You might also like
- Sodium Fluoride PET/CT in Clinical UseFrom EverandSodium Fluoride PET/CT in Clinical UseKalevi KairemoNo ratings yet
- F-FDG Pet/Ct and I-Metaiodobenzylguanidine Imaging in High-Risk Neuroblastoma: Diagnostic Comparison and Survival AnalysisDocument7 pagesF-FDG Pet/Ct and I-Metaiodobenzylguanidine Imaging in High-Risk Neuroblastoma: Diagnostic Comparison and Survival AnalysisManos PanagiotidisNo ratings yet
- Diagnostic Value of F-FDG PET/CT in Paediatric Neuroblastoma: Comparison With I-MIBG ScintigraphyDocument7 pagesDiagnostic Value of F-FDG PET/CT in Paediatric Neuroblastoma: Comparison With I-MIBG ScintigraphyDhruv MahajanNo ratings yet
- Diagnostics 10 00663Document7 pagesDiagnostics 10 00663AdiNNo ratings yet
- Biomedicines 11 00128Document13 pagesBiomedicines 11 00128dmandatari7327No ratings yet
- F DOPA y Otros RF Pet en TNEDocument24 pagesF DOPA y Otros RF Pet en TNEMon Ti TaNo ratings yet
- I-MIBG in The Diagnosis of Primary and Metastatic NeuroblastomaDocument9 pagesI-MIBG in The Diagnosis of Primary and Metastatic NeuroblastomaAdiNNo ratings yet
- The Impact of PETCT On Paediatric OncologyDocument17 pagesThe Impact of PETCT On Paediatric OncologylkitkatgirlNo ratings yet
- 11C MetioninaDocument8 pages11C MetioninaPUIGCOZARNo ratings yet
- 10 1200@jco 20 00386Document12 pages10 1200@jco 20 00386rafaelskpkNo ratings yet
- Recent Advances in Radiological and Radionuclide Imaging and Therapy of Neuroendocrine TumoursDocument14 pagesRecent Advances in Radiological and Radionuclide Imaging and Therapy of Neuroendocrine TumoursrevanthNo ratings yet
- The Role of FDG-PET Scans in Patients With Lymphoma: Review in Translational HematologyDocument11 pagesThe Role of FDG-PET Scans in Patients With Lymphoma: Review in Translational HematologyPunam SinhaNo ratings yet
- 18F FDG PET CT Role in Staging of Gastric CancerDocument8 pages18F FDG PET CT Role in Staging of Gastric Cancermednuclpg mednuclpgNo ratings yet
- Craniotomy For Resection of Meningioma An Age Stratified AnalysisDocument7 pagesCraniotomy For Resection of Meningioma An Age Stratified Analysis49hr84j7spNo ratings yet
- Fluorine 18Document4 pagesFluorine 18Baby DragonNo ratings yet
- J Nucl Med-2009-Putzer-1214-21Document9 pagesJ Nucl Med-2009-Putzer-1214-21Madalina CordonasuNo ratings yet
- Pet Vs Mbgi NeuroblastomaDocument12 pagesPet Vs Mbgi NeuroblastomaItzia VerduzcoNo ratings yet
- TrialllDocument13 pagesTriallljunin_tim4619No ratings yet
- PET in MMDocument8 pagesPET in MMdanishNo ratings yet
- CRITERIOSUSOGA68Document9 pagesCRITERIOSUSOGA68Belen Fdez LlanaNo ratings yet
- Current Radiopharmaceuticals For Positron Emission Tomography of Brain TumorsDocument7 pagesCurrent Radiopharmaceuticals For Positron Emission Tomography of Brain TumorsAl KutbiNo ratings yet
- Jurnal Kanker TiroidDocument6 pagesJurnal Kanker TiroidEkfatil MardiyahNo ratings yet
- New Guidelines For Somatostatin ReceptorsDocument9 pagesNew Guidelines For Somatostatin ReceptorssatyaNo ratings yet
- FDG PET-CT in The Initial Staging and Restaging of Soft Tissue or Bone Sarcoma.Document7 pagesFDG PET-CT in The Initial Staging and Restaging of Soft Tissue or Bone Sarcoma.Anderson Ruben LizcanoNo ratings yet
- FTPDocument5 pagesFTPriezkytrinawatiNo ratings yet
- ch18 6 PDFDocument12 pagesch18 6 PDFomkarNo ratings yet
- PET-CT Radiomics in Breast Cancer - Promising Tool For PredictionDocument10 pagesPET-CT Radiomics in Breast Cancer - Promising Tool For Predictionmazda626 retrocarsNo ratings yet
