Professional Documents
Culture Documents
1 s2.0 S2213260019302437 Main
Uploaded by
Rainaldy SanjayaOriginal Title
Copyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
1 s2.0 S2213260019302437 Main
Uploaded by
Rainaldy SanjayaCopyright:
Available Formats
Articles
Bubble continuous positive airway pressure for children with
high-risk conditions and severe pneumonia in Malawi:
an open label, randomised, controlled trial
Eric D McCollum, Tisungane Mvalo, Michelle Eckerle, Andrew G Smith, Davie Kondowe, Don Makonokaya, Dhananjay Vaidya, Veena Billioux,
Alfred Chalira, Norman Lufesi, Innocent Mofolo, Mina Hosseinipour
Summary
Lancet Respir Med 2019; Background Pneumonia is the leading cause of death among children globally. Most pneumonia deaths in low-income
7: 964–74 and middle-income countries (LMICs) occur among children with HIV infection or exposure, severe malnutrition, or
Published Online hypoxaemia despite antibiotics and oxygen. Non-invasive bubble continuous positive airway pressure (bCPAP) is
September 24, 2019
considered a safe ventilation modality that might improve child pneumonia survival. bCPAP outcomes for high-risk
https://doi.org/10.1016/
S2213-2600(19)30243-7 African children with severe pneumonia are unknown. Since most child pneumonia hospitalisations in Africa occur
See Comment page 923
in non-tertiary district hospitals without daily physician oversight, we aimed to examine whether bCPAP improves
Eudowood Division of Pediatric
severe pneumonia mortality in such settings.
Respiratory Sciences,
Department of Pediatrics, Methods This open-label, randomised, controlled trial was done in the general paediatric ward of Salima District
School of Medicine Hospital, Malawi. We enrolled children aged 1–59 months old with WHO-defined severe pneumonia and either HIV
(E D McCollum MD),
Department of International
infection or exposure, severe malnutrition, or an oxygen saturation of less than 90%. Children were randomly
Health, Bloomberg School of assigned 1:1 to low-flow nasal cannula oxygen or nasal bCPAP. Non-physicians administered care; the primary
Public Health (E D McCollum), outcome was hospital survival. Primary analyses were by intention-to-treat and interim and adverse events analyses
and BEAD Core (D Vaidya PhD, per protocol. This trial is registered with ClinicalTrials.gov, number NCT02484183, and is closed.
V Billioux DrPh), Johns Hopkins
University, Baltimore, MD,
USA; University of North Findings We screened 1712 children for eligibility between June 23, 2015, and March 21, 2018. The data safety and
Carolina Project Malawi, monitoring board stopped the trial for futility after 644 of the intended 900 participants were enrolled. 323 children
Lilongwe, Malawi were randomly assigned to oxygen and 321 to bCPAP. 35 (11%) of 323 children who received oxygen died in hospital,
(T Mvalo FCPaed,
D Kondowe BBiomedSc,
as did 53 (17%) of 321 who received bCPAP (relative risk 1·52; 95% CI 1·02–2·27; p=0·036). 13 oxygen and 17 bCPAP
D Makonokaya BScPH, patients lacked hospital outcomes and were considered lost to follow-up. Suspected adverse events related to
I Mofolo MSc, treatment occurred in 11 (3%) of 321 children receiving bCPAP and 1 (<1%) of 323 children receiving oxygen. Four
M Hosseinipour MD);
bCPAP and one oxygen group deaths were classified as probable aspiration episodes, one bCPAP death as probable
Department of Pediatrics,
School of Medicine (T Mvalo) pneumothorax, and six non-death bCPAP events included skin breakdown around the nares.
and Division of Infectious
Disease (M Hosseinipour), Interpretation bCPAP treatment in a paediatric ward without daily physician supervision did not reduce hospital
University of North Carolina at
mortality among high-risk Malawian children with severe pneumonia, compared with oxygen. The use of bCPAP
Chapel Hill, NC, USA; Division
of Emergency Medicine, within certain patient populations and non-intensive care settings might carry risk that was not previously recognised.
Cincinnati Children’s Hospital bCPAP in LMICs needs further evaluation before wider implementation for child pneumonia care.
Medical Center, Cincinnati, OH,
USA (M Eckerle MD);
Funding Bill & Melinda Gates Foundation, International AIDS Society, Health Empowering Humanity.
Department of Pediatrics,
University of Cincinnati College
of Medicine, Cincinnati, OH, Copyright © 2019 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY 4.0 license.
USA (M Eckerle); University of
Utah School of Medicine, Salt
Lake City, UT, USA
Introduction severe malnutrition, or hypoxaemia (peripheral oxygen
(A G Smith MD); and Malawi Pneumonia is the leading infectious cause of death saturation [SpO2] <90%).4–6
Ministry of Heath, Lilongwe, among children aged 1–59 months worldwide.1 In the southern African country of Malawi, hospital
Malawi (A Chalira BSc, According to WHO criteria, pneumonia is a syndrome mortality for children with pneumonia is 3%,7 while
N Lufesi BSc)
characterised by non-specific respiratory signs and mortality of those with pneumonia and severe
Correspondence to:
symptoms, many of which occur in children without malnutrition exceeds 33%.8 Nearly 50% of child
Dr Eric D McCollum, Eudowood
Division of Pediatric Respiratory primary respiratory disease.2 Along with improved pneumonia deaths in Malawi are attributed to HIV.6
Sciences, Johns Hopkins School vaccine access, treatment according to WHO Children with hypoxaemia and pneumonia in Malawi
of Medicine, Baltimore, pneumonia guidelines by healthcare providers in low- are five times more likely to die than non-hypoxaemic
MD 21287, USA
income and middle-income countries (LMICs) over the pneumonia cases,9 and hypoxaemia accounts for 11% of
emccoll3@jhmi.edu
past 20 years has led to reduced child pneumonia paediatric pneumonia admissions.7 Alongside further
mortality globally.3 Now most pneumonia deaths improvement in WHO pneumonia guideline imple
among children aged 1–59 months in LMICs are mentation, new treatments shown to be effective
concentrated in those with HIV infection or exposure, among children with high-risk conditions such as HIV,
964 www.thelancet.com/respiratory Vol 7 November 2019
Articles
Research in context
Evidence before this study Children with more severe illness were excluded; 7% had an
We searched Medline using the following search strategy: oxygen saturation of less than 92%. The authors reported no
((“Continuous Positive Airway Pressure”[MeSH]) AND “ severe adverse events attributable to bCPAP.
((“Pneumonia”[MeSH])“OR “Respiration Disorders”[MeSH]))
Added value of this study
AND ((“Developing Countries”[MeSH]) OR Ghana). The search
Most children with severe pneumonia in low-income and
yielded 19 studies and was completed on Jan 14, 2019. One
middle-income countries are cared for at non-tertiary district
randomised controlled trial (RCT) was published before
hospitals where intensive care is unavailable, physicians are
initiating our study and evaluated the effect of nasal bubble
scarce, and there is little laboratory and radiographic diagnostic
continuous positive airway pressure (bCPAP) on children
support. Most pneumonia deaths in LMICs occur among
1–59 months old with acute respiratory distress in four rural
children with HIV-infection or HIV-exposure, severe acute
hospitals in Ghana. It found that 1 h of bCPAP administered by
malnutrition, or hypoxaemia. We believe that this is the first
nurses, compared with no bCPAP, was safe and reduced mean
trial to date to investigate the effect of nasal bCPAP on hospital
respiratory rate. Two relevant RCTs were published while our
survival among high-risk African children with severe clinical
study was being done. The first examined hospital treatment
pneumonia at a non-tertiary district hospital where physicians
failure prevalences between three groups of children aged
are unavailable and there is no intensive care. This RCT was
1–59 months old with hypoxaemic pneumonia randomly
designed to balance the controls of a clinical trial with the
assigned to nasal bCPAP, high-flow nasal cannula oxygen, or
representativeness of real-world care, and found that the
low-flow nasal cannula oxygen in an intensive care unit of a
administration of bCPAP by nurses and clinicians without daily
research hospital in urban Bangladesh. Nurses administered care
physician oversight elevated the risk of mortality, as compared
under direct physician supervision. After enrolling 225 children,
with low-flow oxygen. Few enrolled children had a nasogastric
the trial was prematurely stopped owing to a lower relative risk
tube inserted despite nearly all being eligible for nasogastric
(RR) of mortality among bCPAP recipients, compared with
tube placement. The influence of infrequent nasogastric tube
low-flow oxygen recipients, on interim analysis (0·25 RR 95% CI
use on these findings is unclear. Compared with oxygen, almost
0·07–0·89). The authors reported no severe adverse events
all subgroups had excess mortality risk from bCPAP.
