You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- IV Solution Cheat Sheet: Type Description Osmolality Use MiscellaneousDocument1 pageIV Solution Cheat Sheet: Type Description Osmolality Use MiscellaneousKristine Castillo100% (2)
- Power Grid Corporation of India Limited Construction ManagementDocument8 pagesPower Grid Corporation of India Limited Construction ManagementRahul RanjanNo ratings yet
- Project On Baggage Handling and AcceptanceDocument52 pagesProject On Baggage Handling and AcceptanceKiran Reddy50% (2)
- The Emerald Tablets of Thoth Toth The Atlantean - Table 05Document5 pagesThe Emerald Tablets of Thoth Toth The Atlantean - Table 05Georgiana BealcuNo ratings yet
- Webinar Rosuvastatin Perki BandungDocument54 pagesWebinar Rosuvastatin Perki BandungSurya RajNo ratings yet
- Patient Satisfaction with Outpatient Services at Hospitals in 7 Indonesian ProvincesDocument8 pagesPatient Satisfaction with Outpatient Services at Hospitals in 7 Indonesian ProvincesAcil agustinNo ratings yet
- Roberts and Hedges: Clinical Procedures in Emergency Medicine (5th Edition)Document2 pagesRoberts and Hedges: Clinical Procedures in Emergency Medicine (5th Edition)Surya RajNo ratings yet
- Factors Contributing To Patients' Satisfaction With Public Health Services in The Eastern Cape, South AfricaDocument11 pagesFactors Contributing To Patients' Satisfaction With Public Health Services in The Eastern Cape, South AfricaSurya RajNo ratings yet
- Patient Satisfaction with Outpatient Services at Hospitals in 7 Indonesian ProvincesDocument8 pagesPatient Satisfaction with Outpatient Services at Hospitals in 7 Indonesian ProvincesAcil agustinNo ratings yet
- Not All CCBs Provide Equal 24-Hour ProtectionDocument21 pagesNot All CCBs Provide Equal 24-Hour ProtectionSurya RajNo ratings yet
- Bmjopen 2018 024335Document6 pagesBmjopen 2018 024335Surya RajNo ratings yet
- Protecting NVAF Patients From Stroke in Pandemic Era: MA-M - RIV-ID-0090-1Document40 pagesProtecting NVAF Patients From Stroke in Pandemic Era: MA-M - RIV-ID-0090-1Surya RajNo ratings yet
- An Approach For Management of VTE Patients in New Normal: MA-M - RIV-ID-0091-1Document36 pagesAn Approach For Management of VTE Patients in New Normal: MA-M - RIV-ID-0091-1Surya RajNo ratings yet
- Tight Blood Pressure Control Reduces Diabetes RisksDocument11 pagesTight Blood Pressure Control Reduces Diabetes RisksSurya RajNo ratings yet
- EMD2 - K10 - Metabolic Emergencies (Anak)Document47 pagesEMD2 - K10 - Metabolic Emergencies (Anak)Surya RajNo ratings yet
- The importance of a balanced ω-6 to ω-3 ratio in the prevention and management of obesityDocument6 pagesThe importance of a balanced ω-6 to ω-3 ratio in the prevention and management of obesitySurya RajNo ratings yet
- Bacterial Meningitis: Jeremy Fernando (2011)Document2 pagesBacterial Meningitis: Jeremy Fernando (2011)Surya RajNo ratings yet
- Pendekatan Diagnosis OsteoporosisDocument3 pagesPendekatan Diagnosis OsteoporosisSurya RajNo ratings yet
- 05 - 203perkembangan Terkini Diagnosis Dan Penatalaksanaan Imflammatory Bowel Disease PDFDocument6 pages05 - 203perkembangan Terkini Diagnosis Dan Penatalaksanaan Imflammatory Bowel Disease PDFrisda aulia putriNo ratings yet
- Gastritis 508Document8 pagesGastritis 508FaichalMartadinataNo ratings yet
- 10 1001@jamacardio 2017 0119Document1 page10 1001@jamacardio 2017 0119Surya RajNo ratings yet
- 475 483Document9 pages475 483Surya RajNo ratings yet