- Validation of The Meet URO Score in Patients WithDocument9 pagesValidation of The Meet URO Score in Patients Withveaceslav coscodanNo ratings yet
- Cancers 15 00364 v2Document16 pagesCancers 15 00364 v2Raul Matute MartinNo ratings yet
- J Nucl Med-1997-Valdés Olmos-873-9Document8 pagesJ Nucl Med-1997-Valdés Olmos-873-9Mădălina VargaNo ratings yet
- PSMADocument10 pagesPSMADiego GavilanesNo ratings yet
- Nuclear Medicine Imaging in Neuroblastoma: Current Status and New DevelopmentsDocument22 pagesNuclear Medicine Imaging in Neuroblastoma: Current Status and New DevelopmentsAdiNNo ratings yet
- 1 s2.0 S2588931120300900 MainDocument10 pages1 s2.0 S2588931120300900 MainMiro SpiroNo ratings yet
- WBRT Plus SIB With Image Guided Intensity-Modulated Radiotherapy For Multiple Brain MetastasesDocument2 pagesWBRT Plus SIB With Image Guided Intensity-Modulated Radiotherapy For Multiple Brain Metastasessanti lestariNo ratings yet
- 68Ga-DOTATATE PET-Based Radiation Contouring Creates More Precise Radiation Volumes For Patients With MeningiomaDocument7 pages68Ga-DOTATATE PET-Based Radiation Contouring Creates More Precise Radiation Volumes For Patients With MeningiomaandresNo ratings yet
- Artigo de Pet No Monitoramento Precoce Do LinfomaDocument7 pagesArtigo de Pet No Monitoramento Precoce Do LinfomagustavoandradeambrosioNo ratings yet
- JCO 2019 MRD Phéno Myélome PDFDocument20 pagesJCO 2019 MRD Phéno Myélome PDFTony HuynhNo ratings yet
- 10.1007@s00259 019 04298 4Document7 pages10.1007@s00259 019 04298 4CamilleNo ratings yet
- The Place of FDG PET CT in Renal Cell Carcinoma - Value and LimitationsDocument7 pagesThe Place of FDG PET CT in Renal Cell Carcinoma - Value and LimitationslkitkatgirlNo ratings yet
- Diffusion Tensor Imaging, Intra-Operative Neurophysiological Monitoring and Small Craniotomy: Results in A Consecutive Series of 103 GliomasDocument11 pagesDiffusion Tensor Imaging, Intra-Operative Neurophysiological Monitoring and Small Craniotomy: Results in A Consecutive Series of 103 GliomasGeneration GenerationNo ratings yet
- Comparison of 18FDGPETCT and 18FFDGPETMR in Head and Neck 2017Document13 pagesComparison of 18FDGPETCT and 18FFDGPETMR in Head and Neck 2017Victor Alfonso Martinez DiazNo ratings yet
- Gandaglia 2018Document9 pagesGandaglia 2018Arlett Karina Juarez RivasNo ratings yet
- Gandaglia2018 PDFDocument9 pagesGandaglia2018 PDFArlett Karina Juarez RivasNo ratings yet
- Clinical Hepatology: AbstractsDocument2 pagesClinical Hepatology: AbstractssmallheartNo ratings yet
- Intra Individual Comparison of 18F PSMA1007 and 18F-FDG PETCT in The Evaluation of Patients With Prostate CancerDocument8 pagesIntra Individual Comparison of 18F PSMA1007 and 18F-FDG PETCT in The Evaluation of Patients With Prostate CancerJoaquín Escobar FloresNo ratings yet
- JCO 2014 Stary 174 84Document12 pagesJCO 2014 Stary 174 84Ljubisa SavicNo ratings yet
- Neuro OncologyDocument10 pagesNeuro OncologylarissaNo ratings yet
- Clinical Impact of FDG PET-CT On Management Decisions For Patients With Primary Biliary TumoursDocument10 pagesClinical Impact of FDG PET-CT On Management Decisions For Patients With Primary Biliary TumourslkitkatgirlNo ratings yet
- Update On Neuroimaging in Brain Tumours: ReviewDocument8 pagesUpdate On Neuroimaging in Brain Tumours: ReviewYo MismoNo ratings yet
- Letter From The Editors - 2023 - Seminars in Nuclear MedicineDocument2 pagesLetter From The Editors - 2023 - Seminars in Nuclear MedicinePuig CozarNo ratings yet
