You might also like
- Os Finals ReviewerDocument33 pagesOs Finals ReviewerGuen ColisNo ratings yet
- Peri-Implant Complications: A Clinical Guide to Diagnosis and TreatmentFrom EverandPeri-Implant Complications: A Clinical Guide to Diagnosis and TreatmentNo ratings yet
- 3 Fractures of The Mandible - Salwan - Bede Salwan - BedeDocument16 pages3 Fractures of The Mandible - Salwan - Bede Salwan - Bedeammar slimanNo ratings yet
- Root FracturesDocument9 pagesRoot FracturesAbhilashPadmanabhanNo ratings yet
- Maxillofacial Prosthesis IntroductionDocument65 pagesMaxillofacial Prosthesis IntroductionRishabh Madhu Sharan100% (2)
- Skeletally-Anchored Maxillary Expansion: Promising Effects and LimitationsDocument23 pagesSkeletally-Anchored Maxillary Expansion: Promising Effects and LimitationsAya ElsayedNo ratings yet
- Root Fracture Diagnosis TreatmentDocument9 pagesRoot Fracture Diagnosis Treatmentemchen11No ratings yet
- Lec 2 3Document94 pagesLec 2 3Batool SamiNo ratings yet
- Trauma Q&ADocument8 pagesTrauma Q&ANoor MaxeemNo ratings yet
- Mandibular Condylar and Subcondylar Fractures PDFDocument16 pagesMandibular Condylar and Subcondylar Fractures PDFWayan Sutresna YasaNo ratings yet
- Mandibular FracturesDocument46 pagesMandibular FracturesAntony Sebastian100% (1)
- 501 Surgery AssignmentDocument6 pages501 Surgery AssignmentAhmed YousryNo ratings yet
- Management of Facial FracturesDocument35 pagesManagement of Facial FracturesIma OhwNo ratings yet
- Maxillary Transverse DeficiencyDocument4 pagesMaxillary Transverse DeficiencyCarlos Alberto CastañedaNo ratings yet
- Jaw Surgery: Robert M. Menard, Nikhil K. DesaiDocument10 pagesJaw Surgery: Robert M. Menard, Nikhil K. DesaiAlain AguirreNo ratings yet
- MANAGEMENT OF MANDIBULAR FRACTURES - Ghiffar Oka Prihardian - 18700062Document22 pagesMANAGEMENT OF MANDIBULAR FRACTURES - Ghiffar Oka Prihardian - 18700062fransiscaNo ratings yet
- 501 Surgery AssignmentDocument4 pages501 Surgery AssignmentAhmed YousryNo ratings yet
- Li LBM 4 Blok 18 AnggunDocument8 pagesLi LBM 4 Blok 18 AnggunAnggun Amanda SaveriiaNo ratings yet
- Oral and Maxillofacial Surgery/fifth Year Fractures of The Middle Third of The Facial SkeletonDocument19 pagesOral and Maxillofacial Surgery/fifth Year Fractures of The Middle Third of The Facial SkeletonHussein ShumranNo ratings yet
- Carlino 2019Document9 pagesCarlino 2019Isabella WilkeNo ratings yet
- Mandibular FracturesDocument171 pagesMandibular FracturesBalen ShalawNo ratings yet
- Orthodontic Lect 26Document11 pagesOrthodontic Lect 26Said SaidNo ratings yet
- Research Journal of Pharmaceutical, Biological and Chemical SciencesDocument7 pagesResearch Journal of Pharmaceutical, Biological and Chemical SciencesIndah GitaswariNo ratings yet
- Symphysis and Corpus Mandible Fracture: Mgs. Puji Wahid Farhan Muhammad Ilmu Bedah, 2006624892Document18 pagesSymphysis and Corpus Mandible Fracture: Mgs. Puji Wahid Farhan Muhammad Ilmu Bedah, 2006624892Erwan Ahmad DNo ratings yet
- Jurnal 3 WordDocument6 pagesJurnal 3 WordlindaNo ratings yet
- Maxillary Fractures: ©1997 Erlanger Health System Tennessee Craniofacial Center 1 (800) 418-3223Document4 pagesMaxillary Fractures: ©1997 Erlanger Health System Tennessee Craniofacial Center 1 (800) 418-3223Aristiyan LuthfiNo ratings yet
- Midline Shift / Orthodontic Courses by Indian Dental AcademyDocument100 pagesMidline Shift / Orthodontic Courses by Indian Dental Academyindian dental academy100% (1)
- Comparison of Orthodontic Techniques Used ForDocument5 pagesComparison of Orthodontic Techniques Used ForAdina SerbanNo ratings yet
- Lec12 4th ClassDocument8 pagesLec12 4th ClassYaser JasNo ratings yet
