You might also like
- The Burden of Adult ADHD in Comorbid Psychiatric and Neurological DisordersFrom EverandThe Burden of Adult ADHD in Comorbid Psychiatric and Neurological DisordersNo ratings yet
- Neurofeedback AdhdDocument8 pagesNeurofeedback AdhdAlbertoNo ratings yet
- Neurofeedback in ADHD - 2014Document18 pagesNeurofeedback in ADHD - 2014GOLDFINCHNo ratings yet
- Neuropsychologically-Informed PT in Ados and Adults With ADHD - 2014Document10 pagesNeuropsychologically-Informed PT in Ados and Adults With ADHD - 2014GOLDFINCHNo ratings yet
- karch2013Document20 pageskarch2013Laura PGNo ratings yet
- De Zeeuw Et Al. - 2012 - Deficits in Cognitive Control, Timing and Reward Sensitivity Appear To Be Dissociable in ADHDDocument9 pagesDe Zeeuw Et Al. - 2012 - Deficits in Cognitive Control, Timing and Reward Sensitivity Appear To Be Dissociable in ADHDTao CmNo ratings yet
- Pmid 35215389Document23 pagesPmid 35215389Lilly HiliutaNo ratings yet
- Pone 0215095Document26 pagesPone 0215095GokushimakNo ratings yet
- Epigenetics and ADHDDocument26 pagesEpigenetics and ADHDJulius Cesar RomanNo ratings yet
- Reaction Time Assessment in Children with ADHDDocument6 pagesReaction Time Assessment in Children with ADHDjhonNo ratings yet
- cells-10-02156Document34 pagescells-10-02156Isabely AmabilyNo ratings yet
- Paulea - Rowlandb.fergusona - Chelonisc.tannockd - Swansone.castellanos. ADHD Characteristics Interventions ModelsDocument21 pagesPaulea - Rowlandb.fergusona - Chelonisc.tannockd - Swansone.castellanos. ADHD Characteristics Interventions ModelsRute Almeida RomãoNo ratings yet
- Estructura Ejecutiva A Los 3 AñosDocument17 pagesEstructura Ejecutiva A Los 3 AñosRominaNo ratings yet
- RetrieveDocument30 pagesRetrieveDra. Alejandra De la FuenteNo ratings yet
- Múnger Etal (2021) Behavioral and Neurophygiological Markers of ADHDDocument10 pagesMúnger Etal (2021) Behavioral and Neurophygiological Markers of ADHDVander PereiraNo ratings yet
- Effects of Neurofeedback in Children With Attention-Deficit:Hyperactivity Disorder - A Systematic ReviewDocument13 pagesEffects of Neurofeedback in Children With Attention-Deficit:Hyperactivity Disorder - A Systematic ReviewLeonardo AndujoNo ratings yet
- Early Intervention for ADHD: A Neurodevelopmental PerspectiveDocument11 pagesEarly Intervention for ADHD: A Neurodevelopmental PerspectiveGuille monsterNo ratings yet
- The Neurobiological Basis of AdhdDocument7 pagesThe Neurobiological Basis of AdhdSara OlmosNo ratings yet
- 2020 Article 501Document22 pages2020 Article 501Ricardo GalhardoniNo ratings yet
- Nihms-36247 230306 144401Document11 pagesNihms-36247 230306 144401Florencia DrakslerNo ratings yet
- Precision Medicine Care in ADHD The Case For Neural Excitation and InhibitionDocument12 pagesPrecision Medicine Care in ADHD The Case For Neural Excitation and InhibitionDaria DanielNo ratings yet
- The Neurocognitive Pro File of Attention-Deficit/Hyperactivity Disorder: A Review of Meta-AnalysesDocument15 pagesThe Neurocognitive Pro File of Attention-Deficit/Hyperactivity Disorder: A Review of Meta-AnalysesPSIQUIATRÍA HUFANo ratings yet
- Tera Pia Me Taco Gnit IvaDocument11 pagesTera Pia Me Taco Gnit IvaInfocoem InfocoemNo ratings yet
- 2008 Lopez Et Al - TOBSJDocument9 pages2008 Lopez Et Al - TOBSJvlopezhNo ratings yet
- The New Science of Attention Deficit Hyperactivity Disorder: News From The Cutting Edge of Research ScienceDocument6 pagesThe New Science of Attention Deficit Hyperactivity Disorder: News From The Cutting Edge of Research Science-No ratings yet