attributable to bCPAP. The trial excluded children with chronic
illnesses and those meeting predefined treatment failure Implications of all the available evidence
criteria. A crossover design allowed rescue bCPAP or high-flow Our findings show that nasal bCPAP might pose an increased
oxygen for children failing low-flow oxygen, and mechanical risk of mortality, compared with low-flow oxygen, for children
ventilation was available. The second trial was a cluster with severe pneumonia and high-risk conditions who receive
randomised crossover trial in rural Ghana that evaluated 2-week treatment in a non-tertiary LMIC district hospital. These results
mortality after emergency ward care with and without modified differ from the aforementioned trials in Bangladesh and Ghana;
nasal bCPAP among children aged 1–59 months with acute our trial applied wider inclusion criteria in a district hospital
respiratory distress. Care was initiated and administered by setting without physician oversight. These findings raise
nurses under daily physician supervision. Primary analysis found important questions about where and how bCPAP should be
no difference in the RR of mortality between care that included administered, who should administer bCPAP, and which
bCPAP, compared with care without bCPAP (RR 0·67, 95% CI children should receive bCPAP in LMICs. Taken together, nasal
0·42–1·08). A secondary analysis found a two times lower bCPAP should be administered with caution in all care settings
adjusted odds ratio of mortality among children younger than and additional studies are needed to establish which
12 months old receiving bCPAP, compared with those not populations are most likely to benefit from bCPAP when
receiving bCPAP (adjusted odds ratio 0·50, 95% CI 0·28–0·89). intensive care resources are unavailable.
malnutrition, or hypoxaemia will be necessary to mean and increase oxygen delivery among children in shock
ingfully reduce pneumonia mortality globally.3 with circulatory failure.11 A low cost version–bubble CPAP
Non-invasive ventilation with continuous positive (bCPAP)–is used in some high-income settings and is
airway pressure (CPAP) aims to provide constant positive increasingly available in LMICs for neonatal respiratory
airway pressure. This constant positive pressure improves distress, including Malawi.12 Among neonates, bCPAP
lung volumes, ventilation–perfusion mismatch, and the is considered a low-risk treatment with infrequent
work of breathing, thus improving gas exchange.10 By complications that can be safely administered by non-
improving gas exchange, CPAP can reverse or avert physicians.13 bCPAP has also been used for the care of
respiratory failure.10 In many high-income settings, CPAP older infants and children in Malawian tertiary hospitals
is a standard care option for children with respiratory since 2010. Although Malawian data to date have been
failure, including children without hypoxaemia, although observational only, and therefore inconclusive, they
there is variability across settings and evidence is scarce.10 suggest that bCPAP complications among children with
CPAP can also be used to decrease metabolic demand HIV or malnutrition are relatively infrequent and its use
www.thelancet.com/respiratory Vol 7 November 2019 965
Articles
reduces the mean respiratory rate of recipients.14–16 A non-physician clinicians called clinical officers, nurses,
randomised trial from Bangladesh showed bCPAP to be vital sign assistants, and HIV counsellors. Clinical
both safe and efficacious for reducing mortality among officers undergo 3 years of medical education including
children aged 1–59 months with hypoxaemic pneumonia an internship year. To optimise protocol adherence, we
in a physician-supervised intensive care unit.17 However, trained staff on procedures before the study over a 5-day
most paediatric pneumonia hospital admissions in period, including the physiology, application, and
LMICs occur at district hospitals where intensive care is monitoring of bCPAP, did twice-annual refresher
unavailable, pulse oximeters for detecting hypoxaemia courses, and provided on-site paediatrician supervision
are absent, diagnosis by chest radiography is inaccessible, once every 2 weeks. During training and supervisory
and physicians are scarce.18,19 To optimise bCPAP’s child visits, clinical staff were evaluated on their clinical
survival effect in LMICs, bCPAP safety and efficacy must evaluation of patients, use of decision algorithms, and
be evaluated in high-risk pneumonia cases in non-tertiary decision making during directly observed care provision.
district hospitals without daily physician oversight. Remediation took place as necessary. A study paediatrician
We therefore did a randomised controlled trial to based in Malawi was available for telephone consultation
establish whether bCPAP, compared with low-flow at all times. All study nurses had at least 1 year of previous
oxygen, reduces hospital mortality among high-risk bCPAP treatment experience at the referral hospital in
Malawian children with WHO-defined severe pneumonia Lilongwe, Malawi. The nurse study coordinator had
in a general paediatric ward at a non-tertiary district 5 years of bCPAP treatment experience. The trial provided
hospital without daily physician supervision.19 We aimed all respiratory equipment including oxygen concentrators,
to test our hypothesis that bCPAP would decrease bCPAP devices, and pulse oximeters, and also installed
hospital pneumonia mortality among Malawian children an electrical generator, and supplemented medicines.
with high-risk conditions.
Randomisation and masking
Methods This open-label trial used a computer-generated sequence
Study design and participants for simple randomisation; the principal investigator kept
We did an open-label, randomised, superiority trial with the schedule. Random assignment at enrolment was
parallel assignment and a 1:1 allocation ratio as previously established by means of sealed, sequentially numbered
described.20 Eligibility was initially limited to pneumonia opaque envelopes and verified by two study staff.
cases with HIV infection, HIV exposure, or severe
malnutrition. We noted in a parallel observational study at Procedures
the same site that hypoxaemic pneumonia without HIV or Because this study aimed to reflect real world care in
severe malnutrition occurred frequently and also conferred LMIC non-tertiary district hospitals, investigators carefully
high mortality, but limited staffing and equipment deliberated all study procedures to optimise programmatic
resources restricted inclusion of these cases.20 This feasibility and safety. Study procedures have already been
subgroup was incorporated into our study after acquiring described in detail.20 Briefly, children received routine
additional funding. Details of the parallel observational triage and clinical care during consent and were enrolled
study are described elsewhere.20 24 h per day including weekends. After enrolment,
Institutional review boards in Malawi and at all children were immediately placed on the treatment
investigator-affiliated institutions approved the protocol. prescribed by randomisation. All study participants met
Enrolled participants provided written consent. WHO clinical criteria for oxygen use in settings lacking
Eligible children were 1–59 months old with WHO- pulse oximetry. SpO2 was measured in room air by a Rad5
defined severe pneumonia and one or more high-risk pulse oximeter (Masimo, Irvine, CA, USA) for trial
conditions (HIV infection or exposure, severe mal purposes only and participants received bCPAP or low
See Online for appendix nutrition, hypoxaemia; appendix pp 1–3). Severe flow oxygen regardless of SpO2.21 This approach was
pneumonia was defined in two ways, consistent with chosen to reflect typical conditions in non-tertiary district
WHO definitions.21 Specifically, children could meet hospitals where pulse oximeters are not routinely available
eligibility criteria either by having signs of severe and oxygen administration is usually based solely on
pneumonia with or without a general danger sign or by clinical criteria. The protocol did not permit crossover
having signs of pneumonia with a general danger sign. If between groups; children deteriorating on oxygen did not
a child had been enrolled in the study and discharged, and receive rescue bCPAP as bCPAP efficacy had not been
then presented again to the study site, they were ineligible. shown, thus contributing to the equipoise for this trial.
Otherwise, no other exclusion criteria were applied. All participants were assessed for malaria by means of
The trial was done in the general paediatric ward of SD Bioline (HRP2/pLDH) rapid antigen tests (Abbott,
Salima District Hospital in Salima, Malawi, a 250-bed Johannesburg, South Africa) and anaemia by point-of-
government hospital. Intensive care services, mechanical care haemoglobin tests. From May, 2017, children with
ventilation, and portable radiography were unavailable. positive rapid antigen results for malaria also had a
Study staff were available at all times and included smear obtained and processed at the University of North
966 www.thelancet.com/respiratory Vol 7 November 2019
Articles
Carolina Project laboratory, a US Centers for Disease their respiratory danger signs and it was infeasible for
Control and Prevention-certified laboratory, in Lilongwe, staff to frequently titrate the pressure settings and follow
Malawi. Children received antibiotics, intravenous fluids, up to evaluate the clinical response. Previous literature
antimalarials, antipyretics, blood transfusions, and hypo on children reports that CPAP initiation with pressures
glycaemia treatment per WHO and national guidelines.21 between 5 cm and 10 cm H2O is safe.22,23 We used either
Specifically, all children without signs of meningitis were unvented nasal masks or nasal prongs as the nasal
initiated on 50 000 U/kg parenteral benzylpenicillin every interface, with a preference towards nasal masks given
6 h and 7·5 mg/kg parenteral gentamycin daily; those our previous experience of frequent nasal septal trauma
with an abnormal Blantyre Coma Score or stiff neck were and nose bleeds attributed to nasal prong use.14 In the
initiated on 100 mg/kg parenteral ceftriaxone daily. event of a power outage, the nasal mask or prongs were
Children testing positive by rapid antigen testing for immediately removed until the electrical generator was
malaria received 2·4 mg/kg parenteral artesunate daily started.
