You might also like
- Pmi-Acp Exam Prep Study Guide: Extra Preparation for Pmi-Acp Certification ExaminationFrom EverandPmi-Acp Exam Prep Study Guide: Extra Preparation for Pmi-Acp Certification ExaminationNo ratings yet
- Swimlane For CybergovDocument2 pagesSwimlane For Cybergovcheng09No ratings yet
- Clerk (Income Maintenance): Passbooks Study GuideFrom EverandClerk (Income Maintenance): Passbooks Study GuideNo ratings yet
- Tto. Ik1: Curriculum DivisionDocument4 pagesTto. Ik1: Curriculum DivisionTheoSebastianNo ratings yet
- Manual of Operations: The Admissions OfficeDocument1 pageManual of Operations: The Admissions OfficeDarriex Queddeng Delos SantosNo ratings yet
- HEC Needs Based Scholarship Program Scholarship Application FormDocument16 pagesHEC Needs Based Scholarship Program Scholarship Application FormMuhammad MumtazNo ratings yet
- A School Admission and Registrar ProgramDocument3 pagesA School Admission and Registrar ProgramPhobe Sam100% (1)
- DepEd Baguio City Citizen's CharterDocument26 pagesDepEd Baguio City Citizen's CharterGreatDharz DjDiego SolanoyNo ratings yet
- Frontline ServicesDocument1 pageFrontline Servicesapi-379068374No ratings yet
- Exemption FormDocument3 pagesExemption FormMuhammad Umar FarooqNo ratings yet
- HECnbsDocument16 pagesHECnbsaizazNo ratings yet
- Factors Affecting The Acceptance of 4th Year BSA Students Around Cabanatuan City Towards The Section 7 and 9 of The Proposed Accountancy Act of 2021Document23 pagesFactors Affecting The Acceptance of 4th Year BSA Students Around Cabanatuan City Towards The Section 7 and 9 of The Proposed Accountancy Act of 2021Hydee ValinoNo ratings yet
- Financial Aid Application Form (For Local Students) - UG - Fall 22Document2 pagesFinancial Aid Application Form (For Local Students) - UG - Fall 22ShahriarNo ratings yet
- Registration Week Postgraduate Programme IPS UPSI Sem 1 2021Document1 pageRegistration Week Postgraduate Programme IPS UPSI Sem 1 2021Raja Muhd AzriNo ratings yet
- Kavayitri Bahinabai Chaudhari North Maharashtra University Front PageDocument1 pageKavayitri Bahinabai Chaudhari North Maharashtra University Front Pagebinebow517No ratings yet
- PSP GuidelinesDocument4 pagesPSP GuidelinesChimon LoveNo ratings yet
- Annex G-1 Individual Teacher EvaluationDocument1 pageAnnex G-1 Individual Teacher EvaluationRoyPintorNo ratings yet
- Flowchart AdmissionDocument4 pagesFlowchart Admissionmark españolaNo ratings yet
- Gso Application and AdmissionDocument12 pagesGso Application and AdmissionDbNo ratings yet
- Required Documents For EnrolmentDocument7 pagesRequired Documents For EnrolmentCamillus Carillo AngelesNo ratings yet
- Please Submit The Checklist Together With The Requirements.Document1 pagePlease Submit The Checklist Together With The Requirements.Luz DuaNo ratings yet
- Inbound 657161294165611710Document4 pagesInbound 657161294165611710BalesokoNo ratings yet
- John PDFDocument1 pageJohn PDFUMAK Juris DoctorsNo ratings yet
- Fully Funded Form 2020 21Document2 pagesFully Funded Form 2020 21Sikandar KhanNo ratings yet
- 5) Sop of Student Mobility (Inbound)Document2 pages5) Sop of Student Mobility (Inbound)NUR SYUHADAH ATIKA BINTI SHAHIDANNo ratings yet
- Kishore Vaigyanik Protsahan Yojana - 2011: Application Fo M For Stream SP (Medicine) RDocument6 pagesKishore Vaigyanik Protsahan Yojana - 2011: Application Fo M For Stream SP (Medicine) RAvinash TiwariNo ratings yet
- Omnibus T1 SGCDocument4 pagesOmnibus T1 SGCSheina CaradoNo ratings yet
- 22 UojDocument4 pages22 UojMuhammad HussainNo ratings yet
