You might also like
- Fixed Orthodontic Appliances: A Practical GuideFrom EverandFixed Orthodontic Appliances: A Practical GuideRating: 1 out of 5 stars1/5 (1)
- Growth of Maxilla OrthoDocument31 pagesGrowth of Maxilla OrthoFourthMolar.comNo ratings yet
- Pediatric Dentistry: Fourth EditionDocument6 pagesPediatric Dentistry: Fourth EditionFadiaNo ratings yet
- Development of Occlusion: Gum Pads StageDocument5 pagesDevelopment of Occlusion: Gum Pads StageSaid SaidNo ratings yet
- Complete Denture Prosthodontics in Children With Ectodermal DysplasiaDocument29 pagesComplete Denture Prosthodontics in Children With Ectodermal DysplasiaAmit BhargavNo ratings yet
- Facemask treatment of Class III malocclusionDocument31 pagesFacemask treatment of Class III malocclusionNada EmadNo ratings yet
- Growth and Development of the MandibleDocument45 pagesGrowth and Development of the MandibleSamarth VajpayeeNo ratings yet
- Dr. Munizeh Khan S.R OrthodonticsDocument38 pagesDr. Munizeh Khan S.R OrthodonticsMohsin HabibNo ratings yet
- 21 Biomechanics of Maxillary Expansion and Protraction in Class III Patients Copia 2Document2 pages21 Biomechanics of Maxillary Expansion and Protraction in Class III Patients Copia 2Vicente ContrerasNo ratings yet
- Mandible Development from Prenatal to Postnatal StagesDocument14 pagesMandible Development from Prenatal to Postnatal StagesLiyana G Yaya100% (1)
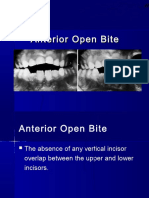
- Dr. Hla Hla Yee Discusses Anterior Open Bite and Deep Bite TreatmentDocument34 pagesDr. Hla Hla Yee Discusses Anterior Open Bite and Deep Bite TreatmentAbdullah100% (1)
- Development of OcclusionDocument50 pagesDevelopment of OcclusionSaid Said100% (1)
- Sunday, March 2, 2008: Important Orthodontic StudiesDocument6 pagesSunday, March 2, 2008: Important Orthodontic StudiesXnb HajiNo ratings yet
- Test 2018 Questions and AnswersDocument23 pagesTest 2018 Questions and AnswersEun SaekNo ratings yet
- Growth and Development Maxilla and MandibleDocument42 pagesGrowth and Development Maxilla and MandibleDrMudit Kumar100% (4)
- Development of DentitionDocument79 pagesDevelopment of Dentitionswathi datrika100% (1)
- Cleft Lip, Cleft Palate and Maxillary Sinus' AkashDocument63 pagesCleft Lip, Cleft Palate and Maxillary Sinus' AkashAkash RautNo ratings yet
- Essential Treatment Planning ConsiderationsDocument28 pagesEssential Treatment Planning ConsiderationsBimalKrishnaNo ratings yet
- Treating Orthodontic Problems in Mixed DentitionDocument109 pagesTreating Orthodontic Problems in Mixed DentitionVishal SharmaNo ratings yet
- Preventive and InterseptiveDocument90 pagesPreventive and InterseptivemuhammadNo ratings yet
- Postnatal Craniofacial Skeleton Growth and DevelopmentDocument62 pagesPostnatal Craniofacial Skeleton Growth and DevelopmentDhanusha ReddyNo ratings yet
- Orthopedo AssDocument4 pagesOrthopedo AssIvyRoselleLacasandileCabañeroNo ratings yet
- Extrinsic and Intrinsic Factors in The Etiology of MalocclusionDocument7 pagesExtrinsic and Intrinsic Factors in The Etiology of MalocclusionNavroop KaurNo ratings yet
- 2dev of MaxillaDocument78 pages2dev of MaxillapriyaNo ratings yet
- 5-Aetiology of MalocclusionDocument7 pages5-Aetiology of MalocclusionKhalid Mortaja100% (1)
- Dent 596 - OrthodonticsDocument6 pagesDent 596 - OrthodonticsAndrei JardanNo ratings yet
