You might also like
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Epidemiology of Mandibular Fractures Treated at Chiang Mai University Hospital: A Review of 198 CasesDocument7 pagesThe Epidemiology of Mandibular Fractures Treated at Chiang Mai University Hospital: A Review of 198 CasesMohammed TarekNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Oral Surgery - Dr. Labeed SamiDocument22 pagesOral Surgery - Dr. Labeed SamiMohammed TarekNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Management of A Bilateral Mandibular Fracture in A Single-Humped CamelDocument4 pagesManagement of A Bilateral Mandibular Fracture in A Single-Humped CamelMohammed TarekNo ratings yet
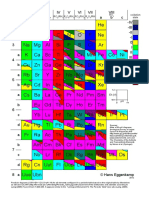
- Mendeleev's Periodic Table of The ElementsDocument20 pagesMendeleev's Periodic Table of The ElementsMohammed TarekNo ratings yet
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- R O RO R O RO /RH R O /RH RO /RH R O /RH RO Oxidation StateDocument1 pageR O RO R O RO /RH R O /RH RO /RH R O /RH RO Oxidation StateMohammed TarekNo ratings yet
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Relationship Between Mandible Fractures and Third Molars: Archives of Craniofacial SurgeryDocument6 pagesRelationship Between Mandible Fractures and Third Molars: Archives of Craniofacial SurgeryMohammed TarekNo ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- 3A The Periodic TableDocument7 pages3A The Periodic TableMohammed TarekNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Metabolic Changes by Wine Flor-Yeasts With Gluconic Acid As The Sole Carbon SourceDocument15 pagesMetabolic Changes by Wine Flor-Yeasts With Gluconic Acid As The Sole Carbon SourceMohammed TarekNo ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Introduction To Endocrine Disrupting ChemicalsDocument76 pagesIntroduction To Endocrine Disrupting ChemicalsMohammed TarekNo ratings yet
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Endo EngDocument107 pagesEndo EngMohammed TarekNo ratings yet
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Artigo18 APSerro ManuscriptDocument19 pagesArtigo18 APSerro ManuscriptMohammed TarekNo ratings yet
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- EndoDocument1 pageEndoMohammed TarekNo ratings yet
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Bleach InstructionsDocument9 pagesBleach InstructionsMohammed TarekNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Library Book List - ENDO, CONSE, NEW, JOURNALSDocument10 pagesLibrary Book List - ENDO, CONSE, NEW, JOURNALSMohammed TarekNo ratings yet
- Q.P.CODE: 430/410: Conservative Dentistry and EndodonticsDocument18 pagesQ.P.CODE: 430/410: Conservative Dentistry and EndodonticsMohammed TarekNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- IFEA IES Endodontic and Dental Practice During COVID-19Document24 pagesIFEA IES Endodontic and Dental Practice During COVID-19Mohammed TarekNo ratings yet
- Long Life, Aluminum Electrolytic: Capacitance Range Capacitance Tolerance Rated Voltage Operating Temperature RangeDocument8 pagesLong Life, Aluminum Electrolytic: Capacitance Range Capacitance Tolerance Rated Voltage Operating Temperature RangeMohammed TarekNo ratings yet
- Human Teeth vs. Animal Teeth PPT (Student Version)Document22 pagesHuman Teeth vs. Animal Teeth PPT (Student Version)Allison LeCoq75% (8)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- BookletDocument115 pagesBookletRoyal CureNo ratings yet
