives in Theory, Assessment, Treatment, (2020)Document530 pagesProulx Et Al (Eds.) - The Wiley Handbook of What Works With Sexual Offenders. Contemporary Perspectives in Theory, Assessment, Treatment, (2020)willl100% (1)
- Cataract PTDocument9 pagesCataract PTpreeti sharmaNo ratings yet
- Retinal DetachmentDocument8 pagesRetinal DetachmentJohanLazuardiNo ratings yet
- Blues A La Machito - CongasDocument2 pagesBlues A La Machito - CongasDavid ScaliseNo ratings yet
- The Handbook of English For Specific Purposes: Edited by Brian Paltridge and Sue StarfieldDocument50 pagesThe Handbook of English For Specific Purposes: Edited by Brian Paltridge and Sue StarfieldEmiliano AcevedoNo ratings yet
- Research Proposal Visual ProblemDocument20 pagesResearch Proposal Visual Problemyaqoob008100% (2)
- Retinal DetachmentDocument10 pagesRetinal DetachmentSilpi HamidiyahNo ratings yet
- Araling Panlipunan 4Document150 pagesAraling Panlipunan 4Alyce Ajtha100% (2)
- Vitreous Floater1Document7 pagesVitreous Floater1mithaa octoviagnesNo ratings yet
- Cataract - Ophthalmology - FastbleepDocument9 pagesCataract - Ophthalmology - FastbleepFaiq Syukri Bin SaparudinNo ratings yet
- Cataract Surgery: A Brief History and OverviewDocument15 pagesCataract Surgery: A Brief History and OverviewwhiezardNo ratings yet
- CATARACTDocument25 pagesCATARACTDea NabilaNo ratings yet
- Biology Invesigatory Project: Group MembersDocument13 pagesBiology Invesigatory Project: Group MembersNavaneeth KrishnanNo ratings yet
- Cataract. Slit Lamp Photograph Cataract. Slit Lamp Photograph FollowingDocument6 pagesCataract. Slit Lamp Photograph Cataract. Slit Lamp Photograph Followingekin_shashaNo ratings yet
- Senile Cataract Clinical Presentation and CausesDocument4 pagesSenile Cataract Clinical Presentation and CausesAhmad FahroziNo ratings yet
- Senile Cataract Clinical Presentation and CausesDocument4 pagesSenile Cataract Clinical Presentation and CausesAhmad Fahrozi100% (1)
- Ageing Eye Posterior Segment ChangesDocument6 pagesAgeing Eye Posterior Segment ChangesirijoaNo ratings yet
- Age-Related Cataract & GlaucomaDocument26 pagesAge-Related Cataract & Glaucomasweetyeyal2002No ratings yet
- Dry Eye Disease GuideDocument25 pagesDry Eye Disease Guide215045 zulfa laili aNo ratings yet
- Cataracts Seminar: Causes, Treatment, and Future OutlookDocument13 pagesCataracts Seminar: Causes, Treatment, and Future OutlookMacarena AlvarezNo ratings yet
- Article Wjpps 1533027420Document25 pagesArticle Wjpps 1533027420rahayuNo ratings yet
- Makrufa NWDocument6 pagesMakrufa NWPujiastutiNo ratings yet
- Retinal Detachments and The Current Trends of TreatmentDocument10 pagesRetinal Detachments and The Current Trends of Treatmentapi-235387260No ratings yet
- Catarac CongenitalDocument3 pagesCatarac CongenitalDicki Pratama HolmesNo ratings yet
- Childhood Cataracts: Aetiology and Management: Indian Supplement Editorial BoardDocument4 pagesChildhood Cataracts: Aetiology and Management: Indian Supplement Editorial Boardnugroho2212No ratings yet
- Holy 3Document3 pagesHoly 3Holy Fitria ArianiNo ratings yet
- Clinical and Experimental Advances in Congenital and Paediatric CataractsDocument16 pagesClinical and Experimental Advances in Congenital and Paediatric CataractsFitri Amelia RizkiNo ratings yet
- Standard Treatment Guidelines Opthalmology Author Dr. Venkatesh PrajnaDocument146 pagesStandard Treatment Guidelines Opthalmology Author Dr. Venkatesh PrajnaAriana BulaiNo ratings yet
- Cataract: Mohd Roslee Bin Abd GhaniDocument46 pagesCataract: Mohd Roslee Bin Abd GhaniSaha DirllahNo ratings yet
- Cataracts - Causes, Symptoms, Treatment, Surgery: Southern Cross Medical LibraryDocument6 pagesCataracts - Causes, Symptoms, Treatment, Surgery: Southern Cross Medical Librarypuskesmas sukorejoNo ratings yet