- Maxillary Permanent Central IncisorsDocument68 pagesMaxillary Permanent Central IncisorsAmit Singh100% (1)
- Development of Dentition & OcclusionDocument109 pagesDevelopment of Dentition & OcclusionSyed Mohammad Osama Ahsan100% (1)
- Tooth DevelopmentDocument36 pagesTooth DevelopmentDaffa YudhistiraNo ratings yet
- Development of MandibleDocument60 pagesDevelopment of MandibleAlisha Aranha100% (1)
- MandibleDocument120 pagesMandibleArnab SantraNo ratings yet
- Development of The Maxilla: Dr. Samson NegussieDocument38 pagesDevelopment of The Maxilla: Dr. Samson NegussieLintoNo ratings yet
- Diet and Dental CariesDocument76 pagesDiet and Dental CariesPawan RajNo ratings yet
- 1st Course Introductory Course in Paediatric Dentistry&Childhood StagesDocument29 pages1st Course Introductory Course in Paediatric Dentistry&Childhood StagesChristosSougkakisNo ratings yet
- Extractions in Orthodontics PDFDocument2 pagesExtractions in Orthodontics PDFJohnNo ratings yet
- Development of Dentition from Birth to AdulthoodDocument80 pagesDevelopment of Dentition from Birth to Adulthoodvasabaka100% (1)
- Esthetic in Pediatric DentistryDocument13 pagesEsthetic in Pediatric DentistryAtikahNo ratings yet
- Development of Dentition and Occlusion: Sujina.SDocument214 pagesDevelopment of Dentition and Occlusion: Sujina.SsathyaNo ratings yet
- 6 Postgraduate Notes in Orthodontics-250-299Document54 pages6 Postgraduate Notes in Orthodontics-250-299Mu'taz ArmanNo ratings yet
- Lecture (16) Orthodontic Dentistry .: ساملا نانج د Myofunctional Appliance in OrthodonticDocument8 pagesLecture (16) Orthodontic Dentistry .: ساملا نانج د Myofunctional Appliance in Orthodonticاسراء فاضل مصطفىNo ratings yet
- CURRICULUM Orodontie - Anul V Sem X2149096871966833453Document18 pagesCURRICULUM Orodontie - Anul V Sem X2149096871966833453Andrei UsaciNo ratings yet
- GROWTH ASSESSMENT METHODSDocument65 pagesGROWTH ASSESSMENT METHODSdr parveen bathlaNo ratings yet
- MalocclusionDocument95 pagesMalocclusionsonal agarwalNo ratings yet
- Written Examination GuideDocument17 pagesWritten Examination GuideIhsan HanbaliNo ratings yet
- Role of Pediatric Dentist - Orthodontic in Cleft Lip and Cleft Palate PatientsDocument8 pagesRole of Pediatric Dentist - Orthodontic in Cleft Lip and Cleft Palate PatientsIOSRjournalNo ratings yet
- Development of Palate and Tongue NotesDocument9 pagesDevelopment of Palate and Tongue NotesClarisse MendozaNo ratings yet
- Lec 5 P 4Document5 pagesLec 5 P 4brshlwnytwaftkhr956No ratings yet
- Analysis of Diagnostic Records and Space EvaluationDocument78 pagesAnalysis of Diagnostic Records and Space EvaluationAtika Iftikhar MirNo ratings yet
- Development of - PPTX Maxilla NewDocument69 pagesDevelopment of - PPTX Maxilla Newshivadev100% (1)
- OPEN BITE 1 / Orthodontic Courses by Indian Dental AcademyDocument23 pagesOPEN BITE 1 / Orthodontic Courses by Indian Dental Academyindian dental academyNo ratings yet
- Pre Natal and Post Natal MandibleDocument92 pagesPre Natal and Post Natal MandiblenivethaseshaNo ratings yet
- The MandibleDocument115 pagesThe MandiblenavjotsinghjassalNo ratings yet
- Growth of MaxillaDocument149 pagesGrowth of MaxillaDrRanjeet Kumar ChaudharyNo ratings yet
- Clinic ManualDocument12 pagesClinic Manualapi-3139594280% (1)
- Diagnosis of Canine ImpactionDocument27 pagesDiagnosis of Canine ImpactionDr.Thrivikhraman KothandaramanNo ratings yet