- ADHD and Impact On LanguageDocument13 pagesADHD and Impact On LanguageayundiarciizpNo ratings yet
- 2007 - The Neuropsychiatry of Impulsivity. - Chamberlain, SahakianDocument7 pages2007 - The Neuropsychiatry of Impulsivity. - Chamberlain, SahakianmvictabNo ratings yet
- Feminism in IndiaDocument2 pagesFeminism in IndiaonlyforpahedownloadsNo ratings yet
- Research Paper On Attention Deficit Hyperactivity DisorderDocument6 pagesResearch Paper On Attention Deficit Hyperactivity DisorderzxnrvkrifNo ratings yet
- Ijpr 2015 112 PDFDocument8 pagesIjpr 2015 112 PDFbellaNo ratings yet
- Measure Fuller, K. H., Monna, W., David, W., & Sanderlin, MDocument1 pageMeasure Fuller, K. H., Monna, W., David, W., & Sanderlin, MMohamad Nazrin YahayaNo ratings yet
- Sensory Process Disorder NeuropsychDocument9 pagesSensory Process Disorder NeuropsychBruno 21No ratings yet
- Detection of Adult Attention Deficit Hyperactivity Disorder With Cognitive Complaint Experience of A French Memory CenterDocument9 pagesDetection of Adult Attention Deficit Hyperactivity Disorder With Cognitive Complaint Experience of A French Memory CenterJasonNo ratings yet
- Primer: in UteroDocument6 pagesPrimer: in UteroSandra MedinaNo ratings yet
- Fuermaier Et Al. 2017Document27 pagesFuermaier Et Al. 2017Malka SarmientoNo ratings yet
- Anhedonia As A Central Factor in Depression)Document18 pagesAnhedonia As A Central Factor in Depression)Gkani ChrysoulaNo ratings yet
- ADHD ADD - ManagementDocument8 pagesADHD ADD - Managementdeepak_anvekarNo ratings yet
- Transcranial Direct Current Stimulation Improves CDocument13 pagesTranscranial Direct Current Stimulation Improves CCarolina Robledo CastroNo ratings yet
- Neuro FeedbackDocument14 pagesNeuro FeedbackMar LindaNo ratings yet
- Sustained Effects of Neurofeedback in ADHD: A Systematic Review and Meta AnalysisDocument13 pagesSustained Effects of Neurofeedback in ADHD: A Systematic Review and Meta AnalysisBrigita de BrillarNo ratings yet
- Effects of Physical Exercise On Children With Attention Deficit Hyperactivity DisorderDocument6 pagesEffects of Physical Exercise On Children With Attention Deficit Hyperactivity DisorderRaoof ARIFNo ratings yet
- Mills & Tamnes, 2014.methods and Considerations For Longitudinal Structural Brain Imaging Analysis Across DevelopmentDocument10 pagesMills & Tamnes, 2014.methods and Considerations For Longitudinal Structural Brain Imaging Analysis Across DevelopmentSu AjaNo ratings yet
- Adhd. BioscienceDocument18 pagesAdhd. BioscienceJuan Carlos Muñoz SalmerónNo ratings yet
- Chapter 7 - Attention Deficit Disorder - 2018 - Integrative MedicineDocument15 pagesChapter 7 - Attention Deficit Disorder - 2018 - Integrative MedicineandreNo ratings yet
- Brainsci 12 00959 v2Document14 pagesBrainsci 12 00959 v2DrShitgenstein RequiemNo ratings yet
- 1 PDFDocument19 pages1 PDFRoberto Alexis Molina CampuzanoNo ratings yet
- Adhd OrgDocument74 pagesAdhd OrgNeil Marzon PaguicanNo ratings yet
- Clinical Applicability and Cutoff Values For AnDocument9 pagesClinical Applicability and Cutoff Values For AnDayanne SilvaNo ratings yet
- Genro Et Al., 2010Document15 pagesGenro Et Al., 2010priyaNo ratings yet
- Minder Et Al 2019Document16 pagesMinder Et Al 2019horanvera10No ratings yet