and antibiotics, were switched to oral artemether– Following initiation, respiratory support for both
lumefantrine after at least 24 h. In addition to first-line groups was weaned in 24 h increments based on step-
antibiotics, HIV-infected or HIV-exposed children wise procedures published previously.20 We established
received oral co-trimoxazole (8 mg/kg trimethoprim) 24 h weaning procedures based on our initial
every 8 h and 2 mg/kg daily oral prednisone for observations that frequent bCPAP pressure titration was
presumptive Pneumocystis jirovecii infection. Consistent not feasible in this setting. Specifically, bCPAP and low-
with WHO guidelines, children with persistent fever or flow oxygen weaning was only permitted for children
worsening respiratory status by day three of hospital who after 24 h of hospitalisation had a decrease in
isation were switched to 80 mg/kg parenteral ceftriaxone respiratory danger signs. Hypoxaemia, grunting or
daily and those with persistent illness despite 5 days of apnoea were considered life threatening and weaning
first-line antibiotics were switched to 80 mg/kg parenteral was not permitted if any of these were present. All
ceftriaxone daily by day 6. Participants with a general children were re-evaluated by clinical staff 60 min after
danger sign, apnoea, grunting, or at least three respiratory any change in bCPAP or low-flow oxygen delivery.
danger signs were fed by nasogastric tube and not Children were escalated back to the previous level of
permitted oral intake. Clinicians and nurses did full respiratory support if new danger signs or hypoxaemia
clinical evaluations of each child at least twice daily. Staff developed after weaning. If not already at maximum
did vital signs and a focused respiratory assessment of low-flow or bCPAP support, children with new danger
children at least every 6 h, including inspecting the nasal signs or hypoxaemia were escalated at all other times
interface for patency. Staff did additional evaluations and
interventions following standard of care for Malawi
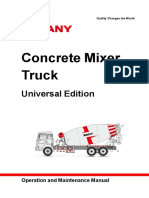
1712 patients assessed for eligibility
district hospitals.
For participants receiving low-flow oxygen, we used the
Airsep Newlife Intensity oxygen concentrator (Chart 1068 excluded
1062 did not meet inclusion criteria
Industries, New York, USA) to deliver oxygen through a 5 declined to participate
flow splitter. The oxygen group initially received 1 other
0·5 L/min if aged 30–59 days and 2 L/min if aged
2–59 months through nasal prongs. Initial settings
644 randomly assigned
followed WHO and national guidelines.21
For participants receiving bCPAP, we used a validated
bCPAP system (Fisher and Paykel Healthcare, Auckland,
New Zealand), which provides warmed humidification 323 allocated to low flow oxygen 321 allocated to bCPAP group
group 145 severe hypoxaemia
and pressure control. As in all bCPAP systems, pressure 142 severe hypoxaemia subgroup
was maintained via the depth of expiratory tubing in the subgroup 15 HIV-infected subgroup
system’s water reservoir, and airflow was titrated to 21 HIV-infected subgroup 49 HIV-exposed subgroup
50 HIV-exposed subgroup 112 severe acute malnutrition
achieve bubbling in the reservoir. Airflow was delivered 110 severe acute malnutrition subgroup
via an Airsep Newlife Intensity oxygen concentrator at subgroup
6–8 L/min. Participants were initiated on 7 cm H2O
nasal bCPAP for children aged 30–59 days and 8 cm H2O 13 lost to follow-up 17 lost to follow-up
nasal bCPAP for children aged 2–59 months. Although 4 referral 2 referral
the bCPAP pressure ranges between 5 cm H2O and 8 cm 9 withdrawal 15 withdrawal
H2O were determined before the trial, the use of 7 cm
H2O and 8 cm H2O as the initial pressure setting was 310 per-protocol analysis 304 per-protocol analysis
established between June and August, 2015, when it was
observed that nine of the first ten enrolled bCPAP Figure 1: Trial profile
recipients required such pressures to stabilise or improve bCPAP=bubble continuous positive airway pressure.
www.thelancet.com/respiratory Vol 7 November 2019 967
Articles
during the trial. For both groups, low-flow oxygen was
Low-flow oxygen bCPAP
(n=323) (n=321) the final step in weaning and was only stopped when all
respiratory danger signs were resolved.
Demographic and anthropomorphic characteristics
The nasal interface was examined for patency and fit
Age, months 7·7 (3·4–15·1) 7·6 (3·0–15·6)
and nasal suctioning by means of a catheter and normal
Sex
saline was done on deteriorating patients or patients
Female 149 (46%) 150 (47%)
with any bCPAP or oxygen change. Chest radiography
Male 174 (54%) 171 (53%)
was done on children with persistent or worsening
Weight, kg 7·3 (2·9) 7·0 (2·7)
illness if transportation to the radiography department
MUAC 12·7 (1·9) 12·7 (1·8)
could be safely completed, as is typical in LMIC district
High risk condition hospitals. Between patient uses, respiratory equipment
HIV infected 21 (7%) 15 (5%) was decontaminated and reused per Malawi guidelines
HIV exposed 50 (15%) 49 (15%) (see appendix p 81), consistent with programmatic
Severe acute malnutrition without HIV infection or exposure 110 (34%) 112 (35%) conditions.
SpO2 <90% without HIV infection, HIV exposure, or severe acute 142 (44%) 145 (45%)
malnutrition
Outcomes
Findings at presentation
The trial’s predefined primary outcome was survival to
Axillary temperature, °C* 37·5 (1·0) 37·4 (1·1)
hospital discharge. Predefined secondary outcomes
Axillary temperature ≥38·0°C* 91/322 (28%) 81/320 (25%)
included antibiotic and hospital treatment failure, 30-day
Pulse rate, beats per min 165 (24) 165 (24)
post-discharge vital status, and hospital adverse events.
Systolic blood pressure, mm Hg† 106 (15) 101 (17) Among those alive on day 14 of hospitalisation, hospital
Respiratory rate, breaths per min 62 (15) 62 (15) treatment failure is defined as the presence of any one of
SpO₂ 88% (84–95) 87% (81·5–94) the following: temperature ≥38°C, any respiratory danger
SpO₂ 93–100% 105 (33%) 86 (27%) sign, or continued oxygen or bCPAP requirement. Events
SpO₂ 90–92% 22 (7%) 16 (5%) were graded per DAIDS AE Grading Table version 1.0 by
SpO₂ <90% 196 (61%) 219 (68%) the investigators and were verified by the data and safety
Any respiratory danger sign 319 (99%) 319 (99%) monitoring board (DSMB). Outcomes were stratified by
Severe lower chest wall indrawing 284 (88%) 291 (91%) prespecified patient characteristics including SpO2, age,
Head nodding or tracheal tugging 84 (26%) 92 (29%) sex, anaemia, wheeze, mental status, diarrhoea, and
Grunting 78 (24%) 76 (24%) malaria.
Very fast breathing for age‡ 107 (33%) 104 (32%)
Stridor while calm 5 (2%) 8 (2%) Statistical methods
Apnoea 16 (5%) 21 (7%) With a sample size of 900 participants, the trial had
Nasal flaring 242 (75%) 229 (71%) 80% power to detect a 6·0 percentage point lower
Any general danger sign 55 (17%) 65 (20%) mortality prevalence with bCPAP, assuming 14·7%
Convulsions 26 (8%) 35 (11%) mortality with standard care at a two-sided α level of
Inability to feed 36 (11%) 42 (13%) 0·05. Sample size calculations and assumptions were
Vomiting everything 8 (2%) 11 (3%) described in detail previously.20 Per-protocol interim
Blantyre Coma Score ≤4 20 (6%) 35 (11%) DMSB analyses were done at 30% and 60% enrolment.
Crackle without wheeze 151 (47%) 160 (50%) O’Brien-Fleming stopping thresholds of 0·0006 were
Wheeze with or without crackle 68 (21%) 60 (19%) prespecified for the first interim analyses and 0·0151 for
Severe anaemia*§ 29 (9%) 36 (11%) the second interim analyses.
Diarrhoea 14 (4%) 10 (3%) The DSMB recommended futility analysis at the second
Dehydration 17 (5%) 16 (5%) interim point. In this context futility was calculated as a
Laboratory assessments
0·0026% probability that bCPAP might achieve a
Haemoglobin, g/dL* 9·6 (2·5) 9·4 (2·7)
significantly lower mortality risk, compared with oxygen,
Malaria rapid antigen positive 89 (28%) 108 (34%)
if enrolment continued to the target sample size.