- Congenital Cataracts Causes, Symptoms and TreatmentDocument2 pagesCongenital Cataracts Causes, Symptoms and TreatmentKuchai BaruNo ratings yet
- Primary Retinal Detachment: Clinical PracticeDocument9 pagesPrimary Retinal Detachment: Clinical PracticeAdita DitaNo ratings yet
- Retinal Disorder Case StudyDocument6 pagesRetinal Disorder Case StudyGabbii CincoNo ratings yet
- Senile Cataract (Age-Related Cataract) - Practice Essentials, Background, PathophysiologyDocument5 pagesSenile Cataract (Age-Related Cataract) - Practice Essentials, Background, PathophysiologyAhmad FahroziNo ratings yet
- Protrusion OjoDocument16 pagesProtrusion OjoAntonio ReaNo ratings yet
- Floaters AbacaxiDocument14 pagesFloaters AbacaxiCristiano TavaresNo ratings yet
- F (GH) PF1 (VsuGH)Document5 pagesF (GH) PF1 (VsuGH)Vijay KautilyaNo ratings yet
- Keratoconus: Picture 1Document6 pagesKeratoconus: Picture 1BuiyiWongNo ratings yet
- Keratoconus: Picture 1Document6 pagesKeratoconus: Picture 1BuiyiWongNo ratings yet
- Jorge G Arroyo, MD, MPH Jonathan Trobe, MD Howard Libman, MD Contributor Disclosures Peer Review ProcessDocument13 pagesJorge G Arroyo, MD, MPH Jonathan Trobe, MD Howard Libman, MD Contributor Disclosures Peer Review ProcessLis Borda MuñozNo ratings yet
- A Cataract Is A Clouding of The EyeDocument5 pagesA Cataract Is A Clouding of The EyeHikari 光 ShidouNo ratings yet
- Cataract CasestudyDocument3 pagesCataract CasestudyJamal AgontongNo ratings yet
- Low Vision Manuscript Group 7Document13 pagesLow Vision Manuscript Group 7Jay JimenNo ratings yet
- ASKEP KATARAK m.2Document24 pagesASKEP KATARAK m.2Given MalelakNo ratings yet
- Retinal DetachmentDocument14 pagesRetinal DetachmentPui_Yee_Siow_6303No ratings yet
- Lens Iris Pupil Retina: Cataract OverviewDocument5 pagesLens Iris Pupil Retina: Cataract Overviewrizky_kurniawan_14No ratings yet
- New Management Strategies For Ectopia LentisDocument14 pagesNew Management Strategies For Ectopia LentisximoNo ratings yet
- Retinal Detachment Diagnosis and TreatmentDocument6 pagesRetinal Detachment Diagnosis and TreatmentDeasy Arindi PutriNo ratings yet
- Thesis On Refractive ErrorsDocument7 pagesThesis On Refractive ErrorsLuz Martinez100% (2)
- Yanoff DukerDocument8 pagesYanoff DukerFerdinando BaehaNo ratings yet
- Extracapsular Cataract Extraction (OR)Document4 pagesExtracapsular Cataract Extraction (OR)Jet-Jet GuillerganNo ratings yet
- What Is Macular Pucker, Epiretinal Membrane and Macular Pucker Surgery, Treatment, Recovery?Document2 pagesWhat Is Macular Pucker, Epiretinal Membrane and Macular Pucker Surgery, Treatment, Recovery?http://feelgoodtime.netNo ratings yet
- Primary Retinal DetachmentDocument9 pagesPrimary Retinal DetachmentMarviane ThenNo ratings yet
- Extracapsular Cataract Extraction (ECCE) Is A Category of Eye Surgery in WhichDocument13 pagesExtracapsular Cataract Extraction (ECCE) Is A Category of Eye Surgery in WhichMa Christina RabayaNo ratings yet
- Surgery 101: Managing Endothelial RiskDocument6 pagesSurgery 101: Managing Endothelial Riskmithaa octoviagnesNo ratings yet
- Cataract Surgery, 3rd Edition: PART VII - Management of Complications Chapter 49 - Corneal Edema After Cataract SurgeryDocument14 pagesCataract Surgery, 3rd Edition: PART VII - Management of Complications Chapter 49 - Corneal Edema After Cataract Surgerymithaa octoviagnesNo ratings yet
- Referat Vfloaters 1Document6 pagesReferat Vfloaters 1mithaa octoviagnesNo ratings yet
- Referat Vfloaters 1Document6 pagesReferat Vfloaters 1mithaa octoviagnesNo ratings yet
- 500 1 1000 1 10 20140203 PDFDocument4 pages500 1 1000 1 10 20140203 PDFAden SagaraNo ratings yet
- Emergency Fluid Therapy - Satriyo Dwi Suryantoro, DR., SP - PDDocument16 pagesEmergency Fluid Therapy - Satriyo Dwi Suryantoro, DR., SP - PDmithaa octoviagnesNo ratings yet
- Hermita Octoviagnes BuarleleDocument1 pageHermita Octoviagnes Buarlelemithaa octoviagnesNo ratings yet