- Perceptual-Motor Skills Reconstruction Program Improves Executive Functions in Children With Attention-Deficit/Hyperactivity DisorderDocument11 pagesPerceptual-Motor Skills Reconstruction Program Improves Executive Functions in Children With Attention-Deficit/Hyperactivity DisorderNisa UrrohmatushNo ratings yet
- 2014 Article 542Document10 pages2014 Article 542abhilasha8dwivediNo ratings yet
- Sun2019 PDFDocument10 pagesSun2019 PDFCristinaNo ratings yet
- Antshel2015 PDFDocument19 pagesAntshel2015 PDFCristinaNo ratings yet
- Currentstatusof Cognitivebehavioral Therapyforadult Attention-Deficit Hyperactivity DisorderDocument13 pagesCurrentstatusof Cognitivebehavioral Therapyforadult Attention-Deficit Hyperactivity Disordershofa nur rahmannisaNo ratings yet
- Fenotipo TDAHDocument14 pagesFenotipo TDAHBrigite AzevedoNo ratings yet
- Meta-Analysis of Memory and ExecutiveDocument25 pagesMeta-Analysis of Memory and ExecutiveJesús AraozNo ratings yet
- Rationale For Dietary Antioxidant Treatment of ADHDocument20 pagesRationale For Dietary Antioxidant Treatment of ADHFernando SouzaNo ratings yet
- ADHD - EnglishDocument64 pagesADHD - EnglishNataly XanthyNo ratings yet
- 2009 Can Cognitive Exercise Prevent The Onset of Dementia Systematic Review of Randomized Clinical Trials With Longitudinal Follow UpDocument9 pages2009 Can Cognitive Exercise Prevent The Onset of Dementia Systematic Review of Randomized Clinical Trials With Longitudinal Follow UpSergio Machado NeurocientistaNo ratings yet
- Stress: A Concept Analysis: Patricia M. Goodnite, RN-BCDocument4 pagesStress: A Concept Analysis: Patricia M. Goodnite, RN-BCJose Alonso Aguilar ValeraNo ratings yet
- 5 7. Dutta Et Al-2018-American Journal of Speech-Language PathologyDocument29 pages5 7. Dutta Et Al-2018-American Journal of Speech-Language PathologyDimas Ade MahendraNo ratings yet
- New Research: Joseph H. Beitchman,, E.B. Brownlie,, Lin BaoDocument17 pagesNew Research: Joseph H. Beitchman,, E.B. Brownlie,, Lin BaoJose Alonso Aguilar ValeraNo ratings yet
- The Challenge of Language Assessment For African American English-Speaking Children: A Historical PerspectiveDocument10 pagesThe Challenge of Language Assessment For African American English-Speaking Children: A Historical PerspectiveJose Alonso Aguilar ValeraNo ratings yet
- Longo 2017Document7 pagesLongo 2017Jose Alonso Aguilar ValeraNo ratings yet
- A Dual Representation Theory of Posttraumatic Stress DisorderDocument17 pagesA Dual Representation Theory of Posttraumatic Stress DisorderJose Alonso Aguilar ValeraNo ratings yet
- Neuroscience and Biobehavioral Reviews: Holger Ursin, Hege R. EriksenDocument5 pagesNeuroscience and Biobehavioral Reviews: Holger Ursin, Hege R. EriksenJose Alonso Aguilar ValeraNo ratings yet
- Socioeconomic Status and Stress-Induced Increases in Interleukin-6Document10 pagesSocioeconomic Status and Stress-Induced Increases in Interleukin-6Jose Alonso Aguilar ValeraNo ratings yet
- Rice 2016Document11 pagesRice 2016Jose Alonso Aguilar ValeraNo ratings yet
- Psychological Theories of Posttraumatic Stress DisorderDocument38 pagesPsychological Theories of Posttraumatic Stress Disordermsl497100% (1)
- Cognitive Activation Theory of Stress, Sensitization, and Common Health ComplaintsDocument7 pagesCognitive Activation Theory of Stress, Sensitization, and Common Health ComplaintsJose Alonso Aguilar ValeraNo ratings yet
- Theories and Mechanisms of Aging: Charles A. CefaluDocument16 pagesTheories and Mechanisms of Aging: Charles A. CefaluJose Alonso Aguilar ValeraNo ratings yet