We assessed unadjusted treatment effects on primary
Data are median (IQR), n (%), and mean (SD). bCPAP=bubble continuous positive airway pressure. MUAC=mid-upper and secondary outcomes in the main and subgroup
arm circumference. SpO₂=peripheral arterial oxyhaemoglobin saturation. *322 and 320 participants in the low-flow
oxygen group and bCPAP group had an axillary temperature measured and 320 in the bCPAP group had a
analyses by means of Stata’s epitab package and log
haemoglobin sample collected. †98 and 96 participants in the low-flow oxygen group and bCPAP group had a binomial regression to estimate relative risks (RRs). We
systolic blood pressure collected. ‡Very fast breathing for age defined as ≥80 breaths per min for children aged tested subgroup by treatment interaction (heterogeneity
30–59 days, ≥70 breaths per min for children aged 2–11 months, and ≥60 breaths per min for children aged of treatment effect) by means of Poisson regression
12–59 months. §Severe anaemia was a haemoglobin <6 g/dL in children without severe acute malnutrition and
<4 g/dL in children with severe acute malnutrition. because some models did not converge. Final analyses
were intention-to-treat. We summarised continuous data
Table 1: Baseline characteristics with means and SDs and compared differences by
Student’s t tests or non-parametric rank sum tests based
968 www.thelancet.com/respiratory Vol 7 November 2019
Articles
on data distribution. Categorical data was reported by
Low-flow bCPAP Relative 95% CI p value
means of the number and proportion within each oxygen (n=321) risk
category and comparisons by Pearson χ² tests. We also (n=323)
did ad-hoc exploratory analyses that included time to Alive 275 (85%) 251 (78%) 0·92 0·85–0·99 0·023
hospital death by study group, fidelity implementation Dead 35 (11%) 53 (17%) 1·52 1·02–2·27 0·036
outcomes per group allocation, baseline characteristics
and fidelity implementation outcomes by hospital Data are n (%), unless otherwise stated. bCPAP=bubble continuous positive airway
pressure.
outcome, and association between study year and
hospital outcome by treatment group. We used non- Table 2: Hospital outcomes
parametric log-rank tests for the survival analysis, and
Cox regression analyses to estimate the treatment hazard
ratio (HR) and its 95% CI. This study is registered with com pared with the oxygen group (1·65 RR, 95% CI
ClinicalTrials.gov, number NCT02484183. 1·00–2·75; p=0·048). The results from the 229 non-
hypoxaemic children (SpO2 90–100%) were not significant
Role of the funding source and did not suggest a benefit from bCPAP, compared
The sponsors had no role in the design, implementation, with oxygen (RR 1·32, 95% CI 0·69–2·55; p=0·39). The
analyses, interpretation, write up, or decision to publish. RR of hospital death among 144 hypoxaemic bCPAP
The corresponding author had access to all data and recipients with no other high-risk condition was 2·67
takes responsibility for the manuscript. (95% CI 1·16–6·16; p=0·021), compared with the
142 hypoxaemic oxygen recipients with no other high-risk
Results condition. Analyses of other hypoxaemic subgroups did
We screened children for eligibility between June 23, 2015, not reach significance (appendix pp 10–11).
and March 21, 2018; children with severe hypoxaemia who Although prespecified analysis by malaria status was
were without HIV or severe malnutrition were included inconclusive it did not suggest children with malaria
after May, 2016. 644 children had a co-existing high-risk benefited from bCPAP, compared with oxygen
condition and were randomly assigned with 323 allocated (appendix pp 10–11). The RR of death from bCPAP,
to low-flow oxygen and 321 to bCPAP (figure 1; table 1). compared with oxygen, among all 197 children that
17 bCPAP and 13 oxygen patients lacked hospital outcomes tested rapid malaria positive was 1·26 (95% CI
and were considered lost to follow-up. Specifically, four 0·70–2·27; p=0·44). Among 447 children with a
low-flow oxygen children and two bCPAP children were negative rapid malaria test, the RR of death from
referred to a tertiary hospital and nine low-flow oxygen bCPAP versus oxygen was 1·64 (95% CI 0·96–2·81;
children and 15 bCPAP children withdrew from the trial. p=0·067). To understand whether a positive rapid
88 (14%) children died while hospitalised; 35 (11%) antigen test represented a true case of malaria, over the
deaths occurred among the oxygen group and 53 (17%) final 12 months of the trial, malaria smears were
among the bCPAP group (table 2). Children randomly collected on all patients testing rapid malaria positive
assigned to bCPAP, compared with oxygen, had a higher and analysed at an internationally certified laboratory.
relative risk of hospital death (RR 1·52, 95% CI 21 (24%) of 89 children in the oxygen group who tested
1·02–2·27; p=0·036). rapid malaria positive had a malaria smear, and only
In analysis of prespecified secondary outcomes, three (14%) of 21 were smear positive. Among
suspected adverse events related to bCPAP or oxygen 108 bCPAP children with positive rapid malaria tests,
occurred in 11 (3%) of 321 children receiving bCPAP and 24 (22%) of 108 had a malaria smear collected and only
1 (<1%) of 323 children receiving oxygen (appendix four (17%) of 24 were smear positive. One oxygen
pp 4–9). Four bCPAP and one oxygen group death were patient who was smear positive and no bCPAP patients
classified as probable aspiration episodes, one bCPAP who were smear positive died in the hospital.
death as probable pneumothorax, and six non-death Although almost all other prespecified high-risk sub
bCPAP events included skin breakdown around the group analyses showed excess mortality for bCPAP,
nares. The RR of 2-week hospital treatment failure in the compared with oxygen, none were statistically significant.
bCPAP group, compared with the oxygen group, was We also compared the RR for children who did and did
1·32 (95% CI 0·96–1·83); p=0·081; appendix p 13). not have a condition of interest to examine whether any
Among children discharged from the hospital, the subgroup had a differential treatment effect from bCPAP
prespecified RR 30-day post discharge mortality in the (heterogeneity of treatment effect), and we found no
bCPAP group, compared with the oxygen group was 1·42 significant difference for any subgroup (presence vs
(95% CI 0·24–8·39; p=0·70; appendix p 16). absence of condition, appendix pp 10–11). All other
We also examined hospital mortality prevalences secondary endpoints are in the appendix pp 12–15.
among children with and without hypoxaemia and An exploratory survival analysis did not suggest delayed
malaria (appendix pp 10–11). Among all 415 hypoxaemic hospital mortality among either group (figure 2).
children, the bCPAP group had a higher RR of death Children randomly assigned to bCPAP had a 1·55 HR
www.thelancet.com/respiratory Vol 7 November 2019 969
Articles
0·30 bCPAP
Oxygen
Hazard ratio 1·55 (95% CI 1·01–2·37; p=0·041)
0·25
Cumulative probability of hospital death
0·20
0·15
0·10
0·05
0
0 1 10 20 30 40
Days in hospital after random assignment
Day 1 Day 2 Day 3 Day 4 Day 5 Days 6–10 Days 11–37
Oxygen bCPAP Oxygen bCPAP Oxygen bCPAP Oxygen bCPAP Oxygen bCPAP Oxygen bCPAP Oxygen bCPAP
Number at risk 323 321 312 307 301 289 295 277 290 272 261 244 22 21
Died 10 10 10 17 5 11 5 5 2 3 3 7 0 0
Figure 2: Kaplan-Meier mortality curves
Time to hospital death was an exploratory analysis. Day 37 was the latest day that a child had a hospital outcome in the oxygen group.
We report additional implementation outcomes that
Low-flow oxygen bCPAP p value
(n=323) (n=321) measured fidelity of the treatment to care protocols in
table 3 and also exploratory analyses in the appendix
Nasogastric tube feeding
pp 16–18. Of note, although 619 (96%) of 644 children
Eligible for nasogastric tube 311 (96%) 308 (96%) 0·84
enrolled onto the trial met nasogastric tube insertion
Nasogastric tube inserted 61 (20%) 40 (13%) 0·024
criteria, records indicated that only 101 (16%) of
Antibiotic switch
619 participants received one. A 7% lower proportion of
Alive and eligible for antibiotic switch at hospital 225/283 (80%) 184/266 (69%) 0·0056
day 6*
bCPAP children (40 (13%) of 308), compared with oxygen
children (61 (20%) of 311), were documented to have had
Antibiotic switched 225/225 (100%) 184/184 (100%) 1·0
a tube inserted (p=0·024). To assess whether respiratory
Respiratory support
equipment might have deteriorated over the course of
Length of respiratory support in days† 3·9 (2·1) 4·5 (1·9) 0·0007
the study we evaluated whether there was any interaction
Fluid support for diarrhoea-associated dehydration
between study year and the odds of hospital mortality by
Dehydrated 17 (5%) 16 (5%) 0·87
trial group, and we observed no significant interaction
Fluid resuscitated‡ 17 (100%) 16 (100%) 1·0
(p=0·20).
Time of death
Died at night§ 25/35 (71%) 24/53 (45%) 0·018
Discussion
Data are n (%) or mean (SD). bCPAP=bubble continuous positive airway pressure. *40 oxygen and 55 bCPAP children Using a randomised trial design implemented in a non-
died or were lost-to-follow up by day six of hospitalisation. †Among 275 oxygen and 251 bCPAP children that survived tertiary district hospital without physicians, we assessed
to hospital discharge. ‡Six oxygen children and six bCPAP children were classified as severe dehydration and all six
the effect of bCPAP compared with low-flow nasal cannula
oxygen children and six bCPAP children were documented as receiving at least one 10 cm³/kg intravenous fluid bolus.