- Principles and Practice of Implant Dentistry 2001 - Weiss (18-15)Document671 pagesPrinciples and Practice of Implant Dentistry 2001 - Weiss (18-15)jktrj100% (1)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Radiography of Facial Bones & PNS.: ModeratorDocument67 pagesRadiography of Facial Bones & PNS.: ModeratorMunish DograNo ratings yet
- Alamat Molars PaskalDocument1 pageAlamat Molars PaskalElsa ChristinaNo ratings yet
- Type of Post and CoreDocument9 pagesType of Post and CoreErliTa TyarLieNo ratings yet
- M-i-M For DME Matrix-In-A-Matrix Technique For Deep Margin ElevationDocument5 pagesM-i-M For DME Matrix-In-A-Matrix Technique For Deep Margin Elevationfernando vicente100% (1)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Local Anaesthesia in EndodonticsDocument76 pagesLocal Anaesthesia in Endodonticssaurav kumar duttaNo ratings yet
- Precision in Dental Esthetics PDFDocument463 pagesPrecision in Dental Esthetics PDFTeodor Baciu50% (2)
- Oral Rehabilitation Patient InjuriesDocument7 pagesOral Rehabilitation Patient InjuriesAlexandru Codrin-IonutNo ratings yet
- Gear-Tip Relief PDFDocument1 pageGear-Tip Relief PDFSyedNo ratings yet
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Toothbrush Life Cycle Analysis: by Suzy MartinDocument11 pagesToothbrush Life Cycle Analysis: by Suzy Martinapi-25886761100% (1)
- All Ceramic Inlays and Onlays For Posterior TeethDocument11 pagesAll Ceramic Inlays and Onlays For Posterior TeethNajeeb Ullah100% (1)
- Lip Reposition Surgery A New Call in PeriodonticsDocument4 pagesLip Reposition Surgery A New Call in PeriodonticsMaysaa mahdiNo ratings yet
- Advance Statistics ProjectDocument9 pagesAdvance Statistics Projectrishit100% (7)
- (PLM) Oral Cavity Salivary Glands Pharynx and EsophagusDocument9 pages(PLM) Oral Cavity Salivary Glands Pharynx and EsophagusJovilyn SilongaNo ratings yet
- 10 Herbs To The Rescue PDFDocument1 page10 Herbs To The Rescue PDFAriel LopezNo ratings yet
- 2 - Human Dentition IntroDocument71 pages2 - Human Dentition IntroozyiamandsNo ratings yet
- Definition:: RetentionDocument39 pagesDefinition:: RetentiontirathramNo ratings yet
- 2016 Endocrown Restorations - A Systematic Review and Meta-AnalysisDocument7 pages2016 Endocrown Restorations - A Systematic Review and Meta-Analysisitzel lopezNo ratings yet
- Reviews: Case Reports in Pediatric DentistryDocument1 pageReviews: Case Reports in Pediatric DentistryYaser JasNo ratings yet
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- GIT PhysiologyDocument27 pagesGIT PhysiologyMohamed AdnanNo ratings yet
- Self-Assessment Tool For Infection Control: First EditionDocument34 pagesSelf-Assessment Tool For Infection Control: First EditionEm EryNo ratings yet
- MDNSDocument7 pagesMDNSRamon HipolitoNo ratings yet
- SR Ivocap System: EN Instructions For UseDocument44 pagesSR Ivocap System: EN Instructions For Useumerjaved86No ratings yet
- Cleftlipandpalate: Mitchell L. Worley,, Krishna G. Patel,, Lauren A. KilpatrickDocument18 pagesCleftlipandpalate: Mitchell L. Worley,, Krishna G. Patel,, Lauren A. KilpatrickYerly Ramirez Muñoz100% (1)
- SoniCare Toothbrush HX681ADocument72 pagesSoniCare Toothbrush HX681Agschlachter2No ratings yet
- 10.epidemiology of Malocclusion PDFDocument5 pages10.epidemiology of Malocclusion PDFhassankhan9849No ratings yet
- The K Test and The Condylar Test by AlmuzianDocument5 pagesThe K Test and The Condylar Test by AlmuzianRahulLife'sNo ratings yet
- Guidelines for Chemical Process Quantitative Risk AnalysisFrom EverandGuidelines for Chemical Process Quantitative Risk AnalysisRating: 5 out of 5 stars5/5 (1)
- Sodium Bicarbonate: Nature's Unique First Aid RemedyFrom EverandSodium Bicarbonate: Nature's Unique First Aid RemedyRating: 5 out of 5 stars5/5 (21)