- Odonto MaDocument5 pagesOdonto MaashariNo ratings yet
- Mandible Fracture - Compiled by Danesh-1Document3 pagesMandible Fracture - Compiled by Danesh-1daneshkumarytcNo ratings yet
- 3 (Fractures of The Middle Third)Document84 pages3 (Fractures of The Middle Third)sara.kattan22No ratings yet
- Orthognathic Surgery RonalDocument56 pagesOrthognathic Surgery Ronaldrghempik100% (2)
- AnemiaDocument9 pagesAnemiaManjeevNo ratings yet
- CraniomaDocument7 pagesCraniomaSophia BeecherNo ratings yet
- A Radiolucency Is The Darker Area Within A Bone On A Conventional RadiographDocument83 pagesA Radiolucency Is The Darker Area Within A Bone On A Conventional Radiographkabir shaikhNo ratings yet
- Ten Facts About Dental Implants: September-October 2016 - No. 5, Vol. 6 P D WWW - Dental-Tribune - MeDocument4 pagesTen Facts About Dental Implants: September-October 2016 - No. 5, Vol. 6 P D WWW - Dental-Tribune - Mefreddybot89No ratings yet
- Mandibular ImpactionDocument51 pagesMandibular ImpactionNikkoCataquizNo ratings yet
- Sidharth Text PptDocument12 pagesSidharth Text PptNikesh KumarNo ratings yet
- Exostosis MandibularDocument6 pagesExostosis MandibularCOne Gomez LinarteNo ratings yet
- Mandibular FracturesDocument67 pagesMandibular FracturesAbel AbrahamNo ratings yet
- Management of Mandibular Fracture by Dr. Bethan JonesDocument31 pagesManagement of Mandibular Fracture by Dr. Bethan JonesAndykaYayanSetiawanNo ratings yet
- 7 Maxillofacial TraumaaDocument36 pages7 Maxillofacial TraumaaAhed ShaerNo ratings yet
- Unilateral subcondylar fracture treated by close reductionDocument3 pagesUnilateral subcondylar fracture treated by close reductionAlbertine JaneNo ratings yet
- MISCH: CHAPTER 12 PREIMPLANT PROSTHODONTICSDocument51 pagesMISCH: CHAPTER 12 PREIMPLANT PROSTHODONTICSNaresh TeresNo ratings yet
- Occlusion 26 / Orthodontic Courses by Indian Dental AcademyDocument77 pagesOcclusion 26 / Orthodontic Courses by Indian Dental Academyindian dental academy100% (1)
- On ImpactionDocument44 pagesOn Impactionmesssi269No ratings yet
- Preprosthetic Surgery 12-02-015 PDFDocument32 pagesPreprosthetic Surgery 12-02-015 PDFguhanderNo ratings yet
- Rehabilitation of maxillary defectsDocument67 pagesRehabilitation of maxillary defectspriyaNo ratings yet
- Mandible Alveolar Fractures Treatment GuideDocument7 pagesMandible Alveolar Fractures Treatment GuideNiero GalangNo ratings yet
- Management of Mandibular FractureDocument13 pagesManagement of Mandibular FractureAnonymous WtgTCQJdNNo ratings yet
- Maxillofacial Trauma and Management - Dental Ebook & Lecture Notes PDF Download (Studynama - Com - India's Biggest Website For BDS Study Material Downloads)Document24 pagesMaxillofacial Trauma and Management - Dental Ebook & Lecture Notes PDF Download (Studynama - Com - India's Biggest Website For BDS Study Material Downloads)Vinnie SinghNo ratings yet
- Dental ImplantDocument34 pagesDental Implantjuren.zafat.05No ratings yet
- Maxillomandibular DefectsDocument114 pagesMaxillomandibular DefectsSahana Rangarajan100% (1)
- Class I and Class II MalocclusionDocument13 pagesClass I and Class II MalocclusionmelNo ratings yet
- Closed Reduction Treatment Parasimfisis (Ada Radriograf), Dan Tata LaksananyaDocument7 pagesClosed Reduction Treatment Parasimfisis (Ada Radriograf), Dan Tata LaksananyaVincent AriesNo ratings yet
- Mandibular FracturesDocument33 pagesMandibular FracturesDrMuskan AroraNo ratings yet
- Combination SyndroneDocument5 pagesCombination SyndroneAmar BhochhibhoyaNo ratings yet
- Case Report: Bhandari PPDocument2 pagesCase Report: Bhandari PPEgiNo ratings yet