§Defined as between 1700 h and 0759 h. oxygen for African children with severe pneumonia and at
least one high-risk condition. Compared with oxygen, we
Table 3: Implementation outcomes
found that bCPAP not only provided no benefit but, more
alarmingly, its use was associated with an increased risk of
for hospital death (95% CI 1·01–2·37; p=0·041) compared mortality among this patient population. These results
with patients in the oxygen group. Most excess bCPAP should be interpreted with caution given the possible
hospital mortality (13 (72%) of 18) occurred on days two overestimation of treatment effect on mortality that might
and three post-random assignment. occur when trials are stopped prematurely.24
970 www.thelancet.com/respiratory Vol 7 November 2019
Articles
Since the study was stopped prematurely by the DSMB, In our study, we attempted to balance internal and
the predefined subgroups were individually under external validity by maintaining the controls of a clinical
powered to detect a mortality risk. Although severely trial while observing implementation in a real-world
malnourished children overall had high hospital setting. This unique design optimises the public health
mortality (20%), the RR of mortality among bCPAP effect of trials and has been classified by others as a type
recipients, compared with oxygen recipients, was 1·07 1 hybrid implementation effectiveness design in which
(95% CI, 0·64–1·79; p=0·79; appendix p 7). This RR was the health outcome is the primary endpoint but imple
modest compared with other prespecified subgroups. On mentation is also monitored.26 We carefully considered
the basis of these findings there does not seem to be external validity in our preparations, and several
much additional risk in the use of bCPAP, compared purposeful design decisions might have affected the trial
with oxygen, among severely malnourished children in results.
this trial. However, almost all subgroups had point First, we focused on severely ill children representative
estimates suggesting excess bCPAP mortality. Taken of most hospital severe pneumonia deaths in LMICs and
together, these results do not support bCPAP treatment limited the exclusion criteria to only patients previously
of these high-risk children in similar LMIC settings enrolled in the study. Under real-world conditions and in
without further evidence. Our findings instead suggest the absence of mechanical ventilation (typical of
that bCPAP might not be safe for high-risk children at conditions in LMICs), many providers would use bCPAP
LMIC non-tertiary district hospitals. It is also unclear if for all children with respiratory danger signs. We also
bCPAP has a detrimental effect on mortality risk among acknowledge that providers using CPAP in other settings
similar high-risk cohorts in settings where physician might not treat similar patients with CPAP based on
supervision is available. Further controlled studies are their own care practices.
needed. Second, we did our trial in an environment that
Previous bCPAP trials either restricted high-risk reflected real-world personnel conditions where non-
children’s inclusion to an intensive care unit under physician providers delivered all patient care without
daily physician supervision or enrolled less-sick daily physician supervision. Our approach was ethically
children.17,25 Interpretation of the results of previous sound on the basis of CPAP’s strong safety record for
trials and our results must be taken in this context. A neonates under the care of non-physicians, including in
randomised trial of 146 hypoxaemic Bangladeshi Malawi, and the fact that physicians rarely provide daily
children aged 1–59 months in an intensive care unit of care in non-tertiary LMIC hospitals.13,14
one research hospital found a 0·25 RR of hospital Third, our study used 6–8 L/min of unblended oxygen
mortality from nasal bCPAP, compared with low-flow to deliver bCPAP pressure. The resources required to
oxygen.17 However, this trial relied on physician- titrate air–oxygen delivery to achieve the flow required for
supervised intensive care, escalated children failing bCPAP are expensive and beyond what most LMIC
treatment to mechanical ventilation, and excluded district hospitals can sustainably provide. Commercial
children with treatment failure at enrolment, an oxygen concentrators, on the other hand, are commonly
important subgroup that, in our experience, would available in LMIC district hospitals, are recommended by
usually be prioritised for bCPAP in real-world settings WHO,27 and generate enough flow to drive bCPAP.
where mechanical ventilation is unavailable. A cluster However, commercial oxygen concentrators generate
randomised trial in Ghana compared modified bCPAP flow with an FiO2 greater than 90%, do not blend oxygen
with routine care among 2181 children aged 1–59 months with medical air unless altered post manufacturing, and
with respiratory distress receiving care from nurses are incom patible with air–oxygen blenders owing to
under daily physician supervision at two district inadequate pressure.27 In order to achieve adequate
hospitals.25 No difference in mortality was seen in the pressures, bCPAP children were exposed to higher flows
primary unadjusted analysis, although secondary of inspired FiO2 than low-flow-oxygen children. Although
adjusted analyses reported a 0·40 RR of mortality difficult to accurately estimate, we acknowledge that
among children younger than 12 months receiving bCPAP children were possibly exposed to FiO2 greater
bCPAP, compared with routine care. In contrast, in our than 60%, which has the theoretical toxicity of reactive
trial children younger than 12 months old had an oxygen species, such as pulmonary inflammation and
elevated RR of mortality compared with children aged adsorption atelectasis, as well as to a longer duration of
12 months and older (RR 1·70, 95% CI 1·00–2·90; respiratory support than oxygen group children.28
appendix p 10). However, the Ghana trial excluded Interestingly, the Bangladesh trial, which showed
severely ill children for whom bCPAP would probably improved survival from bCPAP, also used a commercial
be used in real-world settings and although nurses led oxygen concentrator with FiO2 greater than 90% to drive
care provision, physicians were available for daily flow, and their patients might have been exposed to
supervision of care. Further, the trial’s modified bCPAP similar amounts of oxygen.17 Since the Bangladesh trial
was different to standard bCPAP in that a conventional used standard oxygen nasal prongs to deliver bCPAP,
CPAP machine was used as the flow-driver. rather than commercial CPAP prongs or masks, more
www.thelancet.com/respiratory Vol 7 November 2019 971
Articles
entrainment of room air might have occurred to reduce distension and vomiting, it is also possible that the
FiO2 below possible percentages delivered in our trial. combination of higher initiating CPAP pressures,
However, if the nasal interface was not tightly sealed, enteral feeding, and low proportion of nasogastric tube
then the positive end expiratory pressure is also likely to use among bCPAP recipients predisposed patients to
have been lower. Although improbable, we cannot unrecognised aspiration events. Our findings might not
exclude oxygen toxicity as a possible factor in bCPAP be applicable to settings that have more widely adopted
deaths. the use of nasogastric tubes.
Fourth, we used a validated bCPAP device whose com Pneumothoraces might also have contributed to
ponents are deemed single use by the manufacturer. bCPAP deaths. Although paediatric data are scarce,
Because of budgetary constraints and supply chain issues neonatal bCPAP studies report pneumothoraces as
in Malawi and other LMICs, respiratory supplies are in infrequent, ranging between 0% and 7%.33 Our initiation
our experience almost always disinfected and reused bCPAP pressures (7–8 cm H2O) were unlikely to have
during routine care, and we took this approach.29 Single posed exceptional risk.22,23 We also monitored delivered
use supplies are usually unsustainable during pro pressures by gauge manometry at least twice daily to
grammatic conditions. Since most bCPAP mortality ensure pressures did not persistently exceed these
occurred within 3 days and the odds of bCPAP mortality, amounts. In the event of low pressures, staff evaluated
relative to oxygen mortality, did not change by study year, the fit of the nasal interface and observed for mouth leak.
equipment contamination was unlikely to be a mortality No interventions such as chin straps or other modalities
driver in this trial. were used to mitigate mouth leak in this trial. Owing to
There are other possible explanations for our findings. the unavailability of portable radiography, we relied on
Infants and children with respiratory danger signs clinical examinations to detect pneumothoraces in
might be at an increased risk of swallowing impairment patients considered unsafe for transportation to the
and aspiration.30 Evidence regarding whether nasal radiology department, which was most patients. This
CPAP increases aspiration risk is scarce.31,32 Nevertheless, approach was deliberated extensively before the trial and
to reduce aspiration risk, high-resource setting CPAP it was ascertained to be ethical—given bCPAP’s strong
recipients are often fed continuously through safety record among neonates—and commensurate with
nasogastric or post-pyloric tubing, a practice rare in real-world bCPAP care since most district hospitals do
LMICs. Before this trial, Malawian children with not have portable radiography or 24-h access to
respiratory danger signs were fed orally; only comatose radiologists for urgent interpretations. We identified only
children were bolus fed through nasogastric tubing. one probable pneumothorax among bCPAP recipients
Additionally, in our clinical experience in Malawi, errors and none among oxygen recipients, suggesting that
related to the volume or type of intravenous fluid either pneumothoraces were missed or that they were
administered are common and can have serious health not a key explanation for bCPAP mortality.