- Physiology Stomatognathic SystemDocument19 pagesPhysiology Stomatognathic SystemDan 04No ratings yet
- Zinc Polycorboxylate CementDocument14 pagesZinc Polycorboxylate CementArifa parveenNo ratings yet
- Teeth Development: Bud StageDocument7 pagesTeeth Development: Bud Stageburdall100% (1)
- Growth and Development of Mandible KiranDocument92 pagesGrowth and Development of Mandible Kirannavjotsinghjassal100% (1)
- DR Nick Lekic - Space MaintainersDocument35 pagesDR Nick Lekic - Space MaintainersanatomimanusiaNo ratings yet
- Renal DiseaseDocument18 pagesRenal DiseaseAJPEDO LIFENo ratings yet
- HIV infection in children and oral manifestationsDocument9 pagesHIV infection in children and oral manifestationsAJPEDO LIFENo ratings yet
- Managing Dental Care for Children with Heart DiseaseDocument13 pagesManaging Dental Care for Children with Heart DiseaseAJPEDO LIFENo ratings yet
- Sensory Impairment in Children With Medically Compromised ConditionDocument7 pagesSensory Impairment in Children With Medically Compromised ConditionAJPEDO LIFENo ratings yet
- RespiratorydiseaseDocument13 pagesRespiratorydiseaseAJPEDO LIFENo ratings yet
- Hematological DisorderDocument64 pagesHematological DisorderAJPEDO LIFENo ratings yet
- Role of ProbioticsDocument2 pagesRole of ProbioticsAJPEDO LIFENo ratings yet
- Epilepsy: Neurological DisorderDocument8 pagesEpilepsy: Neurological DisorderAJPEDO LIFENo ratings yet
- BP - DevelopDentition AapdDocument17 pagesBP - DevelopDentition AapdAJPEDO LIFENo ratings yet
- Blood Physiology: Professor A.M.A Abdel GaderDocument45 pagesBlood Physiology: Professor A.M.A Abdel GaderAJPEDO LIFENo ratings yet
- BP - Localanesthesia AapdDocument7 pagesBP - Localanesthesia AapdAJPEDO LIFENo ratings yet
- Guideline On Pediatric Restorative DentistryDocument9 pagesGuideline On Pediatric Restorative DentistryValentina CqNo ratings yet
- Dental Management in Loss of HearingDocument3 pagesDental Management in Loss of HearingAJPEDO LIFENo ratings yet
- Mental DisabilityDocument4 pagesMental DisabilityAJPEDO LIFENo ratings yet
- 5-Plaque and CalculusDocument174 pages5-Plaque and CalculusAJPEDO LIFE100% (1)
- HEMORRHAGIC DISORDERS IN CHILDREN MyDocument146 pagesHEMORRHAGIC DISORDERS IN CHILDREN MyAJPEDO LIFENo ratings yet
- 9-Dental Caries-Epidemiological Studies (International and Indian StudiesDocument133 pages9-Dental Caries-Epidemiological Studies (International and Indian StudiesAJPEDO LIFENo ratings yet
- HEMORRHAGIC DISORDERS IN CHILDREN MyDocument146 pagesHEMORRHAGIC DISORDERS IN CHILDREN MyAJPEDO LIFENo ratings yet
- Survival and Bacteria Reduction of ART RestorationsDocument93 pagesSurvival and Bacteria Reduction of ART RestorationsAJPEDO LIFENo ratings yet
- Hiv in Pediatric DentistryDocument105 pagesHiv in Pediatric DentistryAJPEDO LIFENo ratings yet
- Craniofacial Anomalies Part-IDocument74 pagesCraniofacial Anomalies Part-IAJPEDO LIFENo ratings yet
- Minimal Intervention Restorative DentistryDocument129 pagesMinimal Intervention Restorative DentistryAJPEDO LIFENo ratings yet
- Infant Oral Health CareDocument16 pagesInfant Oral Health CareAJPEDO LIFE100% (1)
- Infant Oral Health CareDocument16 pagesInfant Oral Health CareAJPEDO LIFE100% (1)
- GERIATRIC NUTRITION GUIDEDocument45 pagesGERIATRIC NUTRITION GUIDEveena viswanathan100% (1)
- Why We Need To Protect Polar BearsDocument2 pagesWhy We Need To Protect Polar BearsHân HânNo ratings yet