- (For Graduating Students Only) : Polytechnic University of The Philippines Office of The University RegistrarDocument1 page(For Graduating Students Only) : Polytechnic University of The Philippines Office of The University RegistrarShery Ann Fabreag FesalbonNo ratings yet
- KMU Job Application Form For BPS 05 and AboveDocument6 pagesKMU Job Application Form For BPS 05 and AboveAnonymous EIjnKecu0JNo ratings yet
- OAS Document Checklist FormDocument8 pagesOAS Document Checklist FormPenelope DaphneNo ratings yet
- CHECKLIST-OF-REQUIREMENTS-T1-APPLICANTS-1 (1)Document2 pagesCHECKLIST-OF-REQUIREMENTS-T1-APPLICANTS-1 (1)Vanessa PamparoNo ratings yet
- Omnibus Certification and Veracity FormsDocument4 pagesOmnibus Certification and Veracity FormsFely Grace Cole CamosNo ratings yet
- Obtain certificates from Karachi UniversityDocument1 pageObtain certificates from Karachi UniversityIdrees Jan JanNo ratings yet
- Republic of The Philippines Western Mindanao State University Zamboanga City Request For Publication of Vacant Position(s)Document1 pageRepublic of The Philippines Western Mindanao State University Zamboanga City Request For Publication of Vacant Position(s)Murnie PandaogNo ratings yet
- StuFAPs Application Checklist SY2019-2020Document1 pageStuFAPs Application Checklist SY2019-2020marilyn capuaNo ratings yet
- 9 Assistant Comlaint PDFDocument3 pages9 Assistant Comlaint PDFfawadNo ratings yet
- Law School Apps AndreiDocument3 pagesLaw School Apps AndreiMaisie ZabalaNo ratings yet
- Checklist Applicants (1) Senior HighDocument1 pageChecklist Applicants (1) Senior HighdonNo ratings yet
- San Beda College of Law: University of Santo Tomas Faculty of Civil LawDocument3 pagesSan Beda College of Law: University of Santo Tomas Faculty of Civil LawJames Erwin VelascoNo ratings yet
- Registration Week For Postgraduate Programme, Ips, Upsi: SEMESTER 2, SESSION 2021/2022 (MARCH 2022)Document1 pageRegistration Week For Postgraduate Programme, Ips, Upsi: SEMESTER 2, SESSION 2021/2022 (MARCH 2022)Leshainie ShankarenNo ratings yet
- Benilde Book II SY 2019-2020 IntakeDocument59 pagesBenilde Book II SY 2019-2020 IntakeDeeNo ratings yet
- RitikaDocument1 pageRitikaritikaaitisNo ratings yet
- Charter 2020Document118 pagesCharter 2020Charlene M. CarilloNo ratings yet
- Registration Steps and Forms - 06112017Document21 pagesRegistration Steps and Forms - 06112017ChongMYNo ratings yet
- Annex C - Checklist of Requirements and Omnibus Sworn StatementDocument1 pageAnnex C - Checklist of Requirements and Omnibus Sworn StatementJudith Guiao80% (15)
- O o o o o o o o o o o O: Khyber Medical UniversityDocument3 pagesO o o o o o o o o o o O: Khyber Medical UniversitySobar KhanNo ratings yet
- Enrollment Procedures FormDocument2 pagesEnrollment Procedures FormAnaliza MatildoNo ratings yet
- Enrolment Form Pre MedicalDocument2 pagesEnrolment Form Pre MedicalRamsha GNo ratings yet
- Individual Evaluation Sheet Teacher 1 ApplicantDocument1 pageIndividual Evaluation Sheet Teacher 1 ApplicantSusan ArongNo ratings yet
- Operations Management Course SyllabusDocument9 pagesOperations Management Course SyllabusDodoy Leandro Frincillo CrebelloNo ratings yet
- CLS.17.MBB.00021 RasDocument1 pageCLS.17.MBB.00021 RasjerryvicNo ratings yet
- Ranking FormDocument1 pageRanking Formjoy anne golveoNo ratings yet
- O o o o o o o o o o o O: Khyber Medical UniversityDocument2 pagesO o o o o o o o o o o O: Khyber Medical Universitysaqib yousafNo ratings yet
- PRE-U - EXAM ENTRY FORM - CSEC 2022-23 Stage 2Document3 pagesPRE-U - EXAM ENTRY FORM - CSEC 2022-23 Stage 2Marc CreatesNo ratings yet
- PG ApplicationDocument18 pagesPG ApplicationMansoor Outboard MotorsNo ratings yet
