You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (842)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5807)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Acid-Base Disorder 27 July 2017 PDFDocument48 pagesAcid-Base Disorder 27 July 2017 PDFPauline ChanNo ratings yet
- Ebook PDF Campbell Biology Third 3rd Canadian Edition 2 PDFDocument41 pagesEbook PDF Campbell Biology Third 3rd Canadian Edition 2 PDFmary.martin569100% (33)
- The Endocrine System LabDocument11 pagesThe Endocrine System Lablaike082921100% (1)
- Viticulture ManualDocument66 pagesViticulture Manualpanaglaw100% (2)
- Osmotic PressureDocument2 pagesOsmotic Pressurejana gomezNo ratings yet
- Congestive Heart Failure Case StudyDocument81 pagesCongestive Heart Failure Case Studychibie100% (8)
- Why Study Rizal: Because It Is Mandated by LawDocument28 pagesWhy Study Rizal: Because It Is Mandated by LawChriszanie CruzNo ratings yet
- ArthritisDocument8 pagesArthritisChriszanie CruzNo ratings yet
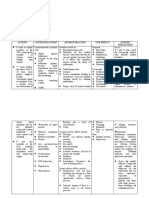
- Nursing Care Plan Cues Nursing Diagnosis Background Knowledge Goal and Objectives Nursing Interventions and Rationale Evaluation Subjective: Goal MetDocument3 pagesNursing Care Plan Cues Nursing Diagnosis Background Knowledge Goal and Objectives Nursing Interventions and Rationale Evaluation Subjective: Goal MetChriszanie CruzNo ratings yet
- Lecture Notes On PerioperativeDocument5 pagesLecture Notes On PerioperativeChriszanie CruzNo ratings yet
- Structural DeformitiesDocument10 pagesStructural DeformitiesChriszanie CruzNo ratings yet
- Human Sexuality NotesDocument1 pageHuman Sexuality NotesChriszanie CruzNo ratings yet
- Perioperative Topic OutlineDocument45 pagesPerioperative Topic OutlineChriszanie CruzNo ratings yet
- Drug StudyDocument5 pagesDrug StudyChriszanie CruzNo ratings yet
- Alterations in Nutrition and GastrointestinalDocument7 pagesAlterations in Nutrition and GastrointestinalChriszanie CruzNo ratings yet
- AnticholinergicsDocument15 pagesAnticholinergicsChriszanie CruzNo ratings yet
- NCP. MOuth SoreDocument1 pageNCP. MOuth SoreChriszanie CruzNo ratings yet
- Myra Levine: The Conservation ModelDocument11 pagesMyra Levine: The Conservation ModelChriszanie CruzNo ratings yet
- Nursing Theory - Joyce TravelbeeDocument11 pagesNursing Theory - Joyce TravelbeeChriszanie CruzNo ratings yet
- Christian MartyrsDocument9 pagesChristian MartyrsChriszanie CruzNo ratings yet
- Anticholinergics 1Document39 pagesAnticholinergics 1Chriszanie CruzNo ratings yet
- Avoiding Common Errors in The Emergency Department-1002-1280Document280 pagesAvoiding Common Errors in The Emergency Department-1002-1280Hernando CastrillónNo ratings yet
- Hidung Dan Sinus ParanasalisDocument16 pagesHidung Dan Sinus ParanasalisChearin Dhea SNo ratings yet
- Estructura Citoarquitectónica de Las Áreas Del Lenguaje: M.C. Etchepareborda, M.J. López-LázaroDocument4 pagesEstructura Citoarquitectónica de Las Áreas Del Lenguaje: M.C. Etchepareborda, M.J. López-LázaroDaniel Gonzalez LaraNo ratings yet
- Gen CHR, Classificatn BryoDocument20 pagesGen CHR, Classificatn BryoadekNo ratings yet
- Drugs For The Treatment of Diabetes MellitusDocument54 pagesDrugs For The Treatment of Diabetes MellitusAndreas AndreouNo ratings yet
- BASICS of ORAL PHYSIOLOGY (Part 1)Document171 pagesBASICS of ORAL PHYSIOLOGY (Part 1)Balarabe EL-HussainNo ratings yet
- (Text) Maternal and Child Health NursingDocument40 pages(Text) Maternal and Child Health NursingVia H.No ratings yet
- 2.2 Biological Molecules Ans PDFDocument18 pages2.2 Biological Molecules Ans PDFtess_15No ratings yet
- Artificial Respiration: ForceDocument15 pagesArtificial Respiration: Forcekushal NeupaneNo ratings yet
- Anatomy and Physiology of The HeartDocument21 pagesAnatomy and Physiology of The HeartNina OaipNo ratings yet
- Biolistrik: DR - Susy OliviaDocument97 pagesBiolistrik: DR - Susy OliviaHartomas BumiharjoNo ratings yet
- Physiology & Behavior: Yoanna M. Ivanova, Hannah Pallubinsky, Rick Kramer, Wouter Van Marken LichtenbeltDocument14 pagesPhysiology & Behavior: Yoanna M. Ivanova, Hannah Pallubinsky, Rick Kramer, Wouter Van Marken LichtenbeltGilberto ZencovNo ratings yet
- Lesson Title: Digestion/Absorption of Nutrients: 7 Grade General Science CourseDocument5 pagesLesson Title: Digestion/Absorption of Nutrients: 7 Grade General Science CourserebbiegNo ratings yet
- Sucrose Gradient Separation ProtocolDocument16 pagesSucrose Gradient Separation ProtocolBalaNo ratings yet
- Serous FluidsDocument14 pagesSerous FluidsSyvelmarie TinteNo ratings yet
- Diagnosing CachexiaDocument8 pagesDiagnosing CachexiainaNo ratings yet
- Femoral Triangle - Borders, Contents and Mnemonics - KenhubDocument7 pagesFemoral Triangle - Borders, Contents and Mnemonics - Kenhubو عجلت اليك ربي لترضيNo ratings yet
- Lesson 6Document4 pagesLesson 6Thea MillanesNo ratings yet
- Blood CollectionDocument6 pagesBlood CollectionSol Kizziah MeiNo ratings yet
- MANISH - KANTI - BISWASUrino-genital System2020-05-04note Kidneyfinal 4-5-20Document11 pagesMANISH - KANTI - BISWASUrino-genital System2020-05-04note Kidneyfinal 4-5-20ShangNo ratings yet
- Neural Charateristics, Types, CommunicationDocument18 pagesNeural Charateristics, Types, CommunicationAdeel AizadNo ratings yet
- Gastric Neuroendocrine TumorsDocument17 pagesGastric Neuroendocrine TumorsNelsonLopezNo ratings yet
- Earth and Life Science SHS 7.1 An Overview of The Nervous SystemDocument38 pagesEarth and Life Science SHS 7.1 An Overview of The Nervous SystemLora Lynne KakilalaNo ratings yet
- Cell Transport - Module-3.09272021Document3 pagesCell Transport - Module-3.09272021Deps CesiNo ratings yet