- Pet ManejoDocument9 pagesPet ManejodrmolinammNo ratings yet
- Magnetic Resonance Imaging - 2023 - Zhang - Artificial Intelligence Applications in Glioma With 1p 19q Co Deletion ADocument15 pagesMagnetic Resonance Imaging - 2023 - Zhang - Artificial Intelligence Applications in Glioma With 1p 19q Co Deletion AMarcNo ratings yet
- Prevalence and Outcomes of Cardiac Amyloidosis in All-Comer Referrals For Bone ScintigraphyDocument6 pagesPrevalence and Outcomes of Cardiac Amyloidosis in All-Comer Referrals For Bone ScintigraphyNadia DuarteNo ratings yet
- Association Between A CTGF Gene Polymorphism andDocument8 pagesAssociation Between A CTGF Gene Polymorphism andAhmad ShamyNo ratings yet
- Ugc Carelist Journals 22novDocument7 pagesUgc Carelist Journals 22novnaresh kotraNo ratings yet
- Neurosurg Focus Article PE4Document8 pagesNeurosurg Focus Article PE4emilyNo ratings yet
- Vander Gee STDocument2 pagesVander Gee STWong Wen JianNo ratings yet
- Chemotherapy Response Evaluation in Metastatic Colorectal Cancer With FDG PET/CT and CT ScansDocument6 pagesChemotherapy Response Evaluation in Metastatic Colorectal Cancer With FDG PET/CT and CT ScansBagus OkaNo ratings yet
- Abordaje de Los Nodulos Pulmonares Indeterminados en El Tamizaje de Cancer de Pulmon Estudio Con PET CTDocument6 pagesAbordaje de Los Nodulos Pulmonares Indeterminados en El Tamizaje de Cancer de Pulmon Estudio Con PET CTAnaNo ratings yet
- Protocol SummaryDocument2 pagesProtocol Summaryapi-642376263No ratings yet
- Tropicalmed 05 00112 v4Document22 pagesTropicalmed 05 00112 v4IchaNo ratings yet
- Tropicalmed 05 00112 v4Document22 pagesTropicalmed 05 00112 v4IchaNo ratings yet
- The Solid Core (Trephine) Bone Marrow Biopsy Needle Advantages of Employing A Biopsy Needle With Core Retention DesignDocument5 pagesThe Solid Core (Trephine) Bone Marrow Biopsy Needle Advantages of Employing A Biopsy Needle With Core Retention DesignIchaNo ratings yet
- Tropicalmed 05 00112 v4Document22 pagesTropicalmed 05 00112 v4IchaNo ratings yet
- Medicine: Clinical Trial/Experimental StudyDocument10 pagesMedicine: Clinical Trial/Experimental StudyIchaNo ratings yet
- Pharmaceutics 12 00210 v2Document10 pagesPharmaceutics 12 00210 v2IchaNo ratings yet
- Predicting Frequent Asthma Exacerbations Using BloDocument13 pagesPredicting Frequent Asthma Exacerbations Using BloIchaNo ratings yet
- Tropicalmed 05 00112 v4Document22 pagesTropicalmed 05 00112 v4IchaNo ratings yet
- Peds 2018-3475 FullDocument30 pagesPeds 2018-3475 FullIchaNo ratings yet
- جورنال جاهزDocument4 pagesجورنال جاهزasrd ramiNo ratings yet
- Medicine: Clinical Trial/Experimental StudyDocument10 pagesMedicine: Clinical Trial/Experimental StudyIchaNo ratings yet
- Urine Cathecolamine Levels As Diagnostic Markers For Neuroblastoma in An Defined Population Implication For Ophthalmic PracticeDocument7 pagesUrine Cathecolamine Levels As Diagnostic Markers For Neuroblastoma in An Defined Population Implication For Ophthalmic PracticeIchaNo ratings yet
- Jurnal Hemato 7Document8 pagesJurnal Hemato 7IchaNo ratings yet
- Jurnal Hemato 8Document13 pagesJurnal Hemato 8IchaNo ratings yet
- Comparisons of The Accuracy of Radiation.5Document8 pagesComparisons of The Accuracy of Radiation.5IchaNo ratings yet
- Done - EDITED-HOPE1 - q1 - Mod5 - ObservesPersonalSafetyProtocolDocument21 pagesDone - EDITED-HOPE1 - q1 - Mod5 - ObservesPersonalSafetyProtocolVivencio Pascual JrNo ratings yet
- Handwashing ProposalDocument2 pagesHandwashing ProposalLevyCastilloNo ratings yet