consequences. Given these safety concerns and that Unlike other trials that used CPAP nasal prongs
enteral feeds is standard of care in most settings for exclusively,17,25 this trial used unvented nasal masks or
children on CPAP, we opted to administer maintenance CPAP nasal prongs for the nasal interface of bCPAP
hydration and enteral feeds to children using nasogastric children. Although study staff inspected the nasal
tubes when respiratory distress was substantial. interface for any obstruction as a part of their routine
Although study staff were trained to use nasogastric evaluations and in any deteriorating patients, it is
tubes, the proportion of eligible children with a tube possible that unrecognised mispositioning of the mask
placed was low and bCPAP recipients, compared with or obstruction of the nasal prongs might have led to the
oxygen recipients, were even less likely to have a tube development of hypoxaemic or hypercapneic respiratory
inserted. An analysis of outcomes for patients with or failure in some children. We observed that a higher
without a nasogastic tube is given in the appendix (p 18). proportion of oxygen children died at night, compared
Unfortunately, our routine supervisory visits did not with bCPAP children, and we speculate that this might
appreciate the degree to which nasogastric tubes were reflect respiratory vulnerability during sleep that is
not used by providers or refused by parents. Notably, insufficiently addressed by low-flow oxygen.
these data are unable to establish whether tube insertion Several additional limitations require discussion.
was low because of inaccurate documentation, parental Although the trial design intentionally sought to replicate
refusal, or health-care provider reluctance (possibly real-world settings as much as possible, we did augment
owing to difficulty inserting the tube when the CPAP clinical staffing, supplement local equipment, and
nasal interface was in place), nor is it clear whether the provide fortnightly in-person paediatrician supervision.
tube was used once inserted. Although speculative, This was done to ensure the degree of internal validity
these trial data might suggest that more unrecognised expected of rigorous efficacy trials. The augmented
aspiration-related events occurred and could have clinical support might imply that similar LMIC district
differentially contributed to bCPAP mortality. Although hospitals could not implement bCPAP without sub
we did not observe frequent issues with gastric stantial investment, or that only select, better-resourced
972 www.thelancet.com/respiratory Vol 7 November 2019
Articles
hospitals would have the capacity for bCPAP in existing definitely address what patient populations might benefit
programmatic conditions. from bCPAP including context-appropriate contra
Next, WHO severe pneumonia is a clinical diagnosis that indications for its use in settings without care escalation
does not require chest radiographs or clinical auscultation options such as invasive mechanical ventilation.
to confirm the presence of lower respiratory disease. The In conclusion, while important questions remain, this
signs and symptoms of WHO severe pneumonia are non- trial challenges the notion that bCPAP is without risk and
specific and can be found in children without primary is ready for widespread implementation for LMIC child
respiratory disease, including those with circulatory pneumonia care where most patients at high-risk receive
failure.2 To pragmatically assess the effect of bCPAP as it care, namely, the general paediatric wards of non-tertiary
would be administered in real-world conditions, this trial district hospitals where physicians are absent. This trial
purposefully included children diagnosed with WHO also challenges the conventional wisdom that effective
severe pneumonia. Given that WHO severe pneumonia is care in one setting always translates to another and
a non-specific diagnosis, some of the trial’s patients highlights the tangible risks of implementing more
probably had signs and symptoms driven primarily by complex care in resource-constrained settings. Taken
non-respiratory disease such as shock from malaria or together with previous bCPAP trial results and limitations,
sepsis. Respiratory support, including CPAP, is these findings generate uncertainty around bCPAP use
recommended for such children with significant and demand further research of bCPAP before wider
circulatory failure as preload is being optimised or implementation in similar LMIC settings.
inotropic support initiated.11 Cardiopulmonary interactions Contributors
must be considered whenever applying bCPAP to patients. EDM acquired the funding. EDM, TM, ME, AGS, MH were
By increasing intrathoracic pressure, CPAP can decrease responsible for conceptualisation and design. EDM curated the data.
DK and DM collected the data. DV, VB, and EDM were responsible for
cardiac preload which can adversely affect some patients in data analysis. EDM, TM, ME, AGS, and MH were responsible for data
shock. In high-resource settings, CPAP is widely used for interpretation. EDM wrote the original draft.. EDM, TM, ME, AGS,
patients in shock in intensive care settings with direct DK, DM, DV, VB, AC, NL, IM, and MH were responsible for writing,
physician oversight and careful evaluation of preload and review, and editing.
cardiac output. As previously discussed, WHO-defined Declaration of interests
severe pneumonia is a non-specific diagnosis that can We declare no competing interests.
include patients in shock. In this trial, we followed WHO Data sharing
guidelines for the treatment and evaluation of patients De-identified individual participant data and a data dictionary will be
made available with publication with a signed data access agreement
with signs of shock. However, given the resources of a with the authors.
district hospital, monitoring of such patients was less than
Acknowledgments
would be done in a typical intensive care or high We offer our sincere thanks to the children and their caregivers
dependency unit. Therefore, we cannot exclude cardio participating in this trial, Salima District Hospital and the Malawi
pulmonary interactions from bCPAP as a contributor to Ministry of Health for their commitment and support, and the CPAP
IMPACT study team for their critical contributions to this study.
our results. Our study was intentionally not designed, and
owing to premature study termination inadequately References
1 Liu L, Oza S, Hogan D, et al. Global, regional, and national causes
powered, to differentiate bCPAP efficacy between patients of under-5 mortality in 2000–15: an updated systematic analysis
with respiratory or circulatory failure, or both, and our with implications for the Sustainable Development Goals. Lancet
results should be interpreted within this context. 2017; 388: 3027–35.
2 Scott JAG, Wonodi C, Moïsi JC, et al. The definition of pneumonia,
Finally, we did not expect to find higher bCPAP the assessment of severity, and clinical standardization in the
mortality. As a result, the trial was not designed and did Pneumonia Etiology Research for Child Health Study.
not have the resources to explicitly evaluate whether Clin Infect Dis 2012; 54: S109–16.
3 McCollum ED, King C, Hammitt LL, et al. Reduction of childhood
aspiration, oxygen toxicity, equipment contamination, or pneumonia mortality in the Sustainable Development era.
pneumothoraces were definitive reasons for increased Lancet Respir Med 2016; 4: 932–33.
bCPAP mortality. Future studies should address all of 4 Sonego M, Pellegrin MC, Becker G, Lazzerini M. Risk factors for
these issues. Of note, since commercially available mortality from acute lower respiratory infections (ALRI) in children
under five years of age in low and middle-income countries:
oxygen concentrators do not titrate FiO2, additional a systematic review and meta-analysis of observational studies.
oxygen delivery innovations that permit titration and PLoS One 2015; 10: e0116380.
high flow rates while remaining feasible and affordable 5 Lazzerini M, Sonego M, Pellegrin MC. Hypoxaemia as a mortality
risk factor in acute lower respiratory infections in children in low
for LMICs will be needed. Further, although radiographic and middle-income countries: systematic review and meta-analysis.
imaging is not widely available, future research should PLoS One 2015; 10: e0136166.
include routine imaging to better assess the incidence of 6 Theodoratou E, McAllister DA, Reed C, et al. Global, regional, and
national estimates of pneumonia burden in HIV-infected children
pneumothoraces among similar patients and to evaluate in 2010: a meta-analysis and modelling study. Lancet Infect Dis 2014;
associations between pneumothoraces and positive end 14: 1250–58.
expiratory pressures. In addition, the inclusion of 7 McCollum ED, Nambiar B, Deula R, et al. Impact of the 13-valent
pneumococcal conjugate vaccine on clinical and hypoxemic
autopsies should be considered to more reliably attribute childhood pneumonia over three years in central Malawi:
cause of death. Lastly, future studies should seek to more an observational study. PLoS One 2017; 12: e0168209.
www.thelancet.com/respiratory Vol 7 November 2019 973
Articles
8 Lazzerini M, Seward N, Lufesi N, et al. Mortality and its risk factors 21 Guidelines for the management of common childhood illnesses,
in Malawian children admitted to hospital with clinical pneumonia, 2nd edn. Geneva, Switzerland: World Health Organization, 2013.
2001–12: a retrospective observational study. Lancet Glob Health http://apps.who.int/iris/bitstream/10665/81170/1/9789241548373_
2016; 4: e57–68. eng.pdf (accessed July 8, 2019).
9 Hooli S, Colbourn T, Lufesi N, et al. Predicting Hospitalised 22 Calderini E, Chidini G, Pelosi P. What are the current indications
Paediatric Pneumonia Mortality Risk: An External Validation of for noninvasive ventilation in children? Curr Opin Anaesthesiol 2010;
RISC and mRISC, and Local Tool Development (RISC-Malawi) 23: 368–74.
from Malawi. PLoS One 2016; 11: e0168126. 23 Essouri S, Chevret L, Durand P, Haas V, Fauroux B, Devictor D.
10 Morley SL. Non-invasive ventilation in paediatric critical care. Noninvasive positive pressure ventilation: five years of experience in
Paediatr Respir Rev 2016; 20: 24–31. a pediatric intensive care unit. Pediatr Crit Care Med 2006;
11 Davis AL, Carcillo JA, Aneja RK, et al. American College of Critical 7: 329–34.
Care Medicine clinical practice parameters for hemodynamic 24 Viele K, McGlothlin A, Broglio K. Interpretation of clinical trials
support of pediatric and neonatal septic shock. Crit Care Med 2017; that stopped early. JAMA 2016; 315: 1646–47.