- Check List For Education LoanDocument1 pageCheck List For Education LoanDevesh FayeNo ratings yet
- HEC Scholarship Application Template 2016Document15 pagesHEC Scholarship Application Template 2016Asad Ullah KhanNo ratings yet
- Templates For The Annex C and DDocument4 pagesTemplates For The Annex C and Ddeary dianneNo ratings yet
- Admission Form Undergraduate Programs - Fall 17 - 0Document2 pagesAdmission Form Undergraduate Programs - Fall 17 - 0The ProfessorNo ratings yet
- Philippine Stock Exchange, Inc.: Via EdgeDocument5 pagesPhilippine Stock Exchange, Inc.: Via EdgeWag NasabiNo ratings yet
- Employee Status ReportDocument2 pagesEmployee Status ReportWag NasabiNo ratings yet
- 2115 Felix Huertas RD., Sta. Cruz, Manila Cellphone No. 0998-257-2724 / 0906-084-3370Document2 pages2115 Felix Huertas RD., Sta. Cruz, Manila Cellphone No. 0998-257-2724 / 0906-084-3370Wag NasabiNo ratings yet
- Fundamental Facts About Mental Health 2016Document112 pagesFundamental Facts About Mental Health 2016Jac1999No ratings yet
- Investing in MNH FinalDocument52 pagesInvesting in MNH FinalkabekuNo ratings yet
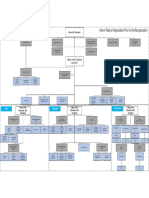
- Interim Table of Organization Prior To The ReorganizationDocument1 pageInterim Table of Organization Prior To The ReorganizationWag NasabiNo ratings yet
- Fundamental Facts 15 PDFDocument94 pagesFundamental Facts 15 PDFHazel LunaNo ratings yet
- EPP - TLE - Most-Essential-Learning-Competencies-MatrixDocument74 pagesEPP - TLE - Most-Essential-Learning-Competencies-MatrixRose Anne Santiago Dongon88% (26)
- Honesty Bus SystemDocument6 pagesHonesty Bus SystemWag NasabiNo ratings yet
- MH Promotion BookDocument310 pagesMH Promotion BookAde Kurnia100% (1)
- Multiple Predetermined Overhead RatesDocument4 pagesMultiple Predetermined Overhead RatesWag NasabiNo ratings yet
- Statement of Claims SCCDocument6 pagesStatement of Claims SCCJoseph Conrad De RamaNo ratings yet
- Absolute Deed of SaleDocument3 pagesAbsolute Deed of SaleNN DDL67% (3)
- The Stock Market and Investment: Is The Market A Sideshow?Document59 pagesThe Stock Market and Investment: Is The Market A Sideshow?kishoreNo ratings yet
- Booklet Stock Market PDFDocument28 pagesBooklet Stock Market PDFMohamed Ali SalemNo ratings yet
- Employee Handbook OverviewDocument18 pagesEmployee Handbook OverviewronsarmientoNo ratings yet
- Employee Handbook OverviewDocument18 pagesEmployee Handbook OverviewronsarmientoNo ratings yet
- Statement of Claims SCCDocument6 pagesStatement of Claims SCCJoseph Conrad De RamaNo ratings yet
- Ra 10591 BsaDocument13 pagesRa 10591 BsaWarlito D CabangNo ratings yet
- Rules and Regulations To Implement The Provisions of RA 10667Document33 pagesRules and Regulations To Implement The Provisions of RA 10667dyajeeNo ratings yet
- Application For A1D and Study Now Pay ETM Later PDFDocument1 pageApplication For A1D and Study Now Pay ETM Later PDFWag NasabiNo ratings yet
- Statement of Claims SCCDocument6 pagesStatement of Claims SCCJoseph Conrad De RamaNo ratings yet
- Statement of Claims SCCDocument6 pagesStatement of Claims SCCJoseph Conrad De RamaNo ratings yet
- 2009 Philippine Standard Industrial ClassificationDocument320 pages2009 Philippine Standard Industrial ClassificationBela Villamil100% (2)
- The Stockmarket BasicsDocument12 pagesThe Stockmarket BasicsWag NasabiNo ratings yet
- Forfeiture NoticeDocument1 pageForfeiture NoticeWag NasabiNo ratings yet
- CONTEMPO-RESERVATION+AGREEMENT+revised+02 08 13Document5 pagesCONTEMPO-RESERVATION+AGREEMENT+revised+02 08 13Wag NasabiNo ratings yet