- The Autism Spectrum Quotient: Children's Version (AQ-Child) : Ó Springer Science+Business Media, LLC 2007Document11 pagesThe Autism Spectrum Quotient: Children's Version (AQ-Child) : Ó Springer Science+Business Media, LLC 2007Jose Alonso Aguilar ValeraNo ratings yet
- Cohen Et Al. (2016) A Stage Model of Stress and DiseaseDocument8 pagesCohen Et Al. (2016) A Stage Model of Stress and DiseaseIrzaFreecsNo ratings yet
- Neuroglia in The Autistic Brain: Evidence From A Preclinical ModelDocument17 pagesNeuroglia in The Autistic Brain: Evidence From A Preclinical ModelJose Alonso Aguilar ValeraNo ratings yet
- Does Theory of Mind Training Enhance Empathy in Autism?Document8 pagesDoes Theory of Mind Training Enhance Empathy in Autism?Jose Alonso Aguilar ValeraNo ratings yet
- The Childhood Autism Spectrum Test (CAST) :spanish Adaptation and ValidationDocument8 pagesThe Childhood Autism Spectrum Test (CAST) :spanish Adaptation and ValidationJose Alonso Aguilar ValeraNo ratings yet
- Silverman 2010Document13 pagesSilverman 2010Jose Alonso Aguilar ValeraNo ratings yet
- The Autism Spectrum Quotient: Children's Version (AQ-Child) : Ó Springer Science+Business Media, LLC 2007Document11 pagesThe Autism Spectrum Quotient: Children's Version (AQ-Child) : Ó Springer Science+Business Media, LLC 2007Jose Alonso Aguilar ValeraNo ratings yet
- Silverman 2010Document13 pagesSilverman 2010Jose Alonso Aguilar ValeraNo ratings yet
- Construct Validity and Cross Validity of A Test Battery Modeling Autism Spectrum Disorder (ASD) in MiceDocument15 pagesConstruct Validity and Cross Validity of A Test Battery Modeling Autism Spectrum Disorder (ASD) in MiceJose Alonso Aguilar ValeraNo ratings yet
- A Screening Instrument For Autism Months of Age: A Follow-Up StudyDocument9 pagesA Screening Instrument For Autism Months of Age: A Follow-Up StudyJose Alonso Aguilar ValeraNo ratings yet
- Dumont Mathieu2005Document10 pagesDumont Mathieu2005Jose Alonso Aguilar ValeraNo ratings yet
- Dumont Mathieu2005Document10 pagesDumont Mathieu2005Jose Alonso Aguilar ValeraNo ratings yet
- Speech and Communication Changes Reported by People With Parkinson's DiseaseDocument11 pagesSpeech and Communication Changes Reported by People With Parkinson's DiseaseJose Alonso Aguilar ValeraNo ratings yet
- Nygren 2012Document11 pagesNygren 2012Jose Alonso Aguilar ValeraNo ratings yet
- Evidence-Based Treatment of Voice and Speech Disorders in Parkinson DiseaseDocument7 pagesEvidence-Based Treatment of Voice and Speech Disorders in Parkinson DiseaseJose Alonso Aguilar ValeraNo ratings yet
- Screening Strategies For Autism Spectrum Disorders in Pediatric Primary CareDocument6 pagesScreening Strategies For Autism Spectrum Disorders in Pediatric Primary CareJose Alonso Aguilar ValeraNo ratings yet
- Speech and Communication Changes Reported by People With Parkinson's DiseaseDocument11 pagesSpeech and Communication Changes Reported by People With Parkinson's DiseaseJose Alonso Aguilar ValeraNo ratings yet
- Speech and Communication Changes Reported by People With Parkinson's DiseaseDocument11 pagesSpeech and Communication Changes Reported by People With Parkinson's DiseaseJose Alonso Aguilar ValeraNo ratings yet
- SPECIFICATIONS For Constant Temperature and Humidity ChamberDocument5 pagesSPECIFICATIONS For Constant Temperature and Humidity Chamber彭以和No ratings yet
