You might also like
- Ankylosed Primary Teeth With No Permanent Successors: What Do You Do? - Part 1Document7 pagesAnkylosed Primary Teeth With No Permanent Successors: What Do You Do? - Part 1Isabela GD GheNo ratings yet
- Prevalence and Change of Malocclusions From Primary To Early Permanent Dentition: A Longitudinal StudyDocument7 pagesPrevalence and Change of Malocclusions From Primary To Early Permanent Dentition: A Longitudinal StudyAmadeaNo ratings yet
- Mandibular Second Molar Eruption Difficulties Related To The Maintenance of Arch Perimeter in The Mixed DentitionDocument7 pagesMandibular Second Molar Eruption Difficulties Related To The Maintenance of Arch Perimeter in The Mixed DentitionMaha Ahmed SolimanNo ratings yet
- A Comparison of Treatment Results of Adult Deep-Bite Cases Treated With Lingual and Labial Fixed AppliancesDocument7 pagesA Comparison of Treatment Results of Adult Deep-Bite Cases Treated With Lingual and Labial Fixed AppliancesScribd AccountNo ratings yet
- Bompereta Labial 2Document7 pagesBompereta Labial 2Aleja LombanaNo ratings yet
- Todentj 13 137Document6 pagesTodentj 13 137luis alejandroNo ratings yet
- 10 1067@mpr 2000 107113Document7 pages10 1067@mpr 2000 107113gbaez.88No ratings yet
- Radiology in Pediatric Dentistry 2Document44 pagesRadiology in Pediatric Dentistry 2Aima Cuba100% (1)
- Twin Blok 4Document11 pagesTwin Blok 4KosanKucingGendutPurwokertoNo ratings yet
- 1 s2.0 S2212443814000186 Main 2Document6 pages1 s2.0 S2212443814000186 Main 2Pau ContrerasNo ratings yet
- Research ArticleDocument10 pagesResearch Articleselvaortho94No ratings yet
- Anesthetic Technique For Inferior Alveolar Nerve Block: A New ApproachDocument5 pagesAnesthetic Technique For Inferior Alveolar Nerve Block: A New ApproachIonela AlexandraNo ratings yet
- Desarrollo de Cerámicas Híbridas para Restauraciones PersonalizadasDocument9 pagesDesarrollo de Cerámicas Híbridas para Restauraciones Personalizadasbarrera2001No ratings yet
- Rapid Maxillary Expansion. Is It Better in The Mixed or in The Permanent Dentition?Document8 pagesRapid Maxillary Expansion. Is It Better in The Mixed or in The Permanent Dentition?Gustavo AnteparraNo ratings yet
- 4 Intraoral Radiographic TechniquesDocument35 pages4 Intraoral Radiographic TechniquesDan 04100% (1)
- 2019 Mcnamara 40 AñosDocument13 pages2019 Mcnamara 40 AñosshadiNo ratings yet
- Impacted Maxillary Canines-A Review. - American Journal of Orthodontics and Dentofacial Orthopedics, 101-159, 1992 PDFDocument13 pagesImpacted Maxillary Canines-A Review. - American Journal of Orthodontics and Dentofacial Orthopedics, 101-159, 1992 PDFPia ContrerasNo ratings yet
- Class II Correction With The Cantilever Bite Jumper: Original ArticleDocument9 pagesClass II Correction With The Cantilever Bite Jumper: Original ArticleNaveenNo ratings yet
- Alqerban2015 (Radiographic Predictors)Document10 pagesAlqerban2015 (Radiographic Predictors)Srishti SyalNo ratings yet
- Effect of Mandibular First Molar Mesialization On Alveolar Bone Height: A Split Mouth StudyDocument7 pagesEffect of Mandibular First Molar Mesialization On Alveolar Bone Height: A Split Mouth StudyRockey ShrivastavaNo ratings yet
- Al-Dumaini - 2018 - A Novel Approach For Treatment of Skeletal Class II Malocclusion - Miniplates-Based Skeletal AnchorageDocument9 pagesAl-Dumaini - 2018 - A Novel Approach For Treatment of Skeletal Class II Malocclusion - Miniplates-Based Skeletal AnchoragefishribbonNo ratings yet