- Classic Meeting Minutes TemplateDocument2 pagesClassic Meeting Minutes TemplateLouise Alyssa SazonNo ratings yet
- Workshop Instructor ContractDocument2 pagesWorkshop Instructor ContractWag NasabiNo ratings yet
- Topics: Nasopharyngeal CarcinomaDocument21 pagesTopics: Nasopharyngeal CarcinomaShruthi Y nursingNo ratings yet
- Respiratory Acidosis: Dr. Ann Valerie F. Habana Critical Care MedicineDocument21 pagesRespiratory Acidosis: Dr. Ann Valerie F. Habana Critical Care Medicineannv748687No ratings yet
- 2004 2005 Magnetom Flash 2 2Document64 pages2004 2005 Magnetom Flash 2 2Herick SavioneNo ratings yet
- 15 - Chapter 7 PDFDocument4 pages15 - Chapter 7 PDFRamNo ratings yet
- Human Anatomy 8th Edition Marieb Solutions Manual DownloadDocument14 pagesHuman Anatomy 8th Edition Marieb Solutions Manual DownloadMary Brown100% (23)
- Discover the history of basil herb in this Wikipedia articleDocument8 pagesDiscover the history of basil herb in this Wikipedia articleCinthia MarielaNo ratings yet
- CLUBFOOT GuidelineDocument111 pagesCLUBFOOT GuidelineNuhiat NahreenNo ratings yet
- File Number 1 1-1000 General InstructionsDocument80 pagesFile Number 1 1-1000 General InstructionsDaniel RstomNo ratings yet
- 25 OET Official Case Notes (Medicine)Document49 pages25 OET Official Case Notes (Medicine)Mesut KirazNo ratings yet
- Unit 8 Stress and Its EffectsDocument14 pagesUnit 8 Stress and Its Effectsafiya chandNo ratings yet
- Aemses Sof Be LCP 2021 2022Document16 pagesAemses Sof Be LCP 2021 2022ROMEO SANTILLANNo ratings yet
- Ants: Social Insects That Thrive in ColoniesDocument21 pagesAnts: Social Insects That Thrive in ColoniesSerajul SalekinNo ratings yet
- Viparita Karani - The Great Rejuvenator PoseDocument7 pagesViparita Karani - The Great Rejuvenator PoseDr Srinivasan Nenmeli -K100% (1)
- Bronquiolite Guidelines AAPDocument32 pagesBronquiolite Guidelines AAPDiego Guedes da SilvaNo ratings yet
- Cattle Pen Fattening Business Plan SummaryDocument65 pagesCattle Pen Fattening Business Plan Summaryprince kupa67% (3)
- Tu Berc U Losis: R T R TDocument56 pagesTu Berc U Losis: R T R TBj DonesNo ratings yet
- Discharge PlanDocument4 pagesDischarge Plandeo_gratias14No ratings yet
- Antisense Oligonucleotide Biotechnology, Applications and FutureDocument29 pagesAntisense Oligonucleotide Biotechnology, Applications and FuturesurojitarpitaNo ratings yet
- Hepatite B CoinfeçãoDocument31 pagesHepatite B Coinfeçãojefferson2392No ratings yet
- Incision and DrainageDocument8 pagesIncision and DrainageAbraham ChiuNo ratings yet
- Enderal Book CollectionDocument266 pagesEnderal Book CollectionMagazyn BotNo ratings yet
- Asia Pacific Dental Students Association Journal - APDSJV3N2Document117 pagesAsia Pacific Dental Students Association Journal - APDSJV3N2APDSANo ratings yet
- Biology 2nd Test CH Wise V1Document14 pagesBiology 2nd Test CH Wise V1ashfaq4985No ratings yet
- Incidence of Aphasia in Ischemic StrokeDocument9 pagesIncidence of Aphasia in Ischemic StrokeIndia SunshineNo ratings yet
- Adverse Event Tracking Log: Subject Initials Subject ID# Page ofDocument1 pageAdverse Event Tracking Log: Subject Initials Subject ID# Page ofPratyNo ratings yet
- CPH AssignmentDocument3 pagesCPH AssignmentChrystelle Mariano TibayNo ratings yet
- Haematology LastDocument65 pagesHaematology LastficocNo ratings yet
- Ortho ExamDocument9 pagesOrtho ExamPrince Rener Velasco Pera100% (2)
- S4 Integumentary SystemDocument9 pagesS4 Integumentary Systemcam broquelNo ratings yet
- All About Vitamins & MineralsDocument42 pagesAll About Vitamins & MineralsHristo AtanasovNo ratings yet