You might also like
- Journey Management Log Sheet: Jazan - Abha Refined Products Pipeline ProjectDocument1 pageJourney Management Log Sheet: Jazan - Abha Refined Products Pipeline ProjectFarrukh IjazNo ratings yet
- RSAW Basic Trip Plan HardDocument1 pageRSAW Basic Trip Plan Hardrichard nagassarNo ratings yet
- JourneyPlanReport 67Document1 pageJourneyPlanReport 67moh.a.elhamid0No ratings yet
- DAGS Travel Order September 2023-Pick-Up I-BEAMSDocument8 pagesDAGS Travel Order September 2023-Pick-Up I-BEAMSFrancis Danver EmerzNo ratings yet
- Cube 180Document1 pageCube 180Gregorio AndradeNo ratings yet
- Journey Management Plan: (For Light Vehicles / Pickups Only) (Tick If Yes)Document2 pagesJourney Management Plan: (For Light Vehicles / Pickups Only) (Tick If Yes)KevinGandjarAdiwidjajaNo ratings yet
- Monthly Vehicle Use RPT - Fuel Card Trans LogDocument8 pagesMonthly Vehicle Use RPT - Fuel Card Trans LogPakistan Tourism OfficialNo ratings yet
- Form2-01-01Process FMEA WorksheetDocument1 pageForm2-01-01Process FMEA WorksheetMuhammad Reza GadranNo ratings yet
- 015 03 AmbulanceDocument1 page015 03 AmbulanceHassan YoussofNo ratings yet
- GreensboroRural BikeroutesDocument1 pageGreensboroRural BikeroutesrvralphNo ratings yet
- Travel Mileage RecordDocument1 pageTravel Mileage RecordRakesh RauniyarNo ratings yet
- ServiceSchedule MD22Document3 pagesServiceSchedule MD22theo_swaranNo ratings yet
- Equipment Maintenance Log Template 12Document1 pageEquipment Maintenance Log Template 12mohammed nayeemNo ratings yet
- C-004-RW-Dozer12 - Rev.1https://www - Scribd.com/upload-Document?archive - Doc 342076489&escape False&metadata ("Context":"archive","page":"read","action":false,"logged - In":true,"platform":"web")Document3 pagesC-004-RW-Dozer12 - Rev.1https://www - Scribd.com/upload-Document?archive - Doc 342076489&escape False&metadata ("Context":"archive","page":"read","action":false,"logged - In":true,"platform":"web")slamet4riadiNo ratings yet
- (Sheet No.-1) : Unit - : M/s. Dalmia Bharat Sugar and Industries LTDDocument2 pages(Sheet No.-1) : Unit - : M/s. Dalmia Bharat Sugar and Industries LTDAderson ScottNo ratings yet
- National Institute of Technology-Andhra Pradesh: Travelling Allowance BillDocument2 pagesNational Institute of Technology-Andhra Pradesh: Travelling Allowance BillBabuRaoThellaNo ratings yet
- BPAC-FR-OHSE-028 Commissioning MAN HAULDocument3 pagesBPAC-FR-OHSE-028 Commissioning MAN HAULFahmi Noviandri100% (1)
- Baja Saeindia 2022 DVP&R + Dfmea TemplateDocument10 pagesBaja Saeindia 2022 DVP&R + Dfmea TemplateNandam HarshithNo ratings yet
- Baja Saeindia 2022 DVP&R + Dfmea TemplateDocument10 pagesBaja Saeindia 2022 DVP&R + Dfmea TemplateTinu MawaleNo ratings yet
- Standard Trip OverviewDocument1 pageStandard Trip OverviewAndreas ManurungNo ratings yet
- 13 Q Driveability Questionaire PDFDocument1 page13 Q Driveability Questionaire PDFisshmangNo ratings yet
- Standard Trip OverviewDocument1 pageStandard Trip OverviewAndreas ManurungNo ratings yet
- Journey Management - Risk-Rated Trip Plan FormDocument1 pageJourney Management - Risk-Rated Trip Plan FormArdiansyahm AncaNo ratings yet
- Barangay Nutrition Action PlanDocument1 pageBarangay Nutrition Action PlanFebNo ratings yet