- Comparison of Skeletal and Dental Changes Between 2-Point and 4-Point Rapid PalatalDocument8 pagesComparison of Skeletal and Dental Changes Between 2-Point and 4-Point Rapid PalatalManena RivoltaNo ratings yet
- Journal of The World Federation of Orthodontists: Nasser Alqahtani, Brian Preston, Guoqiang GuanDocument5 pagesJournal of The World Federation of Orthodontists: Nasser Alqahtani, Brian Preston, Guoqiang GuanPaulanermNo ratings yet
- (Ijacr)Document4 pages(Ijacr)dhelianjaniNo ratings yet
- Apical Root Resorption of Incisors After Orthodontic Treatment of Impacted Maxillary Canines, Radiographic StudyDocument9 pagesApical Root Resorption of Incisors After Orthodontic Treatment of Impacted Maxillary Canines, Radiographic StudyJose CollazosNo ratings yet
- Indirect Pulp Capping Versus Pulpotomy For Treating Deep Carious Lesions Approaching The Pulp in Primary Teeth: A Systematic ReviewDocument6 pagesIndirect Pulp Capping Versus Pulpotomy For Treating Deep Carious Lesions Approaching The Pulp in Primary Teeth: A Systematic ReviewKingkan HongyonNo ratings yet
- Twin SupportDocument11 pagesTwin SupportArwa Said Shokri KhalilNo ratings yet
- CLASSIC ARTICLE Clinical Measurement and EvaluationDocument5 pagesCLASSIC ARTICLE Clinical Measurement and EvaluationJesusCordoba100% (2)
- Hayrax Con Mascara Facial PDFDocument8 pagesHayrax Con Mascara Facial PDFSantos LopNo ratings yet
- Patient-Assessed Security Changes When Replacing Mandibular Complete DenturesDocument7 pagesPatient-Assessed Security Changes When Replacing Mandibular Complete Denturesjinny1_0No ratings yet
- FM Article 52892 en 1Document11 pagesFM Article 52892 en 1Erika NuñezNo ratings yet
- 30121-Article Text-56500-1-10-20200810Document7 pages30121-Article Text-56500-1-10-20200810IfadahNo ratings yet
- 8907 1yk4o27Document6 pages8907 1yk4o27Zahid ManzoorNo ratings yet
- Pi Is 0889540611000370Document5 pagesPi Is 0889540611000370ucsurortodonciaNo ratings yet
- Milares InclinadosDocument10 pagesMilares Inclinadosmaria jose peña rojasNo ratings yet
- Effects of The Jasper Jumper Appliance in TheDocument13 pagesEffects of The Jasper Jumper Appliance in TheRajesh MvNo ratings yet
- Interesting Eruption of 4 Teeth Associated With A Large Dentigerous Cyst in Mandible by Only MarsupializationDocument3 pagesInteresting Eruption of 4 Teeth Associated With A Large Dentigerous Cyst in Mandible by Only MarsupializationAnupama NagrajNo ratings yet
- Comparison of A New Flap Design With The Routinely Used Triangular Flap Design in Third Molar SurgeryDocument8 pagesComparison of A New Flap Design With The Routinely Used Triangular Flap Design in Third Molar SurgeryJean Carlos Barbosa FerreiraNo ratings yet
- Anchorage Loss - A Multifactorial Response: The Angle Orthodontist January 2004Document9 pagesAnchorage Loss - A Multifactorial Response: The Angle Orthodontist January 2004Thomas Karl QuilangNo ratings yet
- Clase II Division IDocument6 pagesClase II Division IAndres CoboNo ratings yet
- Resolving Mandibular Arch Discrepancy Through Utilization of Leeway SpaceDocument4 pagesResolving Mandibular Arch Discrepancy Through Utilization of Leeway Spacesaeed zaitonNo ratings yet
- Resolving Mandibular Arch Discrepancy Through Util PDFDocument4 pagesResolving Mandibular Arch Discrepancy Through Util PDFsaeed zaitonNo ratings yet
- Extraction or Nonextraction in Orthodontic Cases - A Review - PMCDocument6 pagesExtraction or Nonextraction in Orthodontic Cases - A Review - PMCManorama WakleNo ratings yet
