You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5819)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (845)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Lesson Plan - HPVDocument6 pagesLesson Plan - HPVMonique MavronicolasNo ratings yet
- College of Our Lady of Mt. Carmel (Pampanga) : Course SyllabusDocument4 pagesCollege of Our Lady of Mt. Carmel (Pampanga) : Course Syllabus;'SiLeNt';No ratings yet
- Newly Diagnosed HIV Cases in The Philippines: National Epidemiology CenterDocument4 pagesNewly Diagnosed HIV Cases in The Philippines: National Epidemiology CenterDeden DavidNo ratings yet
- Immunization ChartDocument1 pageImmunization ChartDesilva ThampiNo ratings yet
- Journal of Obstetrics and Gynaecology Canada (JOGC) PDFDocument7 pagesJournal of Obstetrics and Gynaecology Canada (JOGC) PDFgilirNo ratings yet
- An Analysis of Taiwan's Vaccination Services and Applications For Vaccine Injury CompensationsDocument15 pagesAn Analysis of Taiwan's Vaccination Services and Applications For Vaccine Injury CompensationsAnonymous FNZ3uR2AHsNo ratings yet
- Gavrila Catalin 1Document1 pageGavrila Catalin 1Doina RusuNo ratings yet
- K.N.ravichitra, Et AlDocument5 pagesK.N.ravichitra, Et AldindaNo ratings yet
- Bacteriology Ii MCQ:: Prepared By: Srey Viso, Pharmd Medical Biologist & Microbiology, DMM For Pharmacy ClassDocument21 pagesBacteriology Ii MCQ:: Prepared By: Srey Viso, Pharmd Medical Biologist & Microbiology, DMM For Pharmacy ClassPiseth VichhekaNo ratings yet
- Antiviral Therapy PDFDocument438 pagesAntiviral Therapy PDFYOUCEF DHIA ELHAK KOUAOUCINo ratings yet
- Daftar Pustaka Fix GbsDocument2 pagesDaftar Pustaka Fix GbsElizabeth IvanaNo ratings yet
- Zoonoses: Drs. Foster & Smith Educational StaffDocument7 pagesZoonoses: Drs. Foster & Smith Educational StaffTINALEETNT723No ratings yet
- 21-05-2020 05-00 EnglishDocument13 pages21-05-2020 05-00 EnglishRohithNo ratings yet
- VIKKI13Document6 pagesVIKKI13Dillisrinivasarao NNo ratings yet
- Objectives 3Document4 pagesObjectives 3sibugan300No ratings yet
- IMSLP664696-PMLP1066603-The Dilemma All Clarinet Version-Score and PartsDocument12 pagesIMSLP664696-PMLP1066603-The Dilemma All Clarinet Version-Score and PartsJoseph RouquetteNo ratings yet
- Leptospirosis by DR SarmaDocument37 pagesLeptospirosis by DR SarmaTias Diah0% (1)
- Alterations With Infectious Inflammatory and Immunologic ResponseDocument15 pagesAlterations With Infectious Inflammatory and Immunologic Responselaurie.charlynjaneNo ratings yet
- VIRUSESDocument7 pagesVIRUSESJitesh SoniNo ratings yet
- The Correlation Between Basic Immunizations Knowledge and Mothers' Attitude at Basic Immunizations Provision in The House of Vaccination KebagusanDocument1 pageThe Correlation Between Basic Immunizations Knowledge and Mothers' Attitude at Basic Immunizations Provision in The House of Vaccination KebagusanMuhammad Agung WNo ratings yet
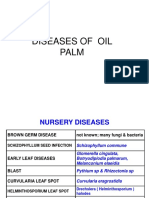
- Diseases of Oil Palm Pictures PpsDocument42 pagesDiseases of Oil Palm Pictures Ppsgafrnce60No ratings yet
- Cutaneous Leishmaniasis: Mark S. Bailey, MRCP, Diana N.J. Lockwood, BSC, MD, FRCPDocument9 pagesCutaneous Leishmaniasis: Mark S. Bailey, MRCP, Diana N.J. Lockwood, BSC, MD, FRCPeva yustianaNo ratings yet
- On The Day of Big Annual SaleDocument7 pagesOn The Day of Big Annual SaleSutin SirisaoNo ratings yet
- Microbial Diseases of The Cardiovascular and Lymphatic SystemsDocument27 pagesMicrobial Diseases of The Cardiovascular and Lymphatic SystemsAbhishek Isaac MathewNo ratings yet
- CarbunclesDocument15 pagesCarbunclesMr DanielNo ratings yet
- Mukesh Kumar,: Municipal CommissionerDocument6 pagesMukesh Kumar,: Municipal CommissionerSSNo ratings yet
- Lymphatic Filariasis SummaryDocument6 pagesLymphatic Filariasis Summaryapi-252809746No ratings yet
- Laboratory Report:: Shaynad Ambalathveettil SharafudheenDocument1 pageLaboratory Report:: Shaynad Ambalathveettil Sharafudheenshaynad binsharafNo ratings yet
- AnaplasmaDocument22 pagesAnaplasmaSomesh SharmaNo ratings yet
- National Immunisation ProgrammeDocument2 pagesNational Immunisation ProgrammeAnonymous whcvnPBeQNo ratings yet