- LTA Claim FormDocument1 pageLTA Claim Formharmeet kaurNo ratings yet
- Labor Influx - KS-05-Excel FileDocument6 pagesLabor Influx - KS-05-Excel FileNatarajan SaravananNo ratings yet
- Icfai University, Dehradun: Student Name Iud No Ibs NoDocument7 pagesIcfai University, Dehradun: Student Name Iud No Ibs Norohit5586No ratings yet
- Form2!01!01Process FMEA Worksheet (RCL SMALL)Document1 pageForm2!01!01Process FMEA Worksheet (RCL SMALL)Muhammad Reza GadranNo ratings yet
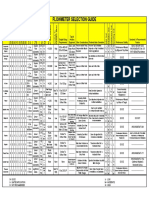
- Flow Meter Selection GuideDocument1 pageFlow Meter Selection GuidePavendhan PavNo ratings yet
- Rao Mooe 2022Document71 pagesRao Mooe 2022brgy.sanmatias2024No ratings yet
- Auto Maintenance LogDocument1 pageAuto Maintenance Logzakarya yahyaNo ratings yet
- Round 2 Allotment List (Broad Sheet) - Uttarakhand - 101-200Document100 pagesRound 2 Allotment List (Broad Sheet) - Uttarakhand - 101-200Ashok PaskalrajNo ratings yet
- Mini Bus C 001 RW 12 Rev.1Document2 pagesMini Bus C 001 RW 12 Rev.1slamet4riadi100% (1)
- DAGS Travel Order For October 2022Document2 pagesDAGS Travel Order For October 2022Francis Danver EmerzNo ratings yet
- HIRA For Stores ActivityDocument5 pagesHIRA For Stores ActivityRohit Singh100% (22)
- Local Exp. (Yrs) Driving Skills / Special Skills / Other RemarkDocument3 pagesLocal Exp. (Yrs) Driving Skills / Special Skills / Other RemarkBibhu PrasadNo ratings yet
- Jsa For Mechanical Activity: H/M/L H/M/LDocument1 pageJsa For Mechanical Activity: H/M/L H/M/Ljithin shankarNo ratings yet
- UgandaDocument1 pageUgandaAlexander Krivov100% (18)
- Autoinspekt Rating: 2018 EICHER PRO 1049 2750Document6 pagesAutoinspekt Rating: 2018 EICHER PRO 1049 2750Pavan Singh RajputNo ratings yet
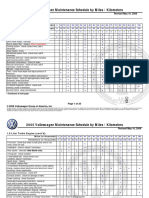
- VW Maintenance Card 2005 Revised May 16 2008 PDFDocument23 pagesVW Maintenance Card 2005 Revised May 16 2008 PDFOndřej PolákNo ratings yet
- Govt. General Hospital, Kurnool Recruitment of Child Psychologist On Contract Basis - 2020 For 01 Post - FINAL MERIT LIST (19.10.2020)Document2 pagesGovt. General Hospital, Kurnool Recruitment of Child Psychologist On Contract Basis - 2020 For 01 Post - FINAL MERIT LIST (19.10.2020)vamsi karnaNo ratings yet
- TA-DA-Form-for-Provincial EmployeesDocument2 pagesTA-DA-Form-for-Provincial EmployeesMuhammad FahimNo ratings yet
- Job Order DriverDocument2 pagesJob Order DriverMae Francesca Isabel GarciaNo ratings yet
- Commissioning Test Pack Template - Normal Condition-Latest 2Document107 pagesCommissioning Test Pack Template - Normal Condition-Latest 2Tomi NofiantoNo ratings yet
- Work Program - 230 PpeDocument6 pagesWork Program - 230 PpeHarris DarpingNo ratings yet
- Bush Pressing MCDocument1 pageBush Pressing MCShreekant GurlakattiNo ratings yet
- Operator'S Manual: 21" Rotary Mower - Model Series 410 Thru 420Document16 pagesOperator'S Manual: 21" Rotary Mower - Model Series 410 Thru 420GorneauNo ratings yet
- Taqdeer Center EstimateDocument2 pagesTaqdeer Center EstimateSourav Raha100% (1)
- UN Contractor Crew Competency Review Form G - 2011Document5 pagesUN Contractor Crew Competency Review Form G - 2011AKOGU J. AKPOCHI J.No ratings yet
- Barsha Pump Brochure MK5Document2 pagesBarsha Pump Brochure MK5Andrés PerezNo ratings yet