- 2015 Pattern of Maxillary and Mandibular Proximal Enamel Thickness at The Contact Area of The Permanent Dentition From First Molar To First MolarDocument10 pages2015 Pattern of Maxillary and Mandibular Proximal Enamel Thickness at The Contact Area of The Permanent Dentition From First Molar To First MolarElías Enrique MartínezNo ratings yet
- Lagravere (2020) retrospectivCBCTDocument9 pagesLagravere (2020) retrospectivCBCTyeny valdivia albornozNo ratings yet
- Diagnostic Test: Visual ExaminationDocument51 pagesDiagnostic Test: Visual ExaminationDr.O.R.GANESAMURTHINo ratings yet
- Benedict Wimes, Mascara FacialDocument8 pagesBenedict Wimes, Mascara FacialjamilistccNo ratings yet
- Periodontal Plastic SurgeryDocument5 pagesPeriodontal Plastic Surgeryudhai170819No ratings yet
- International Journal of Medical and Health Sciences ResearchDocument10 pagesInternational Journal of Medical and Health Sciences ResearchEdwin FransiariNo ratings yet
- 3 Bishara1992Document13 pages3 Bishara1992Marcos CastroNo ratings yet
- Pain and Discomfort During The First Week of Maxillary Expansion Using Two Different Expanders - Patient-Reported Outcomes in A RCTDocument10 pagesPain and Discomfort During The First Week of Maxillary Expansion Using Two Different Expanders - Patient-Reported Outcomes in A RCTtanloonhanNo ratings yet
- Paper 1Document5 pagesPaper 1runit nangaliaNo ratings yet
- Interproximal Tooth Morphology and Its Effect On Plaque Removal. SmulklesDocument8 pagesInterproximal Tooth Morphology and Its Effect On Plaque Removal. SmulklesLuís ArturNo ratings yet
- 1 s2.0 S0889540622006552 MainDocument13 pages1 s2.0 S0889540622006552 MainMarcos Gómez SosaNo ratings yet
- Skeletal Width Changes After Mini-Implant-Assisted Rapid Maxillary Expansion (MARME) in Young AdultsDocument6 pagesSkeletal Width Changes After Mini-Implant-Assisted Rapid Maxillary Expansion (MARME) in Young AdultsRolando Huaman BravoNo ratings yet
- JCDP 19 515Document6 pagesJCDP 19 515jaslinshalinNo ratings yet
- 576 Ijar-2733 PDFDocument4 pages576 Ijar-2733 PDFruli nurul amanNo ratings yet
- Peri-Implant Complications: A Clinical Guide to Diagnosis and TreatmentFrom EverandPeri-Implant Complications: A Clinical Guide to Diagnosis and TreatmentNo ratings yet
- Maxillary and Mandibular Dentoalveolar Expansion With An Auxiliary Beta-Titanium ArchDocument11 pagesMaxillary and Mandibular Dentoalveolar Expansion With An Auxiliary Beta-Titanium ArchfarahNo ratings yet
- Fixed Versus Removable Appliance For Palatal Expansion A 3D Analysis Using The Finite Element MethodDocument11 pagesFixed Versus Removable Appliance For Palatal Expansion A 3D Analysis Using The Finite Element MethodfarahNo ratings yet
- Removable Orthodontic Appliances: New Perspectives On Capabilities and EfficiencyDocument7 pagesRemovable Orthodontic Appliances: New Perspectives On Capabilities and EfficiencyfarahNo ratings yet
- Topical and Systemic Therapies For Oral and Perioral Herpes Simplex Virus InfectionsDocument7 pagesTopical and Systemic Therapies For Oral and Perioral Herpes Simplex Virus InfectionsfarahNo ratings yet
- Two Cases of Recurrent Herpetic Infection of The TongueDocument5 pagesTwo Cases of Recurrent Herpetic Infection of The TonguefarahNo ratings yet
- Connect Insurance Brief Final E Version 29 January 2011Document4 pagesConnect Insurance Brief Final E Version 29 January 2011markleongoldber3215No ratings yet
- KrokodilDocument6 pagesKrokodilapi-252934043No ratings yet