- Hospitalised Sports Injury in Australia, 2016-17: Published February 2020Document20 pagesHospitalised Sports Injury in Australia, 2016-17: Published February 2020Mohammed TarekNo ratings yet
- Relationship Between Mandible Fractures and Third Molars: Archives of Craniofacial SurgeryDocument6 pagesRelationship Between Mandible Fractures and Third Molars: Archives of Craniofacial SurgeryMohammed TarekNo ratings yet
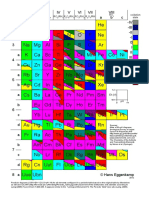
- R O RO R O RO /RH R O /RH RO /RH R O /RH RO Oxidation StateDocument1 pageR O RO R O RO /RH R O /RH RO /RH R O /RH RO Oxidation StateMohammed TarekNo ratings yet
- The Epidemiology of Mandibular Fractures Treated at Chiang Mai University Hospital: A Review of 198 CasesDocument7 pagesThe Epidemiology of Mandibular Fractures Treated at Chiang Mai University Hospital: A Review of 198 CasesMohammed TarekNo ratings yet
- Management of A Bilateral Mandibular Fracture in A Single-Humped CamelDocument4 pagesManagement of A Bilateral Mandibular Fracture in A Single-Humped CamelMohammed TarekNo ratings yet
- Introduction to Computers and C++ Programming ChapterDocument38 pagesIntroduction to Computers and C++ Programming Chapterken lacedaNo ratings yet
- Tierny Visualization Introductionc++Document26 pagesTierny Visualization Introductionc++DurandNo ratings yet
- Periodic Table IsotopesDocument1 pagePeriodic Table IsotopeslamantreveurNo ratings yet
- 3A The Periodic TableDocument7 pages3A The Periodic TableMohammed TarekNo ratings yet
- Mendeleev's Periodic Table of The ElementsDocument20 pagesMendeleev's Periodic Table of The ElementsMohammed TarekNo ratings yet
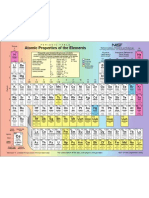
- Atomic Properties of The Elements TableDocument1 pageAtomic Properties of The Elements TableMaahiNo ratings yet
- HPS Per Table With SPDF Ions and Families To PostDocument87 pagesHPS Per Table With SPDF Ions and Families To PostMohammed TarekNo ratings yet
- PDDocument1 pagePDMohammed TarekNo ratings yet
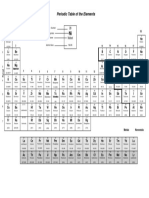
- Periodic Table of The Elements: Atomic Number Symbol NameDocument1 pagePeriodic Table of The Elements: Atomic Number Symbol Namechen haoNo ratings yet
- Computer10to12 2008 PDFDocument72 pagesComputer10to12 2008 PDFA YoungeNo ratings yet
- Mendeleev's Periodic Table of The ElementsDocument20 pagesMendeleev's Periodic Table of The ElementsMohammed TarekNo ratings yet
- MR Robot 1x01 - PilotDocument64 pagesMR Robot 1x01 - Pilotchosen_one_dtnNo ratings yet
- Introduction To Endocrine Disrupting ChemicalsDocument76 pagesIntroduction To Endocrine Disrupting ChemicalsMohammed TarekNo ratings yet
- Endo EngDocument107 pagesEndo EngMohammed TarekNo ratings yet
- Material de ApoyoDocument57 pagesMaterial de ApoyoALEXANDER MONDRAGON DIAZNo ratings yet
- EndoDocument1 pageEndoMohammed TarekNo ratings yet
- ERN On Endocrine Conditions (Endo-ERN)Document1 pageERN On Endocrine Conditions (Endo-ERN)Mohammed TarekNo ratings yet
- Metabolic Changes by Wine Flor-Yeasts With Gluconic Acid As The Sole Carbon SourceDocument15 pagesMetabolic Changes by Wine Flor-Yeasts With Gluconic Acid As The Sole Carbon SourceMohammed TarekNo ratings yet
- CC - MVSA0147 Report Great Barrier Reef - V4 FA - Low Res - Single PagesDocument32 pagesCC - MVSA0147 Report Great Barrier Reef - V4 FA - Low Res - Single PagesMohammed TarekNo ratings yet
- 1462 PDFDocument5 pages1462 PDFMohammed TarekNo ratings yet
- Chlorine Bleach Sanitizing GuideDocument2 pagesChlorine Bleach Sanitizing GuidearjmandquestNo ratings yet
- ENDO Agar: Mode of Action LiteratureDocument2 pagesENDO Agar: Mode of Action LiteratureadiazcalidadNo ratings yet
- Tooth Bleaching - Tooth Whitening (May 2013) (SHC 8782)Document19 pagesTooth Bleaching - Tooth Whitening (May 2013) (SHC 8782)Mohammed TarekNo ratings yet