- WMO VDR.15.AHT - Fiona 38Document1 pageWMO VDR.15.AHT - Fiona 38Kokok LASNo ratings yet
- Formulir Premob Inspection LVDocument2 pagesFormulir Premob Inspection LVElni Gita GirsangNo ratings yet
- Individual Performance Commitment and Review Form: Basic Education Service Teaching Learning Process (30%)Document3 pagesIndividual Performance Commitment and Review Form: Basic Education Service Teaching Learning Process (30%)Donita-jane Bangilan CanceranNo ratings yet
- Japl-F-Wi-008-Journey Management Log Sheet 1Document1 pageJapl-F-Wi-008-Journey Management Log Sheet 1Ali HassanNo ratings yet
- Total Customer Care: 100% Predictable CostsDocument2 pagesTotal Customer Care: 100% Predictable CostsAgustin BerriosNo ratings yet
- I Application IDocument1 pageI Application ISaravanan SaravananNo ratings yet
- Troika PDFDocument2 pagesTroika PDFgattolwkNo ratings yet
- AIRSCALEDocument1 pageAIRSCALEhassaniNo ratings yet
- Add To FavoritesDocument1 pageAdd To FavoriteshassaniNo ratings yet
- z3 RA23100EN04GLA2 RTC LabelDocument3 pagesz3 RA23100EN04GLA2 RTC LabelhassaniNo ratings yet
- Proguard ProjectDocument1 pageProguard ProjecthenryqueNo ratings yet
- 4G NokiaDocument1 page4G NokiahassaniNo ratings yet
- Nokia Airscale SolutionDocument1 pageNokia Airscale SolutionhassaniNo ratings yet
- Warsaw Lab SBTS-40 Parameters - v2Document1 pageWarsaw Lab SBTS-40 Parameters - v2hassaniNo ratings yet
- SRAN16.1 SBTS CommissioningDocument14 pagesSRAN16.1 SBTS Commissioninghassani50% (2)
- Transmission Network OverviewDocument30 pagesTransmission Network OverviewhassaniNo ratings yet
- DocumentDocument12 pagesDocumentDanut Caraboi67% (3)
- 1348063812microwave Link DesignDocument68 pages1348063812microwave Link Designalfred calaunanNo ratings yet
- 1348063812microwave Link DesignDocument68 pages1348063812microwave Link Designalfred calaunanNo ratings yet
- HUAWEI GSM BTS3900A Hardware Structure-20080730-B-ISSUE4 (1) .0Document84 pagesHUAWEI GSM BTS3900A Hardware Structure-20080730-B-ISSUE4 (1) .0Sonny KurniawanNo ratings yet
- RTN 980 V100R007C10 Product Description 02Document257 pagesRTN 980 V100R007C10 Product Description 02Hugo Mauricio Sánchez CNo ratings yet
- Handover in WCDMADocument81 pagesHandover in WCDMAhassaniNo ratings yet
- Map Info Professional Install GuideDocument66 pagesMap Info Professional Install GuidehassaniNo ratings yet
- Huawei DBS3900 Commissioning MOP - V1 - 2 20090515Document30 pagesHuawei DBS3900 Commissioning MOP - V1 - 2 20090515yetunde77100% (5)
- Biologi, Jilid 1 - John W. Kimball Alih Bahasa Oleh H. Siti Soetarmi Tjitrosomo, Nawangsari SugiriDocument1 pageBiologi, Jilid 1 - John W. Kimball Alih Bahasa Oleh H. Siti Soetarmi Tjitrosomo, Nawangsari SugiriSyauka NiarNo ratings yet
- MOP of Troubleshooting-V1Document2 pagesMOP of Troubleshooting-V1hassaniNo ratings yet
- Map Basic ReferenceDocument893 pagesMap Basic ReferencehassaniNo ratings yet
- Huawei DBS3900 Commissioning MOP - V1 - 2 20090515Document30 pagesHuawei DBS3900 Commissioning MOP - V1 - 2 20090515yetunde77100% (5)
- HUAWEI DBS3900 Dual-Mode Base Station Hardware Structure and Pinciple-20090223-IsSUE1.0-BDocument79 pagesHUAWEI DBS3900 Dual-Mode Base Station Hardware Structure and Pinciple-20090223-IsSUE1.0-BUdo Elisha UcheNo ratings yet