- (Nursing Models in Action Series) Charleen Newton RGN, Dip - Nursing (Lond.) (Auth.) - The Roper-Logan-Tierney Model in Action-Macmillan Education UK (1991)Document221 pages(Nursing Models in Action Series) Charleen Newton RGN, Dip - Nursing (Lond.) (Auth.) - The Roper-Logan-Tierney Model in Action-Macmillan Education UK (1991)Sagun PandeyNo ratings yet
- Hiv in PregnancyDocument13 pagesHiv in Pregnancyapi-533578725No ratings yet
- 53 - Great Pacific Life Insurance v. CADocument1 page53 - Great Pacific Life Insurance v. CAperlitainocencioNo ratings yet
- Heliyon: Mayantoinette F. WatsonDocument8 pagesHeliyon: Mayantoinette F. WatsonabdalqaniNo ratings yet
- SOC 185 Final Exam Solutions AnswersDocument3 pagesSOC 185 Final Exam Solutions AnswersdanielNo ratings yet
- Military Police Officer Resume SampleDocument2 pagesMilitary Police Officer Resume Sampleresume7.com100% (2)
- Oral Hygiene InstructionsDocument20 pagesOral Hygiene Instructionsapi-307943695No ratings yet
- Final Sop Manual-1-1Document62 pagesFinal Sop Manual-1-1Dianne JoyNo ratings yet
- Excess Fluid Volume - Nursing Diagnosis & Care Plan - NurseslabsDocument8 pagesExcess Fluid Volume - Nursing Diagnosis & Care Plan - NurseslabsEricsonMitraNo ratings yet
- Light 27 Web FinalDocument28 pagesLight 27 Web FinalrafilhouseNo ratings yet
- 5.20 MSDS HTC NI 500 RP 1.2 MMDocument6 pages5.20 MSDS HTC NI 500 RP 1.2 MMMarsell StandhiNo ratings yet
- Minna 2013Document14 pagesMinna 2013Dr. B. M. LIMANNo ratings yet
- Risk Management in Food IndustryDocument17 pagesRisk Management in Food IndustryShyanyoon Teh100% (1)
- ĐỀ SỞ NAM ĐỊNH - LIVE CHỮA THỨ 4 NGÀY 03012024Document6 pagesĐỀ SỞ NAM ĐỊNH - LIVE CHỮA THỨ 4 NGÀY 03012024panow1037No ratings yet
- Iol Brochure 2023Document12 pagesIol Brochure 2023Shree TrivediNo ratings yet
- AsiaSpa India - 2016 March-AprilDocument190 pagesAsiaSpa India - 2016 March-AprilTa Hoang DinhNo ratings yet
- Chapter 4Document44 pagesChapter 4GGNo ratings yet
- Powers and Duties of Officers and Employees G.O.Ms - No.375 Animal Husbandry and Fisheries (AH-7) Department, Dated 13.07.1990Document7 pagesPowers and Duties of Officers and Employees G.O.Ms - No.375 Animal Husbandry and Fisheries (AH-7) Department, Dated 13.07.1990Patrick SaravananNo ratings yet
- Unit4 ADocument2 pagesUnit4 AsaraNo ratings yet
- Jurnal Mikroplastik 5Document18 pagesJurnal Mikroplastik 5bundazbNo ratings yet
- Medical Surgical Nursing Module 7Document18 pagesMedical Surgical Nursing Module 7weissNo ratings yet
- The Life and Culture of The Indigenous PeopleDocument2 pagesThe Life and Culture of The Indigenous PeopleJustine Airra OndoyNo ratings yet
- Iso 2210Document3 pagesIso 2210kirandevi1981No ratings yet
- Sains t2 PDFDocument6 pagesSains t2 PDFSJK CHUNG HUA 4 1/2 四哩半中公No ratings yet
- Promissory Note Promissory Note: Mauban District Hospital Mauban District HospitalDocument2 pagesPromissory Note Promissory Note: Mauban District Hospital Mauban District HospitalKC PalattaoNo ratings yet
- Class II Malocclusions Diagnostic and Clinical Considerations With and Without Treatment. Seminars in Orthodontics 12 (1) 11-24, Mar 2006. S. BisharaDocument14 pagesClass II Malocclusions Diagnostic and Clinical Considerations With and Without Treatment. Seminars in Orthodontics 12 (1) 11-24, Mar 2006. S. BisharaAhmad EgbariaNo ratings yet
- Abortion Reversal Pill - August 15 2020Document2 pagesAbortion Reversal Pill - August 15 2020api-271968502No ratings yet
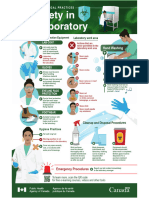
- Biosafety in The LaboratoryDocument1 pageBiosafety in The LaboratoryALFARO CHAT CARMINA ROSARIONo ratings yet