- Road Traffic Accident: Purpose of Medico-Legal InvestigationDocument33 pagesRoad Traffic Accident: Purpose of Medico-Legal InvestigationAmirul AminNo ratings yet
- Enicillin-Like Antibiotics. Diarrhea, Nausea, Vomiting, HeadacheDocument5 pagesEnicillin-Like Antibiotics. Diarrhea, Nausea, Vomiting, HeadachePauline AñesNo ratings yet
- MEMO - RV RTPCR - MergedDocument5 pagesMEMO - RV RTPCR - MergedMukesh KumarNo ratings yet
- Melba Case Scenario FinalDocument34 pagesMelba Case Scenario FinalAlex Antiporda50% (2)
- Katsuura Et Al (2020) Overlapping, Masquerading, and Causative Cervical Spine and Shoulder Pathology2Document14 pagesKatsuura Et Al (2020) Overlapping, Masquerading, and Causative Cervical Spine and Shoulder Pathology2Miguel Jimenez AlvarezNo ratings yet
- Soal Ujian SekolahDocument47 pagesSoal Ujian SekolahClemens JasonNo ratings yet
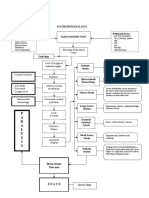
- Pathophysiology: P A R A L Y S I SDocument1 pagePathophysiology: P A R A L Y S I SJordan Garcia AguilarNo ratings yet
- HEALTH-GROUP MEDICLAIM June 2021Document61 pagesHEALTH-GROUP MEDICLAIM June 2021Kishore mohan ManapuramNo ratings yet
- Hyperglycemia Algorithm 2Document1 pageHyperglycemia Algorithm 2damondouglasNo ratings yet
- CHN Health Care Process PDFDocument9 pagesCHN Health Care Process PDFKathleen AngNo ratings yet
- Ingles Parcial Domiciliario 2022Document5 pagesIngles Parcial Domiciliario 2022Macarena zapattaNo ratings yet
- Impaired Posture and MovementDocument40 pagesImpaired Posture and MovementMohamed Magdy ElMeligieNo ratings yet
- Executive Technical Report SHCC 2023Document44 pagesExecutive Technical Report SHCC 2023abdelrahim basheerNo ratings yet
- Family TiesDocument8 pagesFamily TiesCristina Ioana NistorNo ratings yet
- CBC Arikod HoimaDocument37 pagesCBC Arikod Hoimadaniel arikodNo ratings yet
- ECG InterpretationDocument6 pagesECG InterpretationANDREW DEL ROSARIONo ratings yet
- Module 1 in TLE 9 WK 1 2nail CareDocument10 pagesModule 1 in TLE 9 WK 1 2nail CareAdrian AgaNo ratings yet
- 010303A TCCC-MP Tactical Field Care #1 IG 160603Document43 pages010303A TCCC-MP Tactical Field Care #1 IG 160603herralainNo ratings yet
- Life Span Development 16th Edition Santrock Test BankDocument31 pagesLife Span Development 16th Edition Santrock Test Bankbrandoncoletjaxprigfm100% (36)
- Seven Senses Chakra GuideDocument11 pagesSeven Senses Chakra GuidemhliuNo ratings yet
- Nejmoa2035389 ProtocolDocument307 pagesNejmoa2035389 ProtocolRadu FloreaNo ratings yet
- FOLK MEDICINE ExtraDocument22 pagesFOLK MEDICINE ExtraPaul SavvyNo ratings yet
- Covid-19 Ag Rapid Test: OnsiteDocument2 pagesCovid-19 Ag Rapid Test: OnsiteBPG ServiceNo ratings yet
- Falla Cardiaca Consenso 2021Document27 pagesFalla Cardiaca Consenso 2021Medico SantacruzNo ratings yet
- Safety Profile of Rotavac: Observational Prospective StudyDocument7 pagesSafety Profile of Rotavac: Observational Prospective StudyMalook Sekhon100% (1)
- The Art of Surgery: The Strange World of The Placebo ResponseDocument4 pagesThe Art of Surgery: The Strange World of The Placebo ResponseTamsin Athalie NicholsonNo ratings yet
- Handbook of Infant Mental Health Fourth Edition 4th Edition Ebook PDFDocument61 pagesHandbook of Infant Mental Health Fourth Edition 4th Edition Ebook PDFjeffrey.stanton398100% (41)
- 10 Penyakit Terbanyak Di Rawat Jalan Di Puskesmas Provinsi Dki Jakarta TW I Tahun 2019Document9 pages10 Penyakit Terbanyak Di Rawat Jalan Di Puskesmas Provinsi Dki Jakarta TW I Tahun 2019Klinik pratama Iqra' medical centreNo ratings yet