- RV Magazine 202105Document84 pagesRV Magazine 202105jumper_bonesNo ratings yet
- Vehicle Standards Bulletin 01Document37 pagesVehicle Standards Bulletin 01LizardladNo ratings yet
- Airstream Europe Catalog 2009Document11 pagesAirstream Europe Catalog 2009PierreNo ratings yet
- AAA Membership Benefits GuideDocument32 pagesAAA Membership Benefits GuideEddie ZelayaNo ratings yet
- PD 856 Sanitation Code of PhilippinesDocument28 pagesPD 856 Sanitation Code of PhilippinesJason Angel Buñag100% (2)
- Abandoned Vehicle Procedure 8-12-11Document2 pagesAbandoned Vehicle Procedure 8-12-11Michael BenhamouNo ratings yet
- Ford Protect Service PlanDocument6 pagesFord Protect Service PlanRoy HyperblueNo ratings yet
- Caravan Owners Hbook 2006 PDFDocument186 pagesCaravan Owners Hbook 2006 PDFjose antonio Mellado100% (1)
- Mercial TruePDF-January 2017Document92 pagesMercial TruePDF-January 2017Ciprian CociubaNo ratings yet
- Captain CaravanDocument15 pagesCaptain Caravanoguz akakce100% (1)
- Beginner's GuideDocument39 pagesBeginner's GuideMad-Max-1No ratings yet
- My Home Is My CastleDocument5 pagesMy Home Is My CastleVerdeș EcaterinaNo ratings yet
- Caravan - magazine.truePDF December.2018Document102 pagesCaravan - magazine.truePDF December.2018MadaMadutsaNo ratings yet
- Hymer 60 Jahre Sondermodelle 002 enDocument11 pagesHymer 60 Jahre Sondermodelle 002 enPedroNo ratings yet
- Homesteading For 3,000Document38 pagesHomesteading For 3,000WICKED MERCY86% (7)
- Caravanning Australia v14#1Document196 pagesCaravanning Australia v14#1Executive MediaNo ratings yet
- 4ES0 01 Que 20170608Document36 pages4ES0 01 Que 20170608Ustadh Sadique100% (1)
- As 4177.3-2004 Caravan and Light Trailer Towing Components Coupling Body For Ball CouplingsDocument7 pagesAs 4177.3-2004 Caravan and Light Trailer Towing Components Coupling Body For Ball CouplingsSAI Global - APACNo ratings yet
- Turtleback 2021 Sales Deck IssuuDocument18 pagesTurtleback 2021 Sales Deck IssuuTaoufik Lui MêmeNo ratings yet
- Self Assessment TrailerDocument4 pagesSelf Assessment TrailerSusan Jackman0% (1)
- "Camps and Picnic Grounds": Department of HealthDocument21 pages"Camps and Picnic Grounds": Department of HealthLeonesa Ananias LausNo ratings yet
- Trailer Life PDFDocument76 pagesTrailer Life PDFP1tuf1nha100% (1)
- SE FCNHE Campsite St. Fechins T&C 21.05.18Document5 pagesSE FCNHE Campsite St. Fechins T&C 21.05.18Gillian CaldwellNo ratings yet
- MotorCaravan Types and Fuel ConsumptionDocument13 pagesMotorCaravan Types and Fuel ConsumptionBill jonesNo ratings yet
- City of Johannesburg Land Use Scheme (Draft) : 7 June 2017Document71 pagesCity of Johannesburg Land Use Scheme (Draft) : 7 June 2017LCNo ratings yet
- VSB1 TP PDFDocument40 pagesVSB1 TP PDFΤΡΑΧΑΝΑΤΖΗΣ ΓΕΩΡΓΙΟΣNo ratings yet
- F3970 EsDocument4 pagesF3970 Esstefanovicana1No ratings yet
- A Strategic Approach To The Caravan and Camping Industry 2012Document118 pagesA Strategic Approach To The Caravan and Camping Industry 2012Varaprasad ChakriNo ratings yet
- H4212 Spread 3Document1 pageH4212 Spread 3Dimitris76No ratings yet
- Schematy Ektryczne Voyager Roczniki 96-00Document67 pagesSchematy Ektryczne Voyager Roczniki 96-00Stefan JarockiNo ratings yet