- Research Article: Characterization, Acid Activation, and Bleaching Performance of Ibeshe Clay, Lagos, NigeriaDocument6 pagesResearch Article: Characterization, Acid Activation, and Bleaching Performance of Ibeshe Clay, Lagos, NigeriarmburraNo ratings yet
- Midterms LAB Working Length DeterminationDocument3 pagesMidterms LAB Working Length DeterminationBea YmsnNo ratings yet
- Structure and Properties of Enamel and DentinDocument17 pagesStructure and Properties of Enamel and DentinFile SeffinaNo ratings yet
- Extraction of Maxillary Teeth Using Articaine Without A Palatal InjectionDocument5 pagesExtraction of Maxillary Teeth Using Articaine Without A Palatal InjectionAhmadH.MahdiNo ratings yet
- History of ProsthodonticsDocument121 pagesHistory of ProsthodonticsArthi Ramalingam aNo ratings yet
- Final Exam. PRS 412 27 / 1 / 2017: Faculty of Dentistry Removable Prosthodontics DepartmentDocument11 pagesFinal Exam. PRS 412 27 / 1 / 2017: Faculty of Dentistry Removable Prosthodontics DepartmentHassan TantawyNo ratings yet
- Ijomi 2017 Vol 32 P 1296 1307Document12 pagesIjomi 2017 Vol 32 P 1296 1307John MacioNo ratings yet
- The Tooth Fairies' LessonDocument21 pagesThe Tooth Fairies' LessonAmaNie AieMira Junainah RosminNo ratings yet
- Sunday School Week 3.Document3 pagesSunday School Week 3.Jameson CrusperoNo ratings yet
- The Normal PeriodontiumDocument38 pagesThe Normal PeriodontiumAlex HaileyesusNo ratings yet
- The Effectiveness of Stem Cells Grafting On Regeneration of Dental Pulp: A Systematic Review and Meta-AnalysisDocument11 pagesThe Effectiveness of Stem Cells Grafting On Regeneration of Dental Pulp: A Systematic Review and Meta-AnalysisIJAR JOURNALNo ratings yet
- Scope of Endodontics: Regenerative Endodontics: AAE Position StatementDocument3 pagesScope of Endodontics: Regenerative Endodontics: AAE Position StatementPuneet ChahalNo ratings yet
- Principles of Designing Mucoperiosteal FlapsDocument70 pagesPrinciples of Designing Mucoperiosteal FlapsStephen KinyanjuiNo ratings yet
- Frenulum ChildDocument5 pagesFrenulum ChildPutriNo ratings yet
- Zygomatic ImplantDocument18 pagesZygomatic ImplantsmritinarayanNo ratings yet
- Mingival Curettage PDFDocument52 pagesMingival Curettage PDFheycoolalexNo ratings yet
- Optimizing Smile Composition and Esthetics With Resin Composites and Other Conservative Esthetic ProceduresDocument16 pagesOptimizing Smile Composition and Esthetics With Resin Composites and Other Conservative Esthetic ProceduresTiagoNo ratings yet
- Vita 1908e 50 Jahre Vita Metall Keramik Ps en v01Document23 pagesVita 1908e 50 Jahre Vita Metall Keramik Ps en v01Denis da Silveira NascimentoNo ratings yet
- Antimicrobial Mouthwash - Google SearchDocument1 pageAntimicrobial Mouthwash - Google Searchbruce kNo ratings yet
- Selvaratnam2009 PDFDocument23 pagesSelvaratnam2009 PDFKinjal SharmaNo ratings yet
- Sundqvist, G. (1976) Bacteriological Studies of Necrotic Dental Pulps. Umea University, Umea.Document101 pagesSundqvist, G. (1976) Bacteriological Studies of Necrotic Dental Pulps. Umea University, Umea.Jaime BarraganNo ratings yet
- 1.postnatal Growth and DevelopmentDocument135 pages1.postnatal Growth and DevelopmentAJPEDO LIFENo ratings yet
- Plaqueandtartar PDFDocument2 pagesPlaqueandtartar PDFRavi MuruganNo ratings yet
- An Orthopantomographic Study of Hypodontia in Permanent Teeth of Japanese Pediatric PatientsDocument8 pagesAn Orthopantomographic Study of Hypodontia in Permanent Teeth of Japanese Pediatric PatientsMariaCristinaNo ratings yet