- Ilmu Kesehatan Jiwa Rs Soeharto Heerdjan (Online Dan Offline/4 Minggu)Document1 pageIlmu Kesehatan Jiwa Rs Soeharto Heerdjan (Online Dan Offline/4 Minggu)mithaa octoviagnesNo ratings yet
- Ilmu Kesehatan Jiwa Rs Soeharto Heerdjan (Online Dan Offline/4 Minggu)Document1 pageIlmu Kesehatan Jiwa Rs Soeharto Heerdjan (Online Dan Offline/4 Minggu)mithaa octoviagnesNo ratings yet
- Stase 21 Oktober 2019 (Non Autogenerate)Document11 pagesStase 21 Oktober 2019 (Non Autogenerate)Ida Ayu DyahNo ratings yet
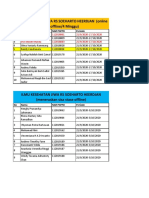
- Ilmu Penyakit Dalam Rsau Esnawan Antariksa: No Nama Nim PSPPD PeriodeDocument2 pagesIlmu Penyakit Dalam Rsau Esnawan Antariksa: No Nama Nim PSPPD Periodemithaa octoviagnesNo ratings yet
- EKG Arrhythmia Identification GuideDocument47 pagesEKG Arrhythmia Identification Guidemithaa octoviagnesNo ratings yet
- EKG Arrhythmia Identification GuideDocument47 pagesEKG Arrhythmia Identification Guidemithaa octoviagnesNo ratings yet
- Skenario 4 F2Document19 pagesSkenario 4 F2Anisa Aulia ReffidaNo ratings yet
- Anapath - Dr. Saad Khairallah - Session 1Document5 pagesAnapath - Dr. Saad Khairallah - Session 1Nagham BazziNo ratings yet
- Actron CP9449 User ManualDocument58 pagesActron CP9449 User ManualMichael BongioviNo ratings yet
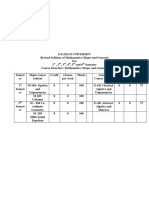
- TDC - Syllabus Mathematics PDFDocument32 pagesTDC - Syllabus Mathematics PDFAnanta PaulNo ratings yet
- 148 Lalgarh Colony, Dum Dum, Kolkata-74 Near Lalgarh Primary School Saraswati Apt. Ground FLOOR - 700074Document14 pages148 Lalgarh Colony, Dum Dum, Kolkata-74 Near Lalgarh Primary School Saraswati Apt. Ground FLOOR - 700074arkaprava paulNo ratings yet
- Adjectives Interconversion of The Degrees of Comparison (Worksheet 3-) Rewrite Each Sentence Using The Other Two Degrees of ComparisonDocument2 pagesAdjectives Interconversion of The Degrees of Comparison (Worksheet 3-) Rewrite Each Sentence Using The Other Two Degrees of ComparisonJeanNo ratings yet
- Caring in Nursing: Four AspectsDocument47 pagesCaring in Nursing: Four AspectsAnuchithra RadhakrishnanNo ratings yet
- ENGLSIH LISTENING SKILLS (Question Paper) PDFDocument2 pagesENGLSIH LISTENING SKILLS (Question Paper) PDFGagan H RNo ratings yet
- Lesson Two AcademicDocument2 pagesLesson Two Academicapi-207515585No ratings yet
- Swami Vivekananda's 1893 Chicago Speech on Religious UnityDocument2 pagesSwami Vivekananda's 1893 Chicago Speech on Religious UnityBiplab MahantiNo ratings yet
- Use of Imagery in Look Back in AngerDocument3 pagesUse of Imagery in Look Back in AngerArindam SenNo ratings yet
- Protocol for managing pesticide poisoningDocument6 pagesProtocol for managing pesticide poisoningJesicca SNo ratings yet
- Merchant Banking Roles and FunctionsDocument18 pagesMerchant Banking Roles and Functionssunita prabhakarNo ratings yet
- The Flower of Services A Study On Private Universities in Sylhet CityDocument11 pagesThe Flower of Services A Study On Private Universities in Sylhet CityLatif AbdulNo ratings yet
- Harry Potter Essay 1 OutlineDocument10 pagesHarry Potter Essay 1 OutlinevickaduzerNo ratings yet
- Lab Manual: CSC-216 (L8) - Data StructuresDocument7 pagesLab Manual: CSC-216 (L8) - Data StructuresAbid KhanNo ratings yet
- Labor 2 CasesDocument77 pagesLabor 2 CasesMercado MarloNo ratings yet
- Polymerization Synthesis of Nylon 6,10 C11!5!22Document8 pagesPolymerization Synthesis of Nylon 6,10 C11!5!22Ade YusraNo ratings yet
- Elecius Franklin IndictmentDocument2 pagesElecius Franklin Indictmentthe kingfishNo ratings yet
- JO1 Plar GIE and MIEDocument2 pagesJO1 Plar GIE and MIEKaloy PlarNo ratings yet
- Developing The Assessment Instrument of SpeakingDocument11 pagesDeveloping The Assessment Instrument of Speakingifdol pentagenNo ratings yet
- E-Commerce and Enterprise SystemsDocument19 pagesE-Commerce and Enterprise SystemsMaria Angela B. GalvezNo ratings yet