- Unit 1 Cultural Issues and ValuesDocument3 pagesUnit 1 Cultural Issues and ValuesACHRAF DOUKARNENo ratings yet
- Insight IAS Prelims 2020 Test 13 S PDFDocument66 pagesInsight IAS Prelims 2020 Test 13 S PDFApooNo ratings yet
- UntitledDocument19 pagesUntitledSmiles PrintingNo ratings yet
- Detailed Teaching Syllabus (DTS) and Instructor Guide (Ig'S)Document10 pagesDetailed Teaching Syllabus (DTS) and Instructor Guide (Ig'S)Charo Gironella100% (1)
- Challenge - Redefining Business Sustainability in Philippine Business Culture (J&T Express)Document4 pagesChallenge - Redefining Business Sustainability in Philippine Business Culture (J&T Express)ANGELICA GABRIELLE UYNo ratings yet
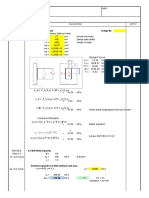
- Weld Check: I. Connection Properties Bridge IDDocument3 pagesWeld Check: I. Connection Properties Bridge IDJemicah YumenaNo ratings yet
- JNTUK - Revised Syllabus For M. Tech Transportation EngineeringDocument20 pagesJNTUK - Revised Syllabus For M. Tech Transportation Engineeringvamsi_rsNo ratings yet
- Linear RegressionDocument15 pagesLinear RegressionAnil Bera67% (3)
- Kelas Xii - May I Help You - Chapter 1Document2 pagesKelas Xii - May I Help You - Chapter 1Syifa Fauziah50% (2)
- STATISTIC AND PROBABILITY 1ST QUARTER EXAM - SourceDocument72 pagesSTATISTIC AND PROBABILITY 1ST QUARTER EXAM - SourceAmanda Dinah RamilNo ratings yet
- Seismic Force CANADA Code - CNBC2005-V421Document7 pagesSeismic Force CANADA Code - CNBC2005-V421Niko NištićNo ratings yet
- Dr. Amir Shafeeq: Associate ProfessorDocument9 pagesDr. Amir Shafeeq: Associate ProfessorMudasar RasheedNo ratings yet
- ShipDocument3 pagesShipAshnee SewockNo ratings yet
- Fred K. Schaefer and The Science of GeographyDocument6 pagesFred K. Schaefer and The Science of GeographyAbraham Paulsen BilbaoNo ratings yet
- Gauss's LawDocument10 pagesGauss's LawAliceAlormenuNo ratings yet
- Simple Reflex Arc Week 2Document4 pagesSimple Reflex Arc Week 2Ahmed KhaledNo ratings yet
- Gap Year Thesis StatementDocument4 pagesGap Year Thesis Statementbrookelordmanchester100% (1)
- SurveyingDocument14 pagesSurveyingkNo ratings yet
- Finals Quiz 1 ReviewerDocument20 pagesFinals Quiz 1 ReviewerAngelo DongonNo ratings yet
- Valvoline Lithium Ep2 GreaseDocument1 pageValvoline Lithium Ep2 GreaseDicky PratamaNo ratings yet
- V2k (Voice To Skull: Download Free PDFDocument43 pagesV2k (Voice To Skull: Download Free PDFLazlo SecretNo ratings yet
- RESIDUE CURVE MAPS GUIDEDocument5 pagesRESIDUE CURVE MAPS GUIDEWali AhsanNo ratings yet
- Biomechanical Considerations For The Restoration of Endodontically Treated TeethDocument13 pagesBiomechanical Considerations For The Restoration of Endodontically Treated TeethSoraya BouchammaNo ratings yet
- Eltorai, Ibrahim M A Spotlight On The History of Ancient EgyptianDocument215 pagesEltorai, Ibrahim M A Spotlight On The History of Ancient EgyptianJonas PsontomfanceNo ratings yet
- New Microsoft Word DocumentDocument2 pagesNew Microsoft Word DocumentSwarnim KumbhareNo ratings yet
- SYNPOL D Service Manual E V20!09!05Document60 pagesSYNPOL D Service Manual E V20!09!05auto etrustNo ratings yet
- Pervious ConcreteDocument4 pagesPervious ConcretesuwashNo ratings yet
- Water Using Volumetric Karl Fischer Titration: Standard Test Method ForDocument12 pagesWater Using Volumetric Karl Fischer Titration: Standard Test Method ForSusana Smaldone MillánNo ratings yet
- CSC415 LAB ASSIGNMENT 1 TOPIC 2-5Document5 pagesCSC415 LAB ASSIGNMENT 1 TOPIC 2-5Amir AimanNo ratings yet