- Main - Form Doc13 345 Abnormal Involuntary Movement Scale Aims WashingtonDocument2 pagesMain - Form Doc13 345 Abnormal Involuntary Movement Scale Aims WashingtonMuhammad Naqvi Al FarisiNo ratings yet
- Jones&Sadler 2012 ReviewDocument10 pagesJones&Sadler 2012 ReviewSidra ZahoorNo ratings yet
- The EnamelDocument27 pagesThe EnamelYousef KhallafNo ratings yet
- Torque in OrthodonticsDocument157 pagesTorque in Orthodonticsdeepankar sarkarNo ratings yet
- Survival of Dental Implants at Sites After Implant Failure: A Systematic ReviewDocument7 pagesSurvival of Dental Implants at Sites After Implant Failure: A Systematic ReviewNetra TaleleNo ratings yet
- cysts 1-مدمجDocument306 pagescysts 1-مدمجأمال داودNo ratings yet
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (402)
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (14)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 5 out of 5 stars5/5 (78)
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 3.5 out of 5 stars3.5/5 (2)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsRating: 5 out of 5 stars5/5 (1)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsFrom EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo ratings yet
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsFrom EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsRating: 4.5 out of 5 stars4.5/5 (169)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeNo ratings yet
- Techniques Exercises And Tricks For Memory ImprovementFrom EverandTechniques Exercises And Tricks For Memory ImprovementRating: 4.5 out of 5 stars4.5/5 (40)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisFrom EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (1)
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 5 out of 5 stars5/5 (4)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 3.5 out of 5 stars3.5/5 (3)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisFrom EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisRating: 4.5 out of 5 stars4.5/5 (42)
- The Ultimate Guide To Memory Improvement TechniquesFrom EverandThe Ultimate Guide To Memory Improvement TechniquesRating: 5 out of 5 stars5/5 (34)
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingFrom EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingRating: 5 out of 5 stars5/5 (5)
- The Happiness Trap: How to Stop Struggling and Start LivingFrom EverandThe Happiness Trap: How to Stop Struggling and Start LivingRating: 4 out of 5 stars4/5 (1)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.From EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Rating: 4.5 out of 5 stars4.5/5 (110)
- The Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsFrom EverandThe Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsNo ratings yet
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessFrom EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessRating: 4.5 out of 5 stars4.5/5 (327)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeFrom EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeRating: 4.5 out of 5 stars4.5/5 (253)
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingFrom EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingRating: 3.5 out of 5 stars3.5/5 (33)
- Daniel Kahneman's "Thinking Fast and Slow": A Macat AnalysisFrom EverandDaniel Kahneman's "Thinking Fast and Slow": A Macat AnalysisRating: 3.5 out of 5 stars3.5/5 (130)
- Summary: It Didn't Start with You: How Inherited Family Trauma Shapes Who We Are and How to End the Cycle By Mark Wolynn: Key Takeaways, Summary & AnalysisFrom EverandSummary: It Didn't Start with You: How Inherited Family Trauma Shapes Who We Are and How to End the Cycle By Mark Wolynn: Key Takeaways, Summary & AnalysisRating: 5 out of 5 stars5/5 (3)