- Anatomy and Physiology-A ReviewDocument38 pagesAnatomy and Physiology-A Reviewjava_biscocho1229100% (4)
- Aplastic AnemiaDocument5 pagesAplastic AnemiaVenice Marie GargantaNo ratings yet
- Bioh111 So S1 2013Document9 pagesBioh111 So S1 2013monicq77No ratings yet
- Effects of Surface Treatment Modification and Implant Design in Implants Placed Crestal and Subcrestally Applying Delayed Loading ProtocolDocument8 pagesEffects of Surface Treatment Modification and Implant Design in Implants Placed Crestal and Subcrestally Applying Delayed Loading ProtocolluisNo ratings yet
- AP Biology-Tissue Types ChartDocument1 pageAP Biology-Tissue Types ChartJeannie WilliamsNo ratings yet
- Calcitonin Hormone Role and RegulationDocument6 pagesCalcitonin Hormone Role and RegulationSAKARIYE MAXAMEDNo ratings yet
- NOFSA 2010 Guideline For Diagnosis Management OsteoporosisDocument200 pagesNOFSA 2010 Guideline For Diagnosis Management OsteoporosisMadalina Mihaela VasilacheNo ratings yet
- Formative Test DMS 2021-2022Document37 pagesFormative Test DMS 2021-2022Lidwina ChandraNo ratings yet
- Modul Final Biologi Form 4 Fasa 1 2021Document60 pagesModul Final Biologi Form 4 Fasa 1 2021Manmohon Kaur100% (1)
- Alveolar BoneDocument114 pagesAlveolar BoneDent DealsNo ratings yet
- Host ModulationDocument17 pagesHost ModulationIbrar HumayunNo ratings yet
- Understand OsteoporosisDocument9 pagesUnderstand OsteoporosisAudrie Allyson Gabales100% (2)
- Technique To Manage The EnlargedDocument16 pagesTechnique To Manage The EnlargedasepNo ratings yet
- Determining The Age of Fish: BluegillDocument2 pagesDetermining The Age of Fish: BluegillAndrew BenavidesNo ratings yet
- Notes of CH 6 Animal Tissues Class 9th ScienceDocument11 pagesNotes of CH 6 Animal Tissues Class 9th ScienceSingh JNo ratings yet
- Dental Implant Loading ProtocolDocument27 pagesDental Implant Loading ProtocolAli AlmakramiNo ratings yet
- Animal Nutrition: Ch11: Macromineral ElementsDocument33 pagesAnimal Nutrition: Ch11: Macromineral Elements溫.No ratings yet
- IDJSR Special Periodontology IssueDocument75 pagesIDJSR Special Periodontology IssueRoxana DumitracheNo ratings yet
- Pi Is 221081571300036 XDocument6 pagesPi Is 221081571300036 XEko CahyonoNo ratings yet
- Shobha Rawlani, Shivlal Rawlani-Textbook of General Anatomy-JP Medical LTD (Document233 pagesShobha Rawlani, Shivlal Rawlani-Textbook of General Anatomy-JP Medical LTD (Rahul50% (2)
- Growth of The Face and Dental Arches: January 2016Document16 pagesGrowth of The Face and Dental Arches: January 2016Andy HongNo ratings yet
- Progressive Bone LoadingDocument21 pagesProgressive Bone Loadingyogananth100% (1)
- Bone and Joint Disease in Young DogsDocument7 pagesBone and Joint Disease in Young Dogsjcoppala4476No ratings yet
- Recent Advances in Fracture - TMPsDocument309 pagesRecent Advances in Fracture - TMPsTOM TENSUBAMNo ratings yet
- Skeletal System Important Qs Important Questions ICSE 995963bf 28ef 48c2 Ad56 5a8b29c84771Document2 pagesSkeletal System Important Qs Important Questions ICSE 995963bf 28ef 48c2 Ad56 5a8b29c84771sujata duttaNo ratings yet
- OSTEOSARCOMA Final Case PressDocument33 pagesOSTEOSARCOMA Final Case Presssonylynne100% (6)
- Medical Surgical Nursing OrthopedicDocument22 pagesMedical Surgical Nursing Orthopedicroger80% (5)
- Bio OssDocument4 pagesBio OssVizi AdrianNo ratings yet