- Weight-Length Chart for Boys from Birth to 2 Years OldDocument1 pageWeight-Length Chart for Boys from Birth to 2 Years OldMalisa LukmanNo ratings yet
- Bacterial Meningitis: Jeremy Fernando (2011)Document2 pagesBacterial Meningitis: Jeremy Fernando (2011)Surya RajNo ratings yet
- Unit 07Document9 pagesUnit 07ZackNo ratings yet
- DE712-014 Parts Manual - 712014 1 en Rev 1Document248 pagesDE712-014 Parts Manual - 712014 1 en Rev 1Emi DominguezNo ratings yet
- 17 The Tarrying TimeDocument22 pages17 The Tarrying Timeapi-303147801100% (1)
- Effect of Blast Induced Vibrations On GroutDocument55 pagesEffect of Blast Induced Vibrations On GroutDavid marpaungNo ratings yet
- Man and Mystery Vol 13 - Monsters and Cryptids (Rev06)Document139 pagesMan and Mystery Vol 13 - Monsters and Cryptids (Rev06)Pablo Jr AgsaludNo ratings yet
- 60 Minutes-60 Questions: Mathematics TestDocument15 pages60 Minutes-60 Questions: Mathematics TestJihyun YeonNo ratings yet
- Persian Polymath Physician Al-Rāzī's Life and WorksDocument10 pagesPersian Polymath Physician Al-Rāzī's Life and WorksAnonymous 29PN6AZTNo ratings yet
- Diagnoza Wstępna Klasa IDocument3 pagesDiagnoza Wstępna Klasa IMagda StręciwilkNo ratings yet
- Statics: Vector Mechanics For EngineersDocument32 pagesStatics: Vector Mechanics For EngineersArdaNo ratings yet
- HP DeskJet Report POM 20150413Document5 pagesHP DeskJet Report POM 20150413Carolina DelgadoNo ratings yet
- 2015 - 3 Lennar Concord Proposal PDFDocument148 pages2015 - 3 Lennar Concord Proposal PDFEric LiptonNo ratings yet
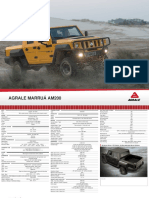
- Off Road and Military Vehicles Off Road Vehicles Agrale Marruaam200 1Document2 pagesOff Road and Military Vehicles Off Road Vehicles Agrale Marruaam200 1Victor SilvaNo ratings yet
- 02-A Guide To Chinese Classical MythologyDocument22 pages02-A Guide To Chinese Classical MythologyNguyen Pham Thien ThanhNo ratings yet
- 22nd Annual Report 2021-22Document155 pages22nd Annual Report 2021-22Karthic Selvam KandavelNo ratings yet
- 2K6 Ec 307 (P) : Basic Electronics Lab: Sessional Work AssessmentDocument1 page2K6 Ec 307 (P) : Basic Electronics Lab: Sessional Work AssessmentJoseph JohnNo ratings yet
- Nexon Genuine AccessoriesDocument15 pagesNexon Genuine AccessoriesjagaaniNo ratings yet
- Brazed Tool ArDocument5 pagesBrazed Tool ArRoni MustafiqNo ratings yet
- Manual: KFD2-UT-E 1Document20 pagesManual: KFD2-UT-E 1Kyrie AbayaNo ratings yet
- Kant ParadigmDocument265 pagesKant ParadigmkairospandemosNo ratings yet
- Presidential Decree No. 1616 establishes Intramuros AdministrationDocument22 pagesPresidential Decree No. 1616 establishes Intramuros AdministrationRemiel Joseph Garniel BataoNo ratings yet
- The Human BodyDocument17 pagesThe Human BodyRuthie MendozaNo ratings yet
- Well Components: Petroleum Production Engineering. DOI: © 2007 Elsevier Inc. All Rights ReservedDocument15 pagesWell Components: Petroleum Production Engineering. DOI: © 2007 Elsevier Inc. All Rights Reservedsoran najebNo ratings yet
- Cats Meow Edition 3 PDFDocument320 pagesCats Meow Edition 3 PDFbrunokfouriNo ratings yet
- Berry phase in the simple harmonic oscillatorDocument14 pagesBerry phase in the simple harmonic oscillatora2618765No ratings yet
- Sunningdale School Notes Summer 2022Document12 pagesSunningdale School Notes Summer 2022sunningdaleschoolNo ratings yet
- 1,16Document138 pages1,16niztgirlNo ratings yet