45: 1061–93. 25 Wilson PT, Baiden F, Brooks JC, et al. Continuous positive airway
12 Jensen EA, Chaudhary A, Bhutta ZA, Kirpalani H. Non-invasive pressure for children with undifferentiated respiratory distress in
respiratory support for infants in low- and middle-income Ghana: an open-label, cluster, crossover trial. Lancet Glob Health
countries. Semin Fetal Neonatal Med 2016; 21: 181–88. 2017; 5: e615–23.
13 Martin S, Duke T, Davis P. Efficacy and safety of bubble CPAP in 26 Curran GM, Bauer M, Mittman B, Pyne JM, Stetler C.
neonatal care in low and middle income countries: a systematic Effectiveness-implementation hybrid designs: combining elements
review. Arch Dis Child Fetal Neonatal Ed 2014; 99: F495–504. of clinical effectiveness and implementation research to enhance
14 Walk J, Dinga P, Banda C, et al. Non-invasive ventilation with public health impact. Med Care 2012; 50: 217–26.
bubble CPAP is feasible and improves respiratory physiology in 27 Technical specifications for oxygen concentrators. Geneva: World
hospitalised Malawian children with acute respiratory failure. Health Organization, 2015. http://apps.who.int/iris/bitstream/
Paediatr Int Child Health 2016; 36: 28–33. handle/10665/199326/9789241509886_eng.pdf?sequence=1
15 Myers S, Dinga P, Anderson M, et al. Use of bubble continuous (accessed July 8, 2019).
positive airway pressure (bCPAP) in the management of critically ill 28 Hafner S, Beloncle F, Koch A, Radermacher P, Asfar P. Hyperoxia
children in a Malawian paediatric unit: an observational study. in intensive care, emergency, and peri-operative medicine: Dr. Jekyll
BMJ Open Respir Res 2019; 6: e000280. or Mr. Hyde? A 2015 update. Ann Intensive Care 2015; 5: 42.
16 McCollum ED, Smith A, Golitko CL. Bubble continuous positive 29 Helping babies breathe provider guide, 2nd edn. Washington, DC:
airway pressure in a human immunodeficiency virus-infected American Academy of Pediatrics, 2016. https://wwwaaporg/en-us/
infant. Int J Tuberc Lung Dis 2011; 15: 562–64. advocacy-and-policy/aap-health-initiatives/helping-babies-survive/
17 Chisti MJ, Salam MA, Smith JH, et al. Bubble continuous positive Pages/Helping-Babies-Breathe-Editionaspx (accessed July 8, 2019).
airway pressure for children with severe pneumonia and 30 Dodrill P, Gosa MM. Pediatric dysphagia: physiology, assessment,
hypoxaemia in Bangladesh: an open, randomised controlled trial. and management. Ann Nutr Metab 2015; 66 (suppl 5): 24–31.
Lancet 2015; 386: 1057–65. 31 Hori R, Isaka M, Oonishi K, Yabe T, Oku Y. Coordination between
18 Graham SM, English M, Hazir T, Enarson P, Duke T. Challenges to respiration and swallowing during non-invasive positive pressure
improving case management of childhood pneumonia at health ventilation. Respirology 2016; 21: 1062–67.
facilities in resource-limited settings. Bull World Health Organ 2008; 32 Hanin M, Nuthakki S, Malkar MB, Jadcherla SR. Safety and efficacy
86: 349–55. of oral feeding in infants with BPD on nasal CPAP. Dysphagia 2015;
19 McCollum ED, Smith AG, Eckerle M, Mvalo T, O’Brien KL, 30: 121–27.
Baqui AH. CPAP treatment for children with pneumonia in 33 Thukral A, Sankar MJ, Chandrasekaran A, Agarwal R, Paul VK.
low-resource settings. Lancet Respir Med 2017; 5: 924–25. Efficacy and safety of CPAP in low- and middle-income countries.
20 Smith AG, Eckerle M, Mvalo T, et al. CPAP IMPACT: a protocol for J Perinatol 2016; 36 (suppl 1): S21–8.
a randomized trial of bubble continuous positive airway pressure
versus standard care for high-risk children with severe pneumonia
using adaptive design methods. BMJ Open Respir Res 2017;
4: e000195.
974 www.thelancet.com/respiratory Vol 7 November 2019
You might also like
- Food Protein Induced Enterocolitis (FPIES): Diagnosis and ManagementFrom EverandFood Protein Induced Enterocolitis (FPIES): Diagnosis and ManagementTerri Faye Brown-WhitehornNo ratings yet
- Vaccines: Does herd immunity justify permanent impairment for a few?From EverandVaccines: Does herd immunity justify permanent impairment for a few?No ratings yet
- Community Acquired Pneumonia, A Case StudyDocument26 pagesCommunity Acquired Pneumonia, A Case StudyMenggay SanDiego57% (7)
- Community-Acquired Pneumonia in Children: Myths and FactsDocument4 pagesCommunity-Acquired Pneumonia in Children: Myths and FactsFranciscoDelgadoNo ratings yet
- Jurnal 1Document8 pagesJurnal 1aziskarnNo ratings yet
- Evaluation and Management of Febrile Children 2016Document7 pagesEvaluation and Management of Febrile Children 2016Luisa Frj100% (1)
- Articles: BackgroundDocument9 pagesArticles: BackgroundklaukakoNo ratings yet
- Inf 40 s07Document11 pagesInf 40 s07187011090No ratings yet
- Revisión Sistematica - TuberculosisDocument9 pagesRevisión Sistematica - TuberculosisKaren Reichell MedinaNo ratings yet
- Macrolides in Children With Community-Acquired Pneumonia: Panacea or Placebo?Document7 pagesMacrolides in Children With Community-Acquired Pneumonia: Panacea or Placebo?Agniya Ali FahmiNo ratings yet
- Neumonia Complicada PDFDocument9 pagesNeumonia Complicada PDFadriana gallardoNo ratings yet
- Debenedictis 2020Document13 pagesDebenedictis 2020Lina María CañónNo ratings yet
- Ventilator-Associated PneumoniDocument15 pagesVentilator-Associated PneumoniYasminNo ratings yet
- Neumonia Por InfluenzaDocument19 pagesNeumonia Por InfluenzaEdgar GavilanesNo ratings yet
- 1 s2.0 S0929664621003892 MainDocument8 pages1 s2.0 S0929664621003892 Mainrheynamaulidar rumoninNo ratings yet
- Cep 2020 00339Document23 pagesCep 2020 00339Elison J PanggaloNo ratings yet
- 01 ProjectDocument30 pages01 Projectkarunyabathula100% (1)
- 12701-50629-1-PB-1 AnakDocument4 pages12701-50629-1-PB-1 AnakAni RoseNo ratings yet
- International Journal of Pediatric Research Ijpr 5 052Document11 pagesInternational Journal of Pediatric Research Ijpr 5 052ahmad asadullahNo ratings yet
- Rajiv Gandhi University of Health Sciences, Bangalore, Karnataka Synopsis Proforma For Registration of Subjects For DissertationDocument14 pagesRajiv Gandhi University of Health Sciences, Bangalore, Karnataka Synopsis Proforma For Registration of Subjects For Dissertationpavin0% (1)
- MacGinty Et Al-2018-Pediatric PulmonologyDocument14 pagesMacGinty Et Al-2018-Pediatric Pulmonologywawa chenNo ratings yet
- Pediatrics 2015 Irwin 635 42Document10 pagesPediatrics 2015 Irwin 635 42Arif Pasti BisaNo ratings yet
- HHS Public Access: Prevention and Control of Childhood Pneumonia and DiarrheaDocument16 pagesHHS Public Access: Prevention and Control of Childhood Pneumonia and DiarrheagemzeddNo ratings yet
- 13-10 Topic 7. Complicated PneumoniaDocument35 pages13-10 Topic 7. Complicated PneumoniaReza Ervanda ZilmiNo ratings yet
- Wurzel 2016Document8 pagesWurzel 2016prolanis pkmmulyoharjoNo ratings yet
- CAP Guidelines SA 2020Document22 pagesCAP Guidelines SA 2020kudzaimuregidubeNo ratings yet
- Fuchs 2018Document14 pagesFuchs 2018Miguel Angel CayojaNo ratings yet
- 1 s2.0 S1896112615000498 MainDocument6 pages1 s2.0 S1896112615000498 MainNELSON VIDIGALNo ratings yet
- Art 2Document14 pagesArt 2linda margaritaNo ratings yet
- Review: Jacquie N Oliwa, Jamlick M Karumbi, Ben J Marais, Shabir A Madhi, Stephen M GrahamDocument9 pagesReview: Jacquie N Oliwa, Jamlick M Karumbi, Ben J Marais, Shabir A Madhi, Stephen M GrahamirenaNo ratings yet
- Key Clinical Research Priorities For The Pediatric Community During The COVID-19 PandemicDocument3 pagesKey Clinical Research Priorities For The Pediatric Community During The COVID-19 PandemicnpidasNo ratings yet
- Perez Velez 2012Document14 pagesPerez Velez 2012Abby OliivasNo ratings yet
- Pattern of Infectious Morbidity in Hiv-Exposed Uninfected Infants and ChildrenDocument8 pagesPattern of Infectious Morbidity in Hiv-Exposed Uninfected Infants and Childrenmiss betawiNo ratings yet
- Pneumonias in Children Practical Policies For StudentsDocument45 pagesPneumonias in Children Practical Policies For StudentsIbtissame BadadNo ratings yet
- TB in ChildrenDocument7 pagesTB in ChildrenPororo KewrenNo ratings yet
- Lowerrespiratory Tractinfections: Anne B. Chang,, Christina C. Chang,, K. O'Grady,, P.J. TorzilloDocument19 pagesLowerrespiratory Tractinfections: Anne B. Chang,, Christina C. Chang,, K. O'Grady,, P.J. Torzilloshrey keyalNo ratings yet
- TB in ChildrenDocument9 pagesTB in Childrenparamita nindyaNo ratings yet
- Trend and Outcome of Sepsis in ChildrenDocument8 pagesTrend and Outcome of Sepsis in ChildrenGunduz AgaNo ratings yet
- Risk Factors For Mortality in Children With HAP in Dr. Sutomo SurabayaDocument7 pagesRisk Factors For Mortality in Children With HAP in Dr. Sutomo SurabayaadhitiaNo ratings yet
- High Prevalence of Pneumocystis Jirovecii Pneumonia Among Mozambican Children 5 Years of Age Admitted To Hospital With Clinical Severe PneumoniaDocument7 pagesHigh Prevalence of Pneumocystis Jirovecii Pneumonia Among Mozambican Children 5 Years of Age Admitted To Hospital With Clinical Severe PneumoniaAnonymous qpHeArUNo ratings yet
- Candidiasis NeonatalDocument9 pagesCandidiasis Neonatalgeorgi15685No ratings yet
- Neumococo Minesota 2014Document10 pagesNeumococo Minesota 2014Milyta1092No ratings yet
- Child Health and TBDocument3 pagesChild Health and TBsoukumar8305No ratings yet
- COVID 19 en UCIP Paises de Recursos Limitados. DR Carcillo. Pediatric Research 2020 Muy BuenaDocument12 pagesCOVID 19 en UCIP Paises de Recursos Limitados. DR Carcillo. Pediatric Research 2020 Muy BuenaDark LouNo ratings yet
- Factors Associated With Complicated Pneumonia in ChildrenDocument19 pagesFactors Associated With Complicated Pneumonia in ChildrenJHONATAN MATA ARANDANo ratings yet
- International Journal of Infectious Diseases: Ben J. MaraisDocument4 pagesInternational Journal of Infectious Diseases: Ben J. MaraisMiftahurrahmah GmsNo ratings yet
- Impact of Malaria at The End of Pregnancy On Infant Mortality and MorbidityDocument9 pagesImpact of Malaria at The End of Pregnancy On Infant Mortality and MorbidityDebby Astasya AnnisaNo ratings yet
- Articulo MicroDocument8 pagesArticulo Microliliana ospinaNo ratings yet
- PediatricsDocument21 pagesPediatricsLuis ArrietaNo ratings yet
- Local Studies and LiteratureDocument9 pagesLocal Studies and LiteratureKarl GutierrezNo ratings yet
- Acceptance of A COVID 19 Vaccine and Associated Factors Among Pregnant Women in China A Multi Center Cross Sectional Study Based On Health BeliefDocument12 pagesAcceptance of A COVID 19 Vaccine and Associated Factors Among Pregnant Women in China A Multi Center Cross Sectional Study Based On Health BeliefamalliaNo ratings yet
- Sepsis Management of Neonates With Suspected or Proven Early-Onset BacterialDocument12 pagesSepsis Management of Neonates With Suspected or Proven Early-Onset BacterialAldo CancellaraNo ratings yet
- Special Issue ARTICLE Less Is More: Evidence-Based Management of BronchiolitisDocument11 pagesSpecial Issue ARTICLE Less Is More: Evidence-Based Management of BronchiolitisyundaNo ratings yet
- In ChildrenDocument7 pagesIn ChildrenJames LopezNo ratings yet
- Immunization Systems Across The GlobeDocument92 pagesImmunization Systems Across The GlobeJosefa CapuyanNo ratings yet
- Vijay 2018Document6 pagesVijay 2018Rabiatul 'raney' AdawiyahNo ratings yet
- Jurnal 2Document11 pagesJurnal 2KikiNurAqidahNo ratings yet
- Summary of Vax-Unvax by Robert F. Kennedy Jr.: Let the Science Speak (Children’s Health Defense)From EverandSummary of Vax-Unvax by Robert F. Kennedy Jr.: Let the Science Speak (Children’s Health Defense)No ratings yet
- Covid-19 Infection and PregnancyFrom EverandCovid-19 Infection and PregnancyAhmed M. Maged El-GolyNo ratings yet
- Mounting: Operating InstructionsDocument6 pagesMounting: Operating InstructionsstankevichijusNo ratings yet
- Guide Isolators 2017Document180 pagesGuide Isolators 2017GhiloufiNo ratings yet
- UGNEWRevisedFinalII IVVI TimeTableAug, Sept03.08.2021Document10 pagesUGNEWRevisedFinalII IVVI TimeTableAug, Sept03.08.2021siva pkbkNo ratings yet
- Traffic Engineering Third Edition by Roess & Prasas 2004 PDFDocument802 pagesTraffic Engineering Third Edition by Roess & Prasas 2004 PDFdanielNo ratings yet
- Combined Cycle Power Plant - Summary StudyDocument3 pagesCombined Cycle Power Plant - Summary StudydndudcNo ratings yet
- Naples Capital Improvement Plan 2022-2026Document215 pagesNaples Capital Improvement Plan 2022-2026Omar Rodriguez OrtizNo ratings yet
- HSE TerminologyDocument6 pagesHSE TerminologyZeshanNo ratings yet
- Chapter 1 Revised Edition HeheheDocument75 pagesChapter 1 Revised Edition HeheheWendell MagdaluyoNo ratings yet
- FORM 5 VariationDocument35 pagesFORM 5 VariationAMOS YAP WEI KANG MoeNo ratings yet
- Concrete Mixer Truck Universal EditionDocument118 pagesConcrete Mixer Truck Universal EditionRendy fahleviNo ratings yet
- Chapter 3 - Transducer and Sensors Part 1Document46 pagesChapter 3 - Transducer and Sensors Part 1Zersh EthioNo ratings yet
- MahindraDocument44 pagesMahindraWuling PalembangNo ratings yet
- Soler Han Weston JSE May 2014Document16 pagesSoler Han Weston JSE May 2014missile1124No ratings yet
- MOV S ManualDocument84 pagesMOV S ManualAbdulrahmanNo ratings yet
- Chapter 3Document96 pagesChapter 3Sinclyr Valenciano100% (2)
- TDS - Pidicryl 120V - UpdatedDocument1 pageTDS - Pidicryl 120V - Updatedhai nguyenNo ratings yet
- Ekeke Chijioke Bright CVDocument4 pagesEkeke Chijioke Bright CVchijioke ekekeNo ratings yet
- Examen de Corigenţă La Limba Engleză Clasa A VIIDocument6 pagesExamen de Corigenţă La Limba Engleză Clasa A VIIAnonymous HdI5CTRNo ratings yet
- Non Destructive TestingDocument9 pagesNon Destructive TestingAhmed KhanNo ratings yet
- 1741 - Long Span Structures ReportDocument5 pages1741 - Long Span Structures ReportHuzefa SayyedNo ratings yet
- Black 1950 PDFDocument10 pagesBlack 1950 PDFcis freteNo ratings yet
- Lab ReportDocument17 pagesLab ReportHabtamu BaynekawNo ratings yet
- Worksheet 8: Language HandbookDocument2 pagesWorksheet 8: Language HandbookMrs BeyNo ratings yet
- Spring 2019 PDFDocument56 pagesSpring 2019 PDFMayyage LokayaNo ratings yet
- Sheet 2 of 2: Turn TurnDocument2 pagesSheet 2 of 2: Turn TurnJesùs AlfaroNo ratings yet
- Farm and Home Visits Are An Essential Part ofDocument16 pagesFarm and Home Visits Are An Essential Part ofChariss VerdidaNo ratings yet
- PR No.03&04 (DT+GD)Document8 pagesPR No.03&04 (DT+GD)Viska FirmanNo ratings yet
- Et3491 Esiot LabDocument95 pagesEt3491 Esiot LabfreefireyomaNo ratings yet
- 005 - Romulan Warbird (D'Deridex)Document20 pages005 - Romulan Warbird (D'Deridex)Fabien